
Abstract
Objective: The objective of this study was to examine the impact of the transition from International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM), to Interactional Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM), on family medicine and to identify areas where additional training might be required.
Methods: Family medicine ICD-9-CM codes were obtained from an Illinois Medicaid data set (113,000 patient visits and $5.5 million in claims). Using the science of networks, we evaluated each ICD-9-CM code used by family medicine physicians to determine whether the transition was simple or convoluted. A simple transition is defined as 1 ICD-9-CM code mapping to 1 ICD-10-CM code, or 1 ICD-9-CM code mapping to multiple ICD-10-CM codes. A convoluted transition is where the transitions between coding systems is nonreciprocal and complex, with multiple codes for which definitions become intertwined. Three family medicine physicians evaluated the most frequently encountered complex mappings for clinical accuracy.
Results: Of the 1635 diagnosis codes used by family medicine physicians, 70% of the codes were categorized as simple, 27% of codes were convoluted, and 3% had no mapping. For the visits, 75%, 24%, and 1% corresponded with simple, convoluted, and no mapping, respectively. Payment for submitted claims was similarly aligned. Of the frequently encountered convoluted codes, 3 diagnosis codes were clinically incorrect, but they represent only <0.1% of the overall diagnosis codes.
Conclusions: The transition to ICD-10-CM is simple for 70% or more of diagnosis codes, visits, and reimbursement for a family medicine physician. However, some frequently used codes for disease management are convoluted and incorrect, and for which additional resources need to be invested to ensure a successful transition to ICD-10-CM.
The transition to the International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM), will have a huge impact on practicing physicians in the United States.1 The transition date of ICD-10-CM was October 1, 2015. The list of potential diagnosis codes in ICD-10-CM is 5 times larger than its International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) counterpart currently used in practice.2The American Medical Association estimates that the cost of the transition to ICD-10-CM is between $83,000 and $2 million per physician practice.1 A more recent Medical Management Group Association report revealed that the average cost to upgrade/replace practice management systems to use ICD-10-CM diagnosis codes per full-time-equivalent practitioner is $10,190.00.3 Additional costs to upgrade/replace electronic health records to use ICD-10-CM diagnosis codes will average $9,979.00 per full-time-equivalent practitioner.3 Previous studies have evaluated a number of different medical specialties with regard to the transition to ICD-10-CM.4⇓–6 The recent ruling by the Center for Medicaid and Medicare Services (CMS) to not deny any claim because of a lack of specificity for the first year during the transition to ICD-10-CM highlights the challenge and potential impact of the new coding system.7 To our knowledge, no other studies have evaluated the impact ICD-10-CM will have on the practice of family medicine.
The United States is the last country to transition to ICD-10-CM. The difficulties in making this national transition are multifactorial, but all can be overcome.8 Some concerns, as evidenced by a Swiss study, showed that it took up to 5 years before ICD-10-CM became as accurate as ICD-9-CM.9 In a Canadian study, the use of ICD-10-CA (the Canadian version of ICD-10-CM but with fewer codes) had a variable impact on quality compared with ICD-9-CM.10 The objective of this study was to examine the impact of ICD-10-CM on family medicine and identify areas where additional training and preparation might be required. The study was approved and given exempt status by our institutional review board (approval no. 2012-0773).
Methods
Overview
Family medicine ICD-9-CM codes were obtained from an Illinois Medicaid data set. Using the science of networks (mathematical algorithms to understand complex networks such as the Internet, interstate highway systems, and social networks), we evaluated each ICD-9-CM code used by family physicians to determine the relative difficulty of the transition for family medicine practices. Then the most frequently used codes with complex mappings were evaluated by a number of family medicine physicians for clinical accuracy in mapping them forward (see “Categorization of Complex Mapping”). A financial analysis was conducted to examine the impact of the different transitions.
Data Set
Data were culled from all Medicaid patients whose primary care provider was affiliated with the University of Illinois on April 2011; a complete set of all 2010 bills related to those patients composed the database.2 All physician bills were labeled by physician specialty. The data set was filtered for bills submitted by family medicine physicians. A total of 1635 ICD-9-CM diagnosis terms were submitted by family medicine physicians, for a total of $5.5 million in reimbursement and 113,000 patient visits. A subset of frequently encountered codes (codes used for >25 visits) was created. The visits with these 189 ICD-9-CM codes accounted for 106,726 visits (94% of all visits) and 80% of all costs ($4,414,005).
