
Abstract
Background: There is increasing demand for managing depressive and/or anxiety disorders among primary care patients. Problem-solving therapy (PST) is a brief evidence- and strength-based psychotherapy that has received increasing support for its effectiveness in managing depression and anxiety among primary care patients.
Methods: We conducted a systematic review and meta-analysis of clinical trials examining PST for patients with depression and/or anxiety in primary care as identified by searches for published literature across 6 databases and manual searching. A weighted average of treatment effect size estimates per study was used for meta-analysis and moderator analysis.
Results: From an initial pool of 153 primary studies, 11 studies (with 2072 participants) met inclusion criteria for synthesis. PST reported an overall significant treatment effect for primary care depression and/or anxiety (d = 0.673; P < .001). Participants' age and sex moderated treatment effects. Physician-involved PST in primary care, despite a significantly smaller treatment effect size than mental health provider only PST, reported an overall statistically significant effect (d = 0.35; P = .029).
Conclusions: Results from the study supported PST's effectiveness for primary care depression and/or anxiety. Our preliminary results also indicated that physician-involved PST offers meaningful improvements for primary care patients' depression and/or anxiety.
Depressive and anxiety disorders are the 2 leading global causes of all nonfatal burden of disease1 and the most prevalent mental disorders in the US primary care system.2⇓–4 The proportion of primary care patients with a probable depressive and/or anxiety disorder ranges from 33% to 80%2,5,6; primary care patients also have alarmingly high levels of co-/multi-morbidity of depressive, anxiety, and physical disorders.7 Depression and anxiety among primary care patients contribute to: poor compliance with medical advice and treatment8; deficits in patient–provider communication9; reduced patient engagement in healthy behaviors10; and decreased physical wellbeing.11,12 Given the high prevalence of primary care depression and anxiety, and their detrimental effects on the qualities of primary care treatments and patients' wellbeing, it is important to identify effective interventions suitable to address primary care depression and anxiety.
Primary care patients with depression and/or anxiety are often referred out to specialty mental health care.13,14 However, outcomes from these referrals are usually poor due to patients' poor adherence and their resistance to mental health treatment15,16. Therefore, it is critical to identify effective mental health interventions that can be delivered in primary care for patients' depression and/or anxiety.17,18 During the past decade, a plethora of clinical trials have investigated different mental health interventions for depression and anxiety delivered in primary care. One of the most promising interventions that has received increasing support for managing depression and anxiety in primary care is Problem-Solving Therapy (PST).
PST
Holding that difficulties with problem solving make people more susceptible to depression, PST is a nonpharmacological, competence-based intervention that involves a step-by-step approach to constructive problem solving.19,20 Developed from cognitive-behavioral-therapy, PST is a short-term psychotherapy approach delivered individually or in group settings. The generic PST manual19 contains 14 training modules that guides PST providers working with patients from establishing a therapeutic relationship to identifying and understanding patient-prioritized problems; from building problem-solving skills to eventually solving the problems. Focused on patient problems in the here-and-now, a typical PST treatment course ranges from 7 to 14 sessions and can be delivered by various health care professionals such as physicians, clinical social workers or nurse practitioners. Because the generic PST manual outlines the treatment formula in detail, providers may deliver PST after receiving 1 month of training. For example, 1 feasibility study on training residents in PST found that residents can provide fidelious PST after 7 weeks' training and reach moderate to high competence after 3 years of practicing PST.21 PST also has a self-help manual available to clients when needed.
PST is a well-established, evidence-based intervention for depression in specialty mental health care and is receiving greater recognition for its effectiveness in treating depression and anxiety in primary care. Systematic and meta-analytic reviews of PST for depression consistently reported moderate to large treatment effects, ranging from d = 0.4 to d = 1.15.22⇓–24 Several clinical trials indicated PST's clinical effectiveness in alleviating anxiety as well.25,26 Most importantly, PST has been adapted for primary care settings (PST-PC) and can be delivered by a variety of health care providers with fewer number of sessions and shorter session length. These unique features make PST(-PC) an ideal psychotherapy for depressive and/or anxiety disorders in primary care.
