
Article Figures & Data
Figures
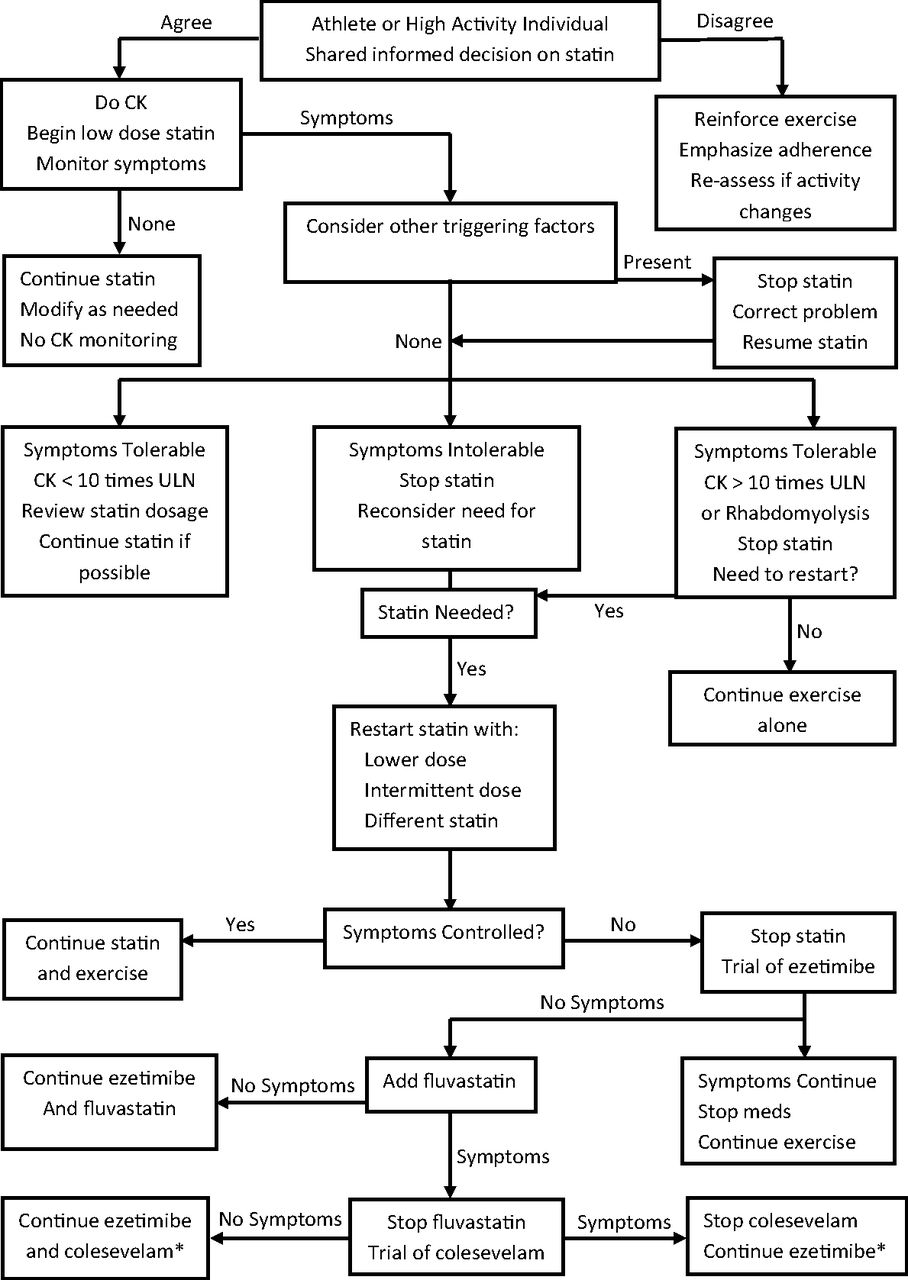
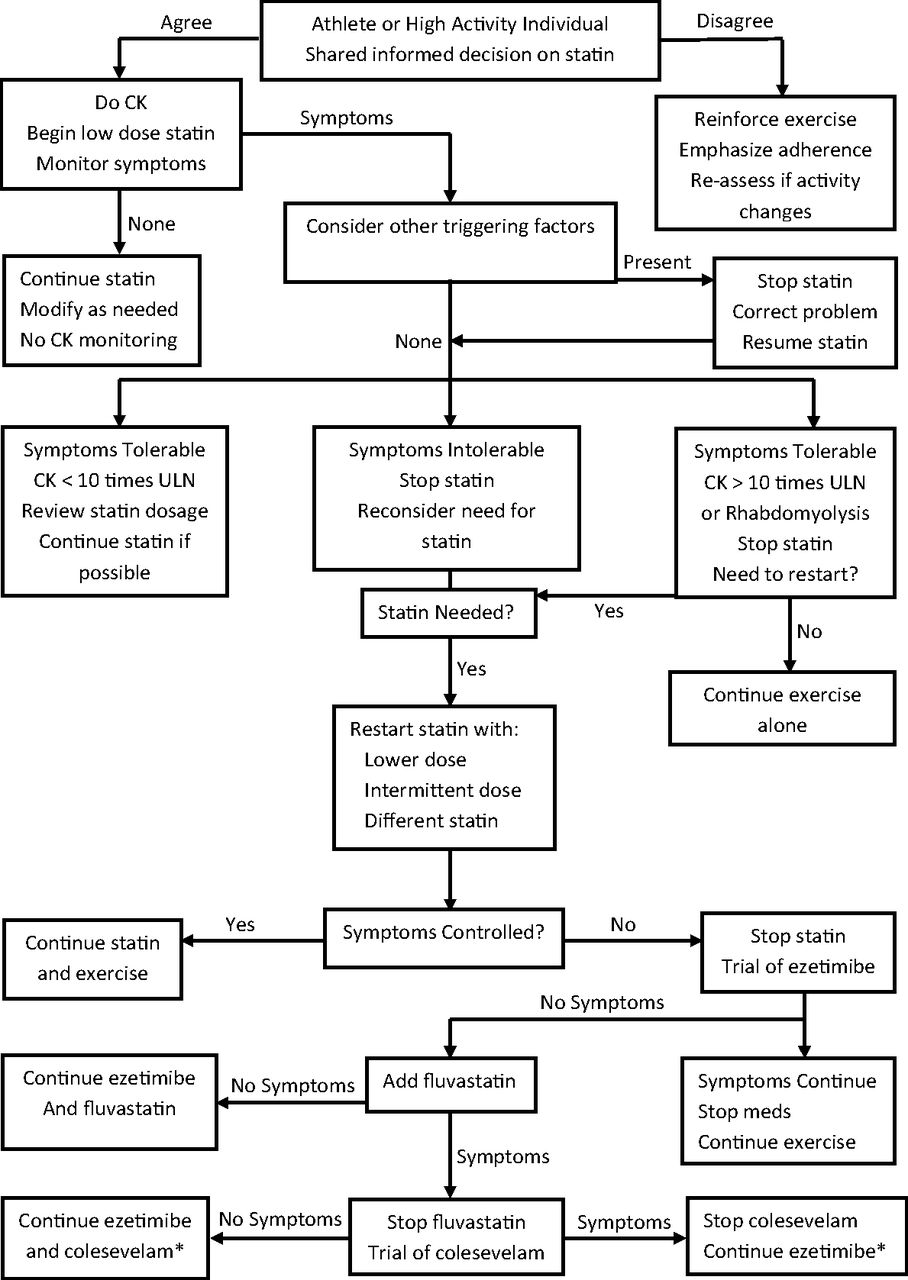
- Figure 1.
Management of statin myopathy in exercising adults. *Lowers low-density lipoprotein (no evidence of cardiovascular disease event reduction109). CK, creatine kinase; ULN, upper limit of normal.
Tables
Strength of Recommendation Definition A Based on consistent and good-quality, patient-oriented evidence* B Based on inconsistent or limited-quality patient-oriented evidence* C Based on consensus, usual practice, opinion, or case series Study Quality Definition Examples Level 1 Good-quality, patient-oriented evidence* High-quality RCT SR or MA of high-quality studies High-quality prospective cohort study or SR or MA of such studies Level 2 Limited-quality, patient-oriented evidence* Lower-quality clinical trial Lower-quality cohort study Retrospective cohort study SR or MA of lower-quality studies or studies with inconsistent findings SR or MA of lower-quality cohort studies or studies with inconsistent results Case-control study Level 3 Other evidence Consensus guidelines Expert opinion Case series Adapted from Ebell et al.22
↵* Patient-oriented evidence measures outcomes that matter to patients, such as morbidity, mortality, symptom improvement, and quality of life. Measures of disease activity or surrogate outcomes may or may not matter to the patient.