Mapping from ICD-9-CM to ICD-10-CM Codes
The CMS created a general equivalent mapping (GEM), a directional mapping from ICD-9-CM to ICD-10-CM.11 CMS also created a separate reverse mapping from ICD-10-CM to ICD-9-CM.11 A motif analysis tool was used to map all the ICD-9-CM diagnosis codes.2
Categorization of Complex Mapping
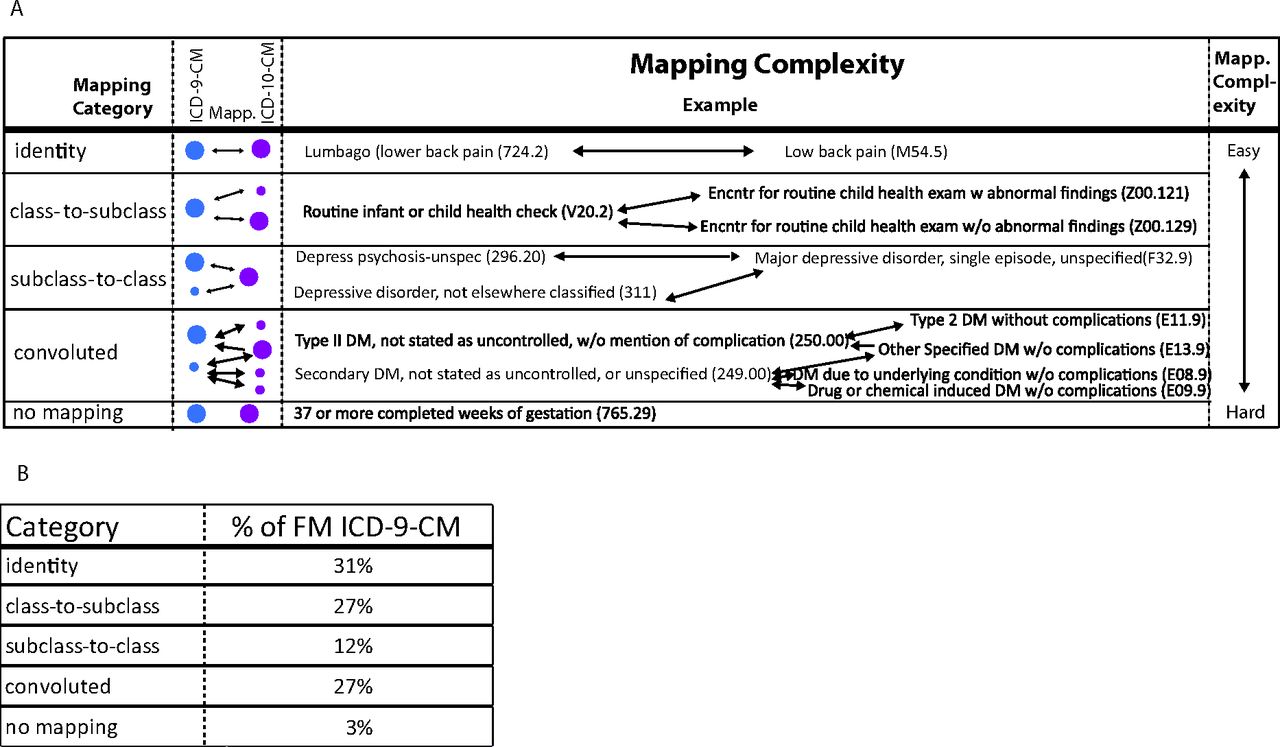
ICD-9-CM diagnosis codes have previously been categorized for the complexity of their transition to ICD-10-CM1 (Figure 1). The categories are simple and convoluted. Within the simple category are 3 subcategories: identity, where the ICD-9-CM and ICD-10-CM had a 1-to-1 mapping (Figure 1); class to subclass, where additional data are needed to classify the concept in ICD-10-CM; and subclass to class, where a number of concepts in ICD-9-CM are merged into a single ICD-10-CM concept. An example of the latter subcategory is when depressive disorder and depressive psychosis (unspecified) are mapped to major depressive disorder, single episode, unspecified (Figure 1).

Mapping complexity. Each International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) diagnosis code was categorized into 1 of 5 categories. A: The blue circles represent ICD-9-CM codes and the purple circles represent International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) diagnosis codes. The smaller circles represent secondary codes that are related to the category but have separate analysis as a primary code elsewhere. The arrows between the circles represent the mapping by the GEM files provided by the government. Identity is the category where 1 code replaces another code. Class-to-subclass is where multiple ICD-10-CM codes are represented by a single ICD-9-CM diagnosis code. Additional documentation or detail is required. Subclass-to-class is where multiple ICD-9-CM codes are represented by a single ICD-10-CM code. Convoluted codes are nonreciprocal and have secondary codes confounding the diagnosis concepts. No mapping is where the GEM file does not provide a mapping to the ICD-10-CM codes. B: Categories represent the percentage of diagnosis codes used in the complete data set in each category.