Previous reviews of PST focused on its effectiveness for depression care, but with little attention to PST's effect on anxiety or comorbid depression anxiety. In addition, to our knowledge, no previous reviews of PST have focused on managing depressive and/or anxiety disorders in primary care. Although research demonstrates that PST has a strong evidence base for treating depression and/or anxiety in specialty mental health care settings, more research is needed to determine whether PST remains effective for treating depressive and/or anxiety disorders when delivered in primary care. To address this gap, we conducted a systematic review and meta-analysis on the effectiveness of PST for treating depressive and/or anxiety disorders with primary care patients.
Methods
Search Strategies
This review included searches in 6 electronic databases (Academic Search Complete, CINAHL, Medline, PsychINFO, PUBMED, and the Cochrane Library/Database) and 3 professional Web sites (Academy of Cognitive Therapy, IMPACT, Anxiety and Depression Association of America) for primary care depression and anxiety studies published between January 1900 and September 2016. We also E-mailed major authors of PST studies for feedback and input. Search terms of title and/or abstract searches included: [“PST” or “Problem-Solving Therapy” or “Problem Solving Therapy” or “Problem Solving”] AND [“Depression” or “Depressive” or “Anxiety” or “Panic” or “Phobia”] AND [“primarycare” or “primary care” or “PCP” or “Family Medicine” or “Family Doctor”]. We supplemented the procedure described above with a manual search of study references.
Eligibility Criteria
For inclusion in analyses, a study needed to be 1) a randomized-controlled-trial of 2) PST for 3) primary care patients' 4) depressive and/or anxiety disorders. For studies that examined face-to-face, in-person PST, the intervention must be delivered in primary care for inclusion. If studies examined tele-PST (eg, telephone delivery, video conferencing, computer-based), the intervention must be connected to patients' primary care services for a study to be included. For example, when a primary care physician prescribed computer-based PST at home for their patients, the study met inclusion criteria (as it was still considered managing depression “in primary care” in the present review). However, studies would be excluded if a primary care physician referred patients to an external mental health intervention. Finally, studies must document and report sufficient statistical information for calculating effect size for inclusion in the final analysis.