MA, meta-analysis; RCT, randomized controlled trial; SR, systematic review.
Myopathy Myalgia Myositis Rhabdomyolysis Canadian Working Group23 General term for muscle events Normal CK Aching or weakness CK more than the ULN Aching or weakness Aching or weakness CK >10× ULN ± Renal dysfunction NLA Muscle Safety Task Force24 Spectrum of muscle events Muscle soreness, stiffness, cramps, tenderness Muscle inflammation CK >3× ULN with myoglobinuria or acute renal failure ACC/AHA/NHLBI Clinical Advisory25 General term for muscle events Normal CK Aching or weakness CK more than the ULN Aching or weakness Aching or weakness Marked CK elevation + Elevated creatinine + Urine myoglobin ACC, American College of Cardiology; AHA, American Heart Association; CK, creatine kinase; NHLBI, National Heart Lung and Blood Institute; NLA, National Lipid Association; ULN, upper limit of normal.
Reference, Year Study Population Design, Intervention Findings SORT Study Quality Comments Panza et al,46 2015 418 adults not taking statins
Age 44 ± 16.1 years
50% menRCT; high-dose statin vs placebo for 6 months PA ↓ over time in placebo and statin arms equally Level 1* Young; very few at high activity levels
Used accelerometryParker et al,40 2013 420 healthy adults not taking statins
50% menRCT; high-dose statin vs placebo for 6 months PA ↓ over time in both placebo and statin arms; ↑ myalgia and CK in statin arm
Statin arm had significant myalgia ↑, PA ↓ in >55-year-old age group vs controlsLevel 1 Young; very few at high activity levels
Used accelerometryGolomb et al,47 2012 1016 adults
No CVD or diabetes
LDL 3.0 to 5.0 mmol/L
Age ≥20 years
67% menRCT; moderate-dose statin vs placebo for 6 months Scale-rated energy levels ↓ and fatigue with exertion ↑ with statins
Effects worse for womenLevel 1 4 in 10 women noted some harm
2 in 10 noted harm overallMikus et al,48 2013 37 sedentary overweight or obese adults with ≥2 MS risk factors not taking statins
Age 25–59 years
35% menRCT; moderate-dose statin + PA vs PA alone for 12 weeks Statin attenuated ↑ in cardiorespiratory fitness (↑ 1.5% with statin vs 10%) Level 2 No placebo control
Younger populationScott et al,49 2009 774 noninstitutionalized older adults
Age 62 ± 7 years
52% menProspective cohort study, 2.6 years Statin users had reduced leg strength over 2.6 years vs controls Level 2 Strength measured by dynamometry Qureshi et al,50 2015 17,264 adults
Age 59 ± 8 years
54% menProspective cohort study, 5.4 years Statins did not affect peak treadmill performance
Statin users were more sedentaryLevel 2 Mortality study comparing the benefits of fitness and statins Lee et al, 512014 5994 elderly men
Age ≥65
100% menProspective cohort study, 6.9 years Men taking statins had a 10% ↓ in PA and showed more sedentary behavior
New statin users had the most rapid decline in PALevel 2 PA measured by accelerometry
Moderate PA ↓ 9.6% and vigorous PA ↓ 9% among statin usersWilliams et al,45 2015 66,377 runners and 12,031 walkers not taking statins
Age 21–82 years
55% menProspective cohort study, 7.2 years PA levels ↓ in all hypercholesterolemic people, whether taking statins or not
? Reverse causality (↓ PA may have led to high lipids)Level 2 Majority age 40–50 years
Rate of statin discontinuation was not recorded
Low-dose statinsBruckert et al,18 2005 7924 unselected hyperlipidemic patients taking high-dose statins
Age 18–75 years
70% menObservational, cross-sectional study Muscle symptoms in 10.5%
38% of these were unable to tolerate moderate activityLevel 3 Self-report of activity
No placebo control
14% with high PA levels had muscle symptomsTerpak et al,52 2015 749 swimmers, 558 controls
Age ≥35 yearsCross-sectional study Statin use not associated with change in swimming activity Level 3 Self-report of activity Cham et al,53 2010 354 adults taking statins
Age 34–86 years
53% menCase series One-third met causality criteria for statin myalgia†
Activities most affected were running and walkingLevel 3 Subjects were self-selected
Self-reportSinzinger et al,43 2004 22 elite athletes with familial hypercholesterolemia
Age 13–35 years
68% menCase series 80% were unable to tolerate any statin dose Level 3 Series of professional athletes monitored in clinic for 8 years
Young populationCK, creatine kinase; CVD, cardiovascular disease; LDL, low-density lipoprotein; MS, metabolic syndrome; PA, physical activity; RCT, randomized controlled trial.