Simple codes comprise the above 3 categories. Convoluted codes represent transitions between coding systems that are nonreciprocal and have secondary codes confounding the diagnosis concepts. An example of a convoluted code is diabetes with or without complications (controlled or uncontrolled) mapping to various diagnostic codes with or without complications, and vice versa (Figure 1). Last, no mapping is an additional category used when the CMS methods do not provide any mapping forward to ICD-10-CM, for example, pregnancy codes (Figure 1).
Data Analysis
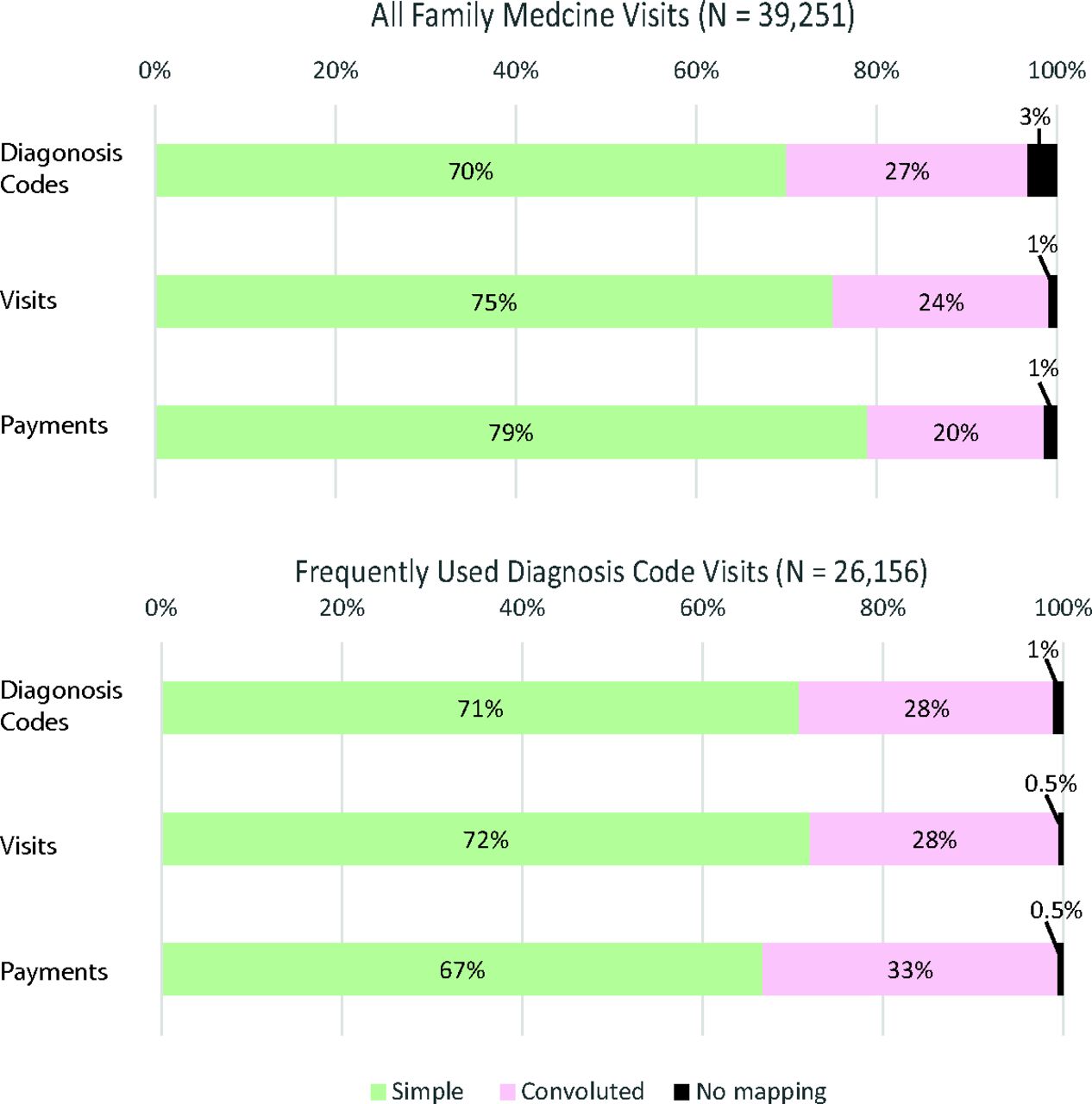
Using the science of networks, which leverages the relationships between ICD-9-CM and ICD-10-CM as provided by the GEM files,1 we mapped the family medicine ICD-9-CM diagnosis codes to the corresponding ICD-10-CM codes and labeled them as simple, convoluted, or no mapping.2 The benefit of the science of networks is that it mathematically reveals complex or convoluted transitions to ICD-10-CM. The initial analysis of each category involved the number of codes, the number of patient visits, and payment made for each unique code and for the more frequently (>25) encountered diagnosis codes (Figure 2).

