
Article Figures & Data
Figures
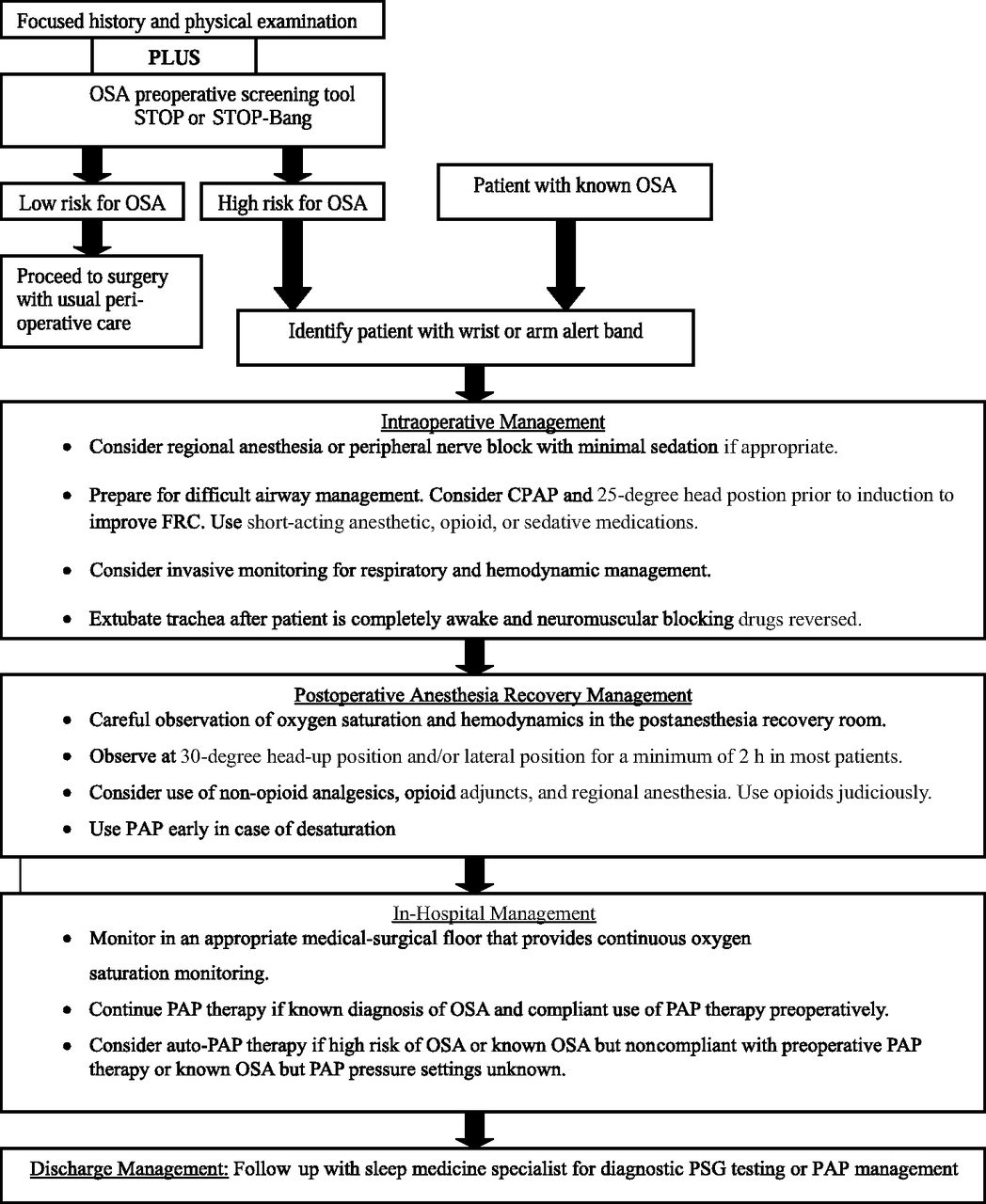
- Figure 1.