Data Abstraction and Coding
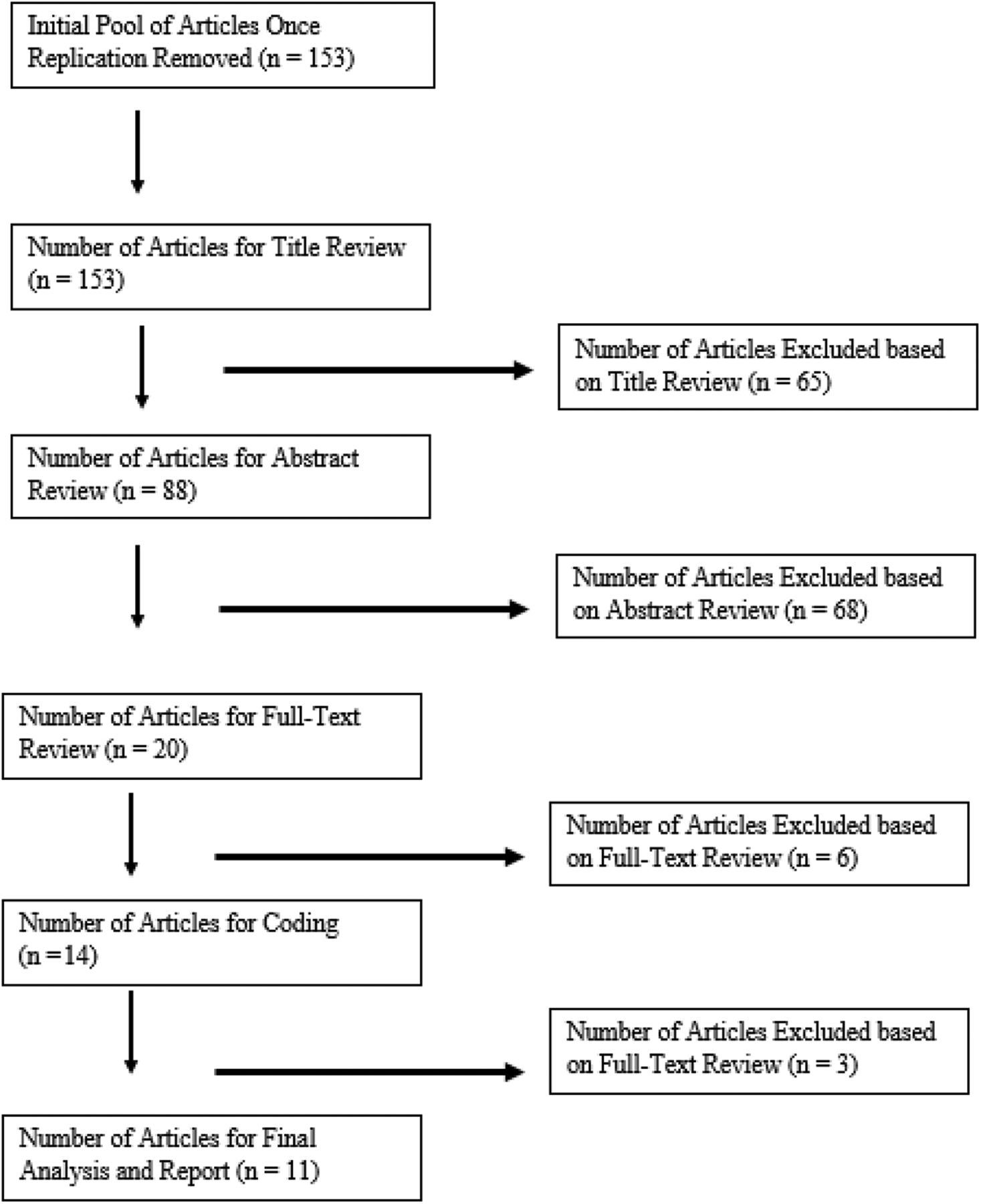
Two authors (AZ and JES) reviewed an initial pool of 153 studies and agreed to remove 65 studies based on title and 68 studies based on abstract, resulting in 20 studies for full-text review. To develop the final list, we excluded 6 studies after closer review of full-text and consultation with a third reviewer who is an established PST researcher. Lastly, we excluded 2 studies due to 1) a study with a design that blurred the effect of PST with other treatments and 2) unsuccessful contact with a study author to request data needed for calculating effect size. We used a final sample of 11 studies for meta-analysis. The PRISMA chart is presented in Figure 1.

Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) chart of literature search for Problem-solving therapy (PST) studies for treating primary care patients' depression and/or anxiety.
Statistical Analysis
This study conducted meta-analysis with the following procedures: 1) calculated a weighted average of effect size estimates per study for depression and anxiety separately (to ensure independence)27; 2) synthesized an overall treatment effect estimate using fixed- or random-effects model based on a heterogeneity statistic (Q-statistic)28; and 3) performed univariate meta-regression with a mixed-effects model for moderator analysis.29 Although other more advanced statistical approaches allow inclusion of multiple treatment effect size estimates per study for data synthesis, like the Generalized Least Squares method30 or the Robust Variance Estimation method31, this study employed a typical approach because of the relatively small sample and absence of study information required to conduct more advanced methods. Following procedures outlined by Cooper and colleagues32, we conducted all analyses with R software.33 We chose to conduct analyses in R, rather than software specific to meta-analysis (eg, RevMan), because R allowed for more flexibility in statistical modeling (eg, small sample size correction).34 Sensitivity analysis using Robust Variance Estimation did not significantly alter results estimated with the typical approach. And so this study presents results from only the typical approach for purposes of parsimony and clarity.