↵* SORT represents the Strength of Recommendation Taxonomy rating of study quality determined by Ebell et al.22
↵† Muscle symptoms improved upon reducing or discontinuing the statin dose and resumed upon restarting the drug.
Meta-analyses Duration (Years) Coronary Events (HR) Total CVD Events (HR) CV Mortality (HR) All-Cause Mortality (HR) Thavendiranathan et al,84 2006 4.3 0.78 (NNT, 60) NS NS Mills et al,85 2008 1.8–5.2 0.85 0.89 0.93 Petretta et al,86 2010 3.9 Men: 0.59
Women: NSMen: NS
Women: NSBruckert et al,18 2005 4.1 0.70 (NNT, 77) 0.88 (NNT, 167) Ray et al,87 2010 3.7 NS Mora et al,88 2010 Not stated Women: 0.63 Women: NS Kostis et al,89 2012 4.0 Men: 0.73
Women: 0.85Men: NS
Women: 0.87Savarese et al,6 2013 3.5 0.61 NS NS Taylor et al,90 2013 1–5.3 0.73 0.65 (NNT, 56) 0.86 (NNT, 96) CV, cardiovascular; CVD, cardiovascular disease; HR, hazard ratio; NNT, number needed to treat; NS, not significant.
- Table 5.
Exercise Benefit in Primary Prevention: Meta-analyses of Prospective Cohort Studies
Authors Time Interval (Years) Moderate Exercise (HR) Vigorous Exercise (HR) Pooled Exercise (HR) (Data Source) Mortality studies Hamer and Chida,20 2008 4–31 0.68 Löllgen et al,94 2009 5–26 Men: 0.81
Women: 0.76Men: 0.78
Women: 0.69Nocon et al,95 2008 4–20 Overall: 0.67 (fitness test: 0.59; self-report: 0.71) Cardiovascular event studies Sofi et al,19 2008 4–25 0.88 0.73 Li and Siegrist,96 2012 >5 0.89 0.76 Sattelmair et al,97 2011 No record 0.86 0.80 Hamer and Chida,20 2008 4–31 0.69 Nocon et al,95 2008 4–20 Overall: 0.65 (fitness test: 0.43; self-report: 0.70) HR, hazard ratio.
Conclusion SORT Categorization References Myopathy is a significant adverse outcome of exposure to statins. A 40 Addition of statins in exercising adults significantly increases myopathy risk. B 18 Addition of statins may present special risk for reduction in physical activity in: Very high levels of activity C 43 The elderly B 40, 44, 49 High-dose statin therapy B 18 Statins added to exercise can provide additional protection against cardiovascular events and mortality. B 21 A stable level of physical activity should be established before starting a statin. B 58, 59 If statins are used, low doses can provide similar protection to high doses in primary prevention. B 60, 61 Fluvastatin may be the least myotoxic of the statins and the least likely to cause myalgia with exercise. B 18, 35 Ezetimibe and colesevelam do not cause myopathy and may be useful in combination or when added to a statin. B 82, 86 Other measures to improve statin tolerance may be useful, but evidence is of low quality and confounded by a considerable nocebo effect. C 53, 62, 63, 69, 70 If a choice needs to be made between drug and exercise interventions, continued exercise is the better option. B 21 SORT, Strength of Recommendation Taxonomy.22
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Obstacles aux interventions cliniques liees a lactivite physique dans le traitement des maladies cardiometaboliques
- Impediments to clinical application of exercise interventions in the treatment of cardiometabolic disease
- Bread and Butter of Family Medicine: Guidelines, Population Screening, Diagnostic Evaluations, and Practice Models