Perioperative management of adult patients with obstructive sleep apnea (OSA) or at high risk for OSA undergoing elective, non–upper airway surgery. CPAP, continuous positive airway pressure; FRC, functional residual capacity; PAP, positive airway pressure; PSG, polysomnography. Adapted from Adesanya et al.5
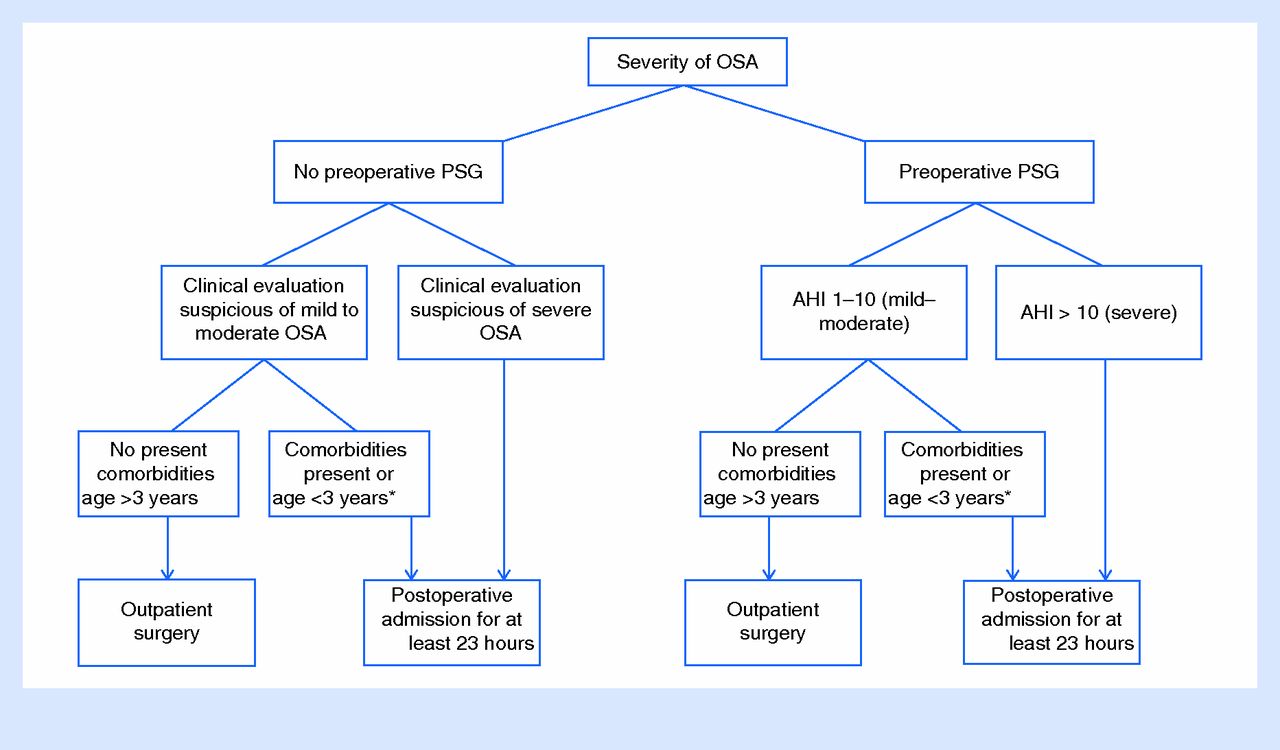
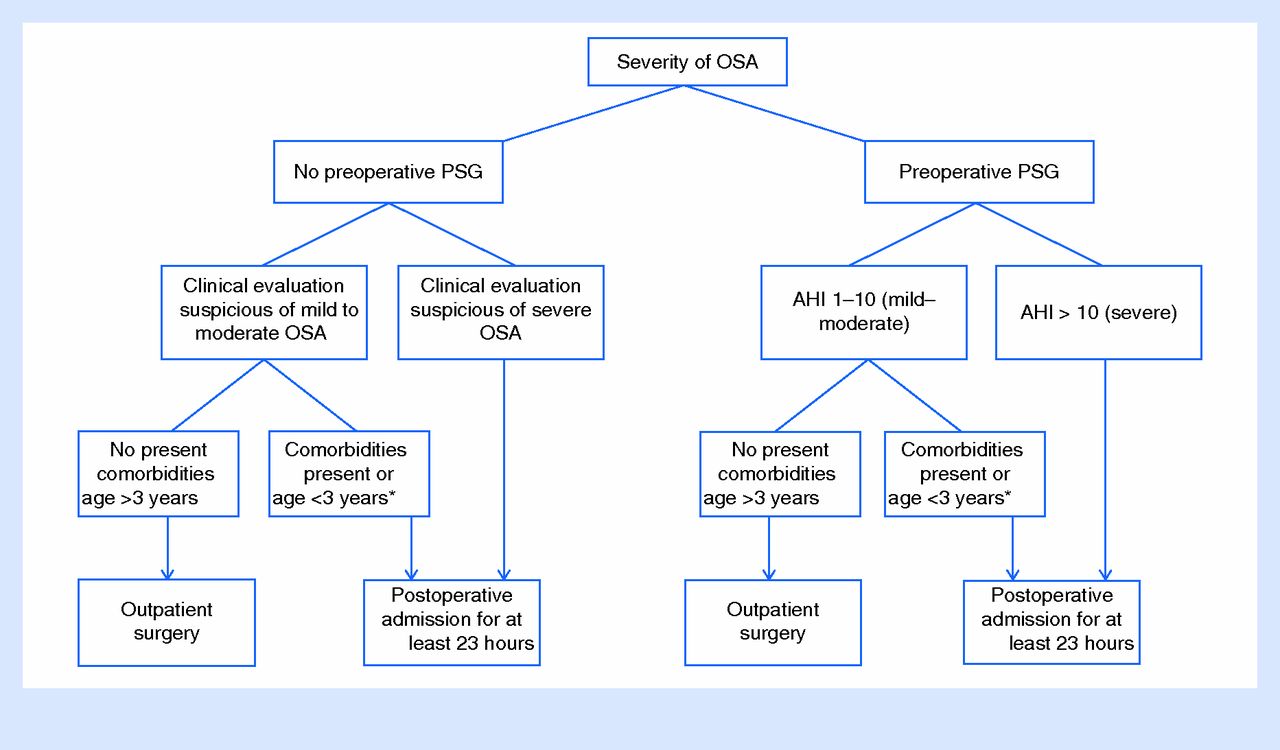
- Figure 2.