Publication Bias, Risk of Bias and Quality of Studies
To detect publication bias, we used a funnel plot of effect size estimates graphed against their standard errors for visual investigation. To evaluate risk of bias, we used the Cochrane Collaboration's tool for assessing risk of bias in randomized trials35 and the Quality Assessment of Controlled Intervention Studies to evaluate study quality.36
Results
Primary Studies
Eleven PST studies for primary care depression and/or anxiety reported a total sample size of 2072 participants. Participants' age averaged 50.1 and ranged from 24.5 to 71.8 years old. Ten studies reported participants' sex with an average of 35.6% male participants across all studies. Seven studies (63.6%) reported participants' racial background with most identified as non-Hispanic white (83.6%). Other racial/ethnic groups were poorly reported for meaningful summary. Five studies used active medication as a comparison, including 3 studies that used both active medication and placebo medication. The rest compared PST with treatment-as-usual while 2 studies used active control group (eg, video education material). Four studies involved physicians in some component of intervention delivery. PCPs provided PST in 2 studies; supervised and collaborated with depression care manager in 1 study, and collaborated with a primary care nurse in another. Ten studies reported an average of 6 PST sessions (M = 6.1) ranging from 3 to 12 sessions. All but 1 study (n = 10) used individual PST and 2 studies used tele-health modalities to provide PST. All studies used standardized measures of depression and anxiety. Examples of the most common measures included: PHQ-9, CES-D, HAM-D, and BDI-II. Table 1 presents a detailed description of study characteristics.
Study Characteristics for Problem-Solving Therapy as Intervention for Treating Depression and/or Anxiety Among Primary Care Patients (n = 11)
Publication Bias, Risk of Bias, and Quality of Studies
The funnel plot (Figure 2) did not indicate any clear sign of publication bias. Risk of bias (Table 4) indicated an overall acceptable risk across studies included for review with blinding of participants and personnel, blinding of outcome assessment and incomplete outcome data most vulnerable to risk of bias. Quality of study assessment (Table 5) indicated an overall satisfactory study quality with over half of studies (n = 6) achieving ratings of “Good” study quality.

Funnel Plot for Publication Bias in Problem-solving therapy (PST) Studies for Treating Primary Care Patients' Depression an/or Anxiety.
Meta-analysis and moderator analysis
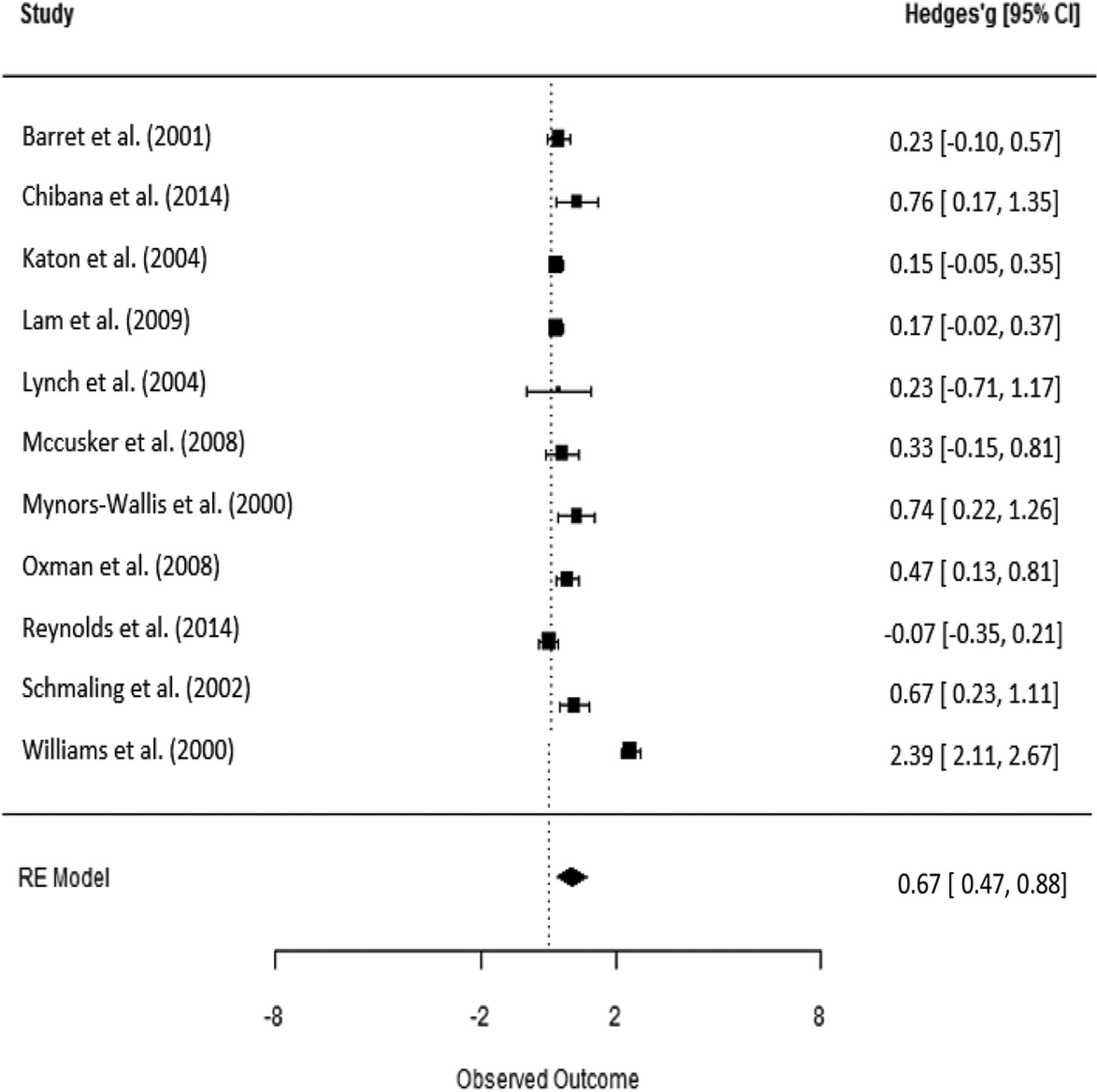
Figure 3 presents a forest plot of treatment effects per study, including depression and anxiety measures. Table 3 presents subgroup analysis of overall treatment effect by moderator and Table 2 presents the results of meta-analysis and moderator analysis. Meta-analysis revealed an overall significant treatment effect of PST for primary care depression and/or anxiety (d = 0.67; P < .001). Further investigation revealed no significant difference between the mean treatment effect of PST for depression versus anxiety in primary care (d(diff.) = −0.25; P = .317) while subgroup analysis revealed the overall treatment effect for anxiety was not significant (d = 0.35; P = .226). Age was found to be a significant moderator (β1 = 0.02; P = .012) for treatment outcomes, indicating that for each unit increase in participants' age, the overall treatment effect for primary are depression and/or anxiety are expected to increase by 0.02 (standard deviations). Neither participants' ethnic or racial backgrounds nor marital status significantly moderated the overall treatment outcome.
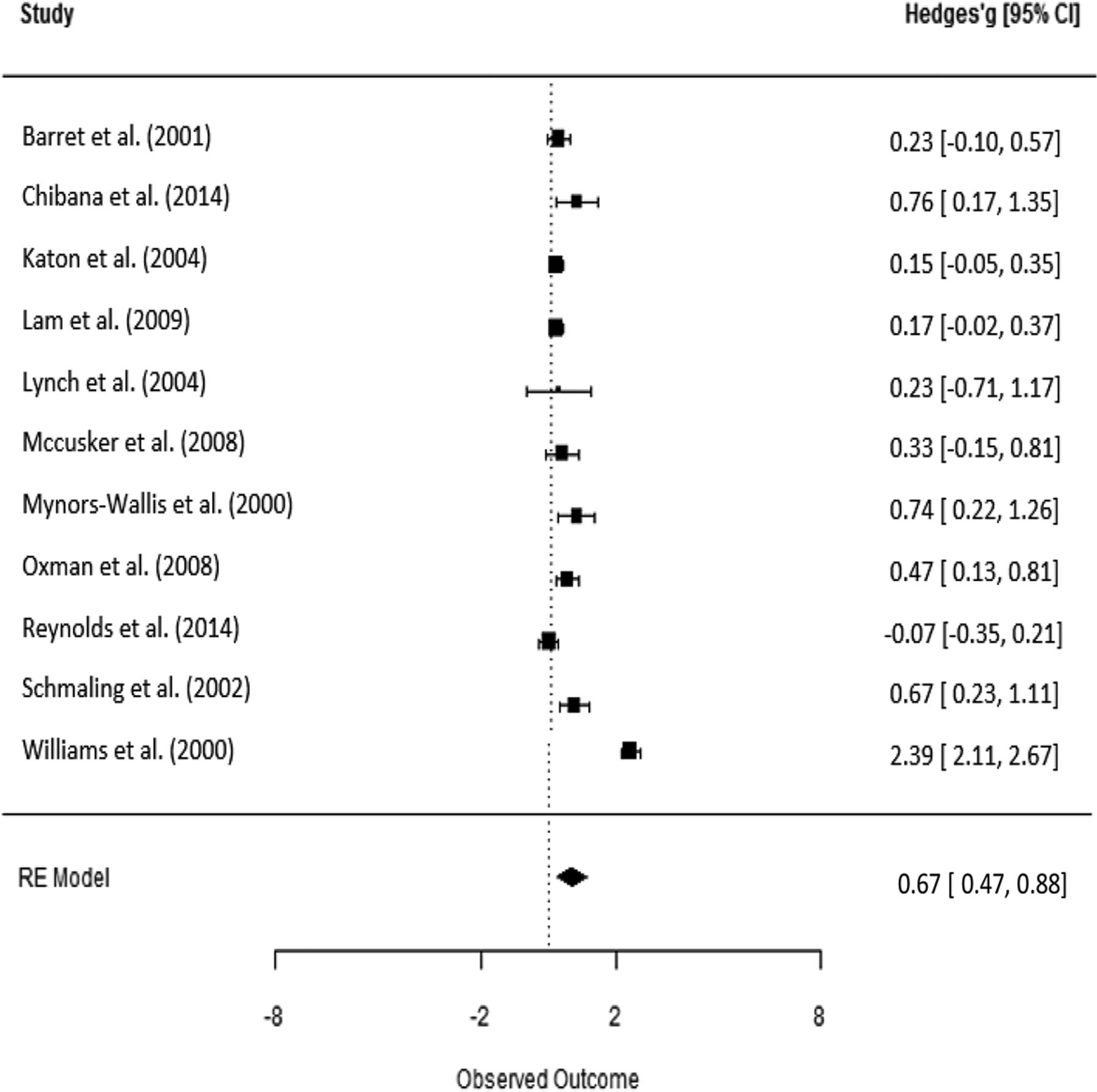
Forest Plot of PST Treatment Effect Size Estimates for Treating Primary Care Patients' Depression and/or Anxiety per Study.