Post-adenotonsillectomy disposition of children with obstructive sleep apnea (OSA). *Comorbidities in children <3 years old include severe OSA documented by polysomnography (PSG), failure to thrive, obesity, cardiac involvement (right ventricular hypertrophy), Down syndrome, history of prematurity, craniofacial abnormalities, neuromuscular diseases, chronic lung disease, and sickle cell disease (comorbidities are taken from Table 3 in Ref. 65). AHI, Apnea-Hypopnea Index. From Patino et al.65

Tables
Apnea Adult: ≥90% drop in airflow from baseline lasting ≥10 seconds*
Children: ≥90% reduction of airflow from the pre-event baseline for ≥2 breaths with respiratory effort throughout this periodHypopnea Adult: abnormal respiratory event lasting at least 10 seconds with ≥30% reduction in thoracoabdominal movement or airflow compared with baseline, and with at least a 4% oxygen desaturation18
Children: ≥30% reduction of nasal airflow from the pre-event baseline for at least 2 breaths, and with at least a 3% oxygen desaturationAHI Number of apneas plus hypopneas per hour of sleep
Based on the AHI, the severity of OSA is classified as follows7,19:OSA severity Adult criteria (AHI/hour)† Pediatric criteria (AHI/hour) None/minimal <5 0 Mild 5–14 1–5 Moderate 15–29 6–10 Severe ≥30 >10 Oxygen Desaturation Index Hourly average number of desaturation episodes, defined as ≥4% decrease in saturation from the average saturation in the preceding 120 seconds, and lasting >10 seconds Central apnea Reduction in flow is mainly caused by a reduction in ventilatory effort Obstructive apnea Reduction in airflow is mainly caused by increased upper airway resistance OSA syndrome Adults: AHI score ≥15 events/hour or ≥5 events/hour with symptoms (such as daytime somnolence, fatigue, and cognitive impairment; or cardiovascular comorbid conditions, such as hypertension, ischemic heart disease, or prior stroke)‡
Children: disorder of breathing during sleep characterized by prolonged partial upper airway obstruction and/or intermittent complete obstruction (obstructive apnea) that disrupts normal ventilation during sleep and normal sleep patterns, accompanied by symptoms or signs§↵* The American Academy of Sleep Medicine (AASM) definition; Centers for Medicare & Medicaid Services (CMS) uses cessation of airflow.
↵† Most studies use these criteria. Because of a lack of a uniform definition of obstructive sleep apnea (OSA) severity, the American Society of Anesthesiologists' latest guideline on perioperative management of OSA uses the terms mild, moderate, and severe “as defined by the laboratory where the sleep study was performed.” If overall severity is not indicated by the sleep laboratory, they classify OSA severity from Apnea-Hypopnea Index (AHI) as none (0–5), mild (6–20), moderate (21–40), severe (>40).7
↵‡ Criteria for OSA diagnosis of both AASM and the CMS.19
Also see Berry et al.20
↵§ As listed in Table 2, right column, “Symptoms and Signs of Pediatric OSAS.”16
Clinical Features of Adult OSAS Symptoms and Signs of Pediatric OSAS Breathing disturbances during sleep Nocturnal Symptoms Habitual, socially disruptive snoring Snoring Witnessed apneas Gasping Gasping or choking Noisy breathing (typically inspiratory) Difficulties maintaining sleep Paradoxical breathing Snort arousals Retractions (cervical or costal) Dyspnea spells Witnessed apneas Restlessness Restless sleep Nocturia Neck hyperextension Diaphoresis Mouth breathing Gastroesophageal reflux Nocturnal sweating Daytime dysfunction Enuresis (after 6 mo continence) Nonrestorative sleep
Excessive daytime sleepiness in a nonstimulating environment (eg, watching TV, reading, riding in/driving a car)Parasomnia (walking, talking, terrors) Bruxism Mouth breathing
Daytime SymptomsMotor vehicle accidents, especially a history of “falling asleep at the wheel” Difficulty waking Unrefreshed on waking Impaired concentration, cognition, or memory Excessive sleepiness Headaches upon arising Hyperactivity Mood lability Aggression/moodiness Weakened libido Mouth breathing Risk factors Poor appetite Obesity Dysphagia Smoking Difficulty in school Nasal congestion Signs/Findings Alcohol Tonsil hypertrophy Sedative/hypnotics High/large tongue position Opioid analgesics Growth disturbance Supine (on the back) sleep positioning Obesity Comorbidities Failure to thrive Hypertension Pulmonary hypertension Myocardial infarction Systemic hypertension Congestive heart failure Craniofacial abnormalities Stroke Laryngomalacia Pulmonary hypertension Nasal airway obstruction Diabetes/metabolic syndrome HypotoniaGastroesophageal reflux Column 1 (adult) adapted from Ref. 23. Column 2 (pediatric) reprinted from Ref. 16.
OSAS, obstructive sleep apnea syndrome.
Variables Berlin Questionnaire ASA Checklist STOP Questionnaire STOP-Bang Questionnaire Nocturnal Oximetry Authors Chung et al.46 Chung et al.46 Chung et al.47 Chung et al.47 Chung et al.48 Validation Perioperative setting Perioperative setting Perioperative setting Perioperative setting Perioperative setting Items (n) 10 14 4 8 — High risk of OSA Score ≥2 categories Score ≥2 categories Positive score ≥2 Positive score ≥3 ODI >10 AHI ≥15 Sensitivity (%) 78.6 (67.1–87.5) 78.6 (67.1–87.5) 74.3 (62.4–84.0) 92.9 (84.1–97.6) 93.3 (89.7–97.0) Specificity (%) 50.5 (40.6–62.3) 37.4 (28.2–47.3) 53.3 (43.4–63.0) 43.0 (33.5–52.9) 74.6 (69.6–79.6) AHI ≥30 Sensitivity (%) 87.2 (72.6–95.7) 87.2 (72.6–95.7) 79.5 (63.5–90.7) 100 (91.0–100.0) 100 (100–100) Specificity (%) 46.4 (37.9–55.1) 36.2 (28.2–44.8) 48.6 (40.0–63.0) 37.0 (28.9–45.6) 58.6 (53.7–63.4) Data are presented as mean percentage (95% confidence interval)
Adapted from Ankichetty and Chung.49
AHI, Apnea-Hypopnea Index; ASA, American Society of Anesthesiologists; OSA, obstructive sleep apnea; ODI, Oxygen Desaturation Index (see Table 1 for a definition of ODI).

Practice Recommendation Level of Evidence References A question about snoring should be part of every pediatric preoperative assessment.* If the answer is affirmative or if a child or adolescent presents with signs or symptoms of OSAS, clinicians should perform a more focused evaluation. B 58 Preoperative screening using the STOP or STOP-Bang questionnaire should become routine to identify adult patients at increased risk of OSA. C 50, 70 Continuous postoperative monitoring with pulse oximetry is effective in detecting hypoxemic events in patients with known or suspected OSA. B 7 ↵* The original American Academy of Pediatrics guideline recommends asking about snoring “as part of routine health maintenance visits.”
OSA, obstructive sleep apnea; OSAS, obstructive sleep apnea syndrome.

In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Quality improvement initiative: use of the STOP-BANG score and monitoring to reduce adverse events in hospitalised patients at risk of obstructive sleep apnoea
- Rationalising requests for preoperative sleep studies and postoperative HDU beds: a quality improvement project in paediatric ENT patients undergoing elective surgery
- Pulmonary edema post-adenotonsillectomy in children
- Economic Assessment of 4 Approaches to the Diagnosis and Initial Treatment of Sleep Apnea
- Content Usage and the Most Frequently Read Articles of 2016
- Outcomes of Health System Structures, Highly Pertinent Clinical Information, Idea Stimulators, Clinical Reviews, and Prediction Tools: JABFM Exemplified