PST for Treating Primary Care Patients' Depression and/or Anxiety; Results of Univariate Meta-regression
Results of Subgroup Analysis of Overall Treatment Effect (by Moderator) of PST for Treating Primary Care Patients' Depression and/or Anxiety
PST for Treating Primary Care Patients' Depression and/or Anxiety; Results of the Cochrane Collaboration's Tool for Assessing Risk of Bias*
Quality Assessment of Controlled PST Intervention Studies for Primary Care Patients' Depression and/or Anxiety (n=11)
The overall treatment effect was not moderated by any treatment characteristics including: treatment modality (individual vs group PST), delivery methods (face-to-face vs tele-health PST), number of PST sessions and length of individual PST sessions. Subgroup analysis indicated an overall significant treatment effect of in-person PST (d = 0.72; P < .001) but not of tele-PST (d = 0.53; P = .097). However, the difference between the 2 was not statistically significant.
PST providers background and primary care physician's involvement significantly moderated the overall treatment effect size. Master's-level providers reported an overall treatment effect (d = 1.57; P < .001) significantly higher than doctoral-level providers (d = −1.33; P = .007). Both physician-involved and nonphysician involved PST reported significant overall treatment effect of PST for depression and/or anxiety in primary care (d = 1.06; P < .001 and d = 0.35; P = .029, respectively). Moderator analysis further revealed that PST without physician involvement reported significantly greater treatment effects compared with physician-involved PST in primary care (d = −0.71; P = .005). Results of subgroup and moderator analyses indicated that while the difference (in treatment effect) between physician and nonphysician involved PST in primary care were statistically significant, physician-involved PST was also statistically significant, thus practically meaningful.
Discussion
Results of the study demonstrated a statistically significant overall treatment effect in outcomes of depression and/or anxiety for primary care patients receiving PST compared with patients in control groups. The outcome type—depression versus anxiety—failed to moderate treatment effect; only PST for depression reported a significant overall effect size. This could indicate that many studies primarily targeted depression and included anxiety measures as secondary outcomes. For this reason, we expect to find a greater treatment effect for primary care depression. It was unsurprising that treatment characteristics failed to moderate treatment effect size because most primary studies used PST-PC or its modified version; there was insufficient variation between studies (and moderators), yielding insignificant moderating coefficients.
Although delivery method did not moderate treatment effect reported in studies included in this review, significant effect was only reported by studies using face-to-face in-person PST but not by those with tele-PST modalities (n = 2). Although evidence for the effectiveness of tele-PST is established or increasing in a variety of settings37⇓–39 most PST studies for primary care patients have used face-to-face, in-person PST. Our study further supported the use of face-to-face in-person PST for treating depression and anxiety among primary care patients. We recognize, however, that current and projected shortages in specialty mental health care provision, felt acutely in subspecialties such as geriatric mental health, necessitate more trials with PST tele-health modalities.40
It is salient to note that, while nonphysician-involved PST studies reported significantly greater treatment effect than those involving physicians, PCP-involved studies also reported an overall significant effect size. Closer examination indicated that studies with physician-involved PST were either delivered by physicians or other nonmental health professionals (eg, registered nurses or depression care managers). Lack of sufficient PST training might explain the difference in treatment effect sizes being statistically significant. Yet, the fact that physician-involved PST studies reported an overall statistically significant effect size for primary care depression and/or anxiety suggested a meaningful treatment effect for clinical practice. When faced with a shortage of mental health professionals (eg, psychologists, clinical social workers, licensed professional counselors), our findings suggest physician-led or -supervised PST interventions could still improve primary care patients' depression and/or anxiety. Researchers are encouraged to further examine the treatment effect of PST delivered by mental health professionals in collaboration with primary care physicians.
Limitation
This study has several weaknesses that are inherent to meta-analyses. There is no way to assure we included all studies despite adopting a comprehensive search and coding strategy (ie, file drawer problem). Second, while all studies in this meta-analysis seemed to have satisfactory methodological rigor, it is possible that internal biases within some studies may influence results. This study takes a quantitative meta-analysis approach which inherently neglects other study designs and methodologies that also provide valuable information about the effectiveness, feasibility, and acceptability of PST for treating primary care patients with depression. To ensure independence of data, this study used a weighted average of effect size estimates per study in synthesizing an overall treatment effect and conducting moderator analysis. While sensitivity analysis did not reveal significant differences from the reported results, we will not know for sure how our choice of statistical method might affect the results.
Acknowledgments
The authors are grateful to Dr. Namkee Choi, Professor and the Louis and Ann Wolens Centennial Chair in Gerontology at the University of Texas at Austin Steve Hicks School of Social Work, for her mentorship and insightful comments during preparation of the manuscript.
Notes
This article was externally peer reviewed.
Funding: none.
Conflict of interest: none declared.
Ethics Review: This is a systematic review and meta-analysis based on de-identified aggregate study data. No human participants or animals were involved in this study. No ethics review was required.
To see this article online, please go to: http://jabfm.org/content/31/1/139.full.
- Received for publication July 5, 2017.
- Revision received September 14, 2017.
- Accepted for publication September 27, 2017.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Global health reciprocal innovation to address mental health and well-being: strategies used and lessons learnt
- Psychologic Treatment of Depression Compared With Pharmacotherapy and Combined Treatment in Primary Care: A Network Meta-Analysis
- Brief behaviour change strategies for distressed patients in primary care
- Interventions Must Be Realistic to Be Useful and Completed in Family Medicine