Analysis of family medicine encounters. A: This graph analyzes all 39,251 encounters with family medicine physicians. The Diagnosis Codes graph counts each diagnosis code as a single value and categorizes all the codes as a percentage of the total number of codes. The Visits graph analyses all the visits for a specific diagnosis code and calculates a percentage of total number of visits. The simple diagnosis codes account for more visits than the convoluted codes. The Payments analysis takes the payments for each diagnosis code and categorizes them into the simple or convoluted diagnosis code category and divides by the total amount of reimbursement. B: A secondary analysis of all diagnosis codes used >25 times was performed and included a total of 26,156 visits. The percentages are nearly equivalent to the complete representation of visits.
For the frequently encountered diagnosis codes data set (n = 189 codes), the diagnosis codes that were labeled as convoluted (52 codes [28%[; Figure 2) were evaluated by 3 family physicians and classified as clinically correct or clinically incorrect. With the disagreements, when 2 of the 3 clinicians agreed it was incorrect, the code was listed. Additional financial analysis was performed on the clinically incorrect codes (Figure 2).
Results
Of the 1635 diagnosis codes used by family medicine physicians, 70% are categorized as simple, 27% are categorized as convoluted, and 3% have no mapping (Figure 2). Of all the 113,000 visits, percentages of patient visits for each diagnostic code category were 75%, 24%, and 1% for simple, convoluted, and no mapping, respectively (Figure 2). The frequently encountered codes (n = 189) had a similar distribution: 28% of the diagnosis codes and visits were convoluted and 33% of payments were convoluted (Figure 2).
Of the 189 most frequently used codes, the 53 most frequently encountered convoluted diagnosis codes were evaluated for accuracy of clinical mapping. A total of 16 codes were evaluated by 1 family medicine physician as being incorrect. However, only 3 were deemed clinically incorrect by at least 2 physicians (Table 1); this translates into roughly 5% of the frequently encountered convoluted codes as clinically incorrect (Table 2, full list of frequently encountered convoluted codes). However, only 0.2% of the overall codes are clinically incorrect when including the complete set of 1635 codes.
Discussion
When coding in ICD-10-CM, CMS recommends reviewing the patient documentation and then selecting ICD-10-CM codes. Use of automatic mapping software systems can lead to problems as through convolution. As highlighted in this article, 70% of the diagnosis codes are mapped forward relatively easily. While many family medicine physicians may not know about the GEM, using previously used ICD-9-CM codes as a frame of reference for what the terms are in ICD-10-CM is strongly recommended as a first step. The concept of convolution helps to highlight the 27% of family medicine codes for which the clinical concepts have changed. Documentation or paradigm shifts will likely be necessary to fully accommodate the new coding system in ICD-10-CM. One major challenge with convoluted codes will be disease management reports or other medical reports. By their nature, these reports typically provide comparison data from month to month or year to year, or they reflect seasonal comparison. Changing the clinical concepts between ICD-9-CM and ICD-10-CM could result in misleading reports. Detailed analysis about the change is necessary to identify which reports have to be modified when scrutinizing future data.
The example of a convoluted code (Figure 1), “type 2 DM, not stated as uncontrolled, without mention of complication” (ICD-9-CM code 250.00), is a great example. This code maps forward and reverse to “type 2 DM without complications” (ICD-10-CM code E11.9). The reason 250.00 is convoluted is because of the other associated code, “other specified DM without complications” (ICD-10-CM code E13.9). Code E13.9 only maps backward to 250.00, as well as to “secondary DM, not stated as uncontrolled, or unspecified” (ICD-9-CM code 249.00). When comparing the results before and after the transition to ICD-10-CM for diabetes registries, the mapping of E13.9 (ICD-10-CM) might inflate the number of type 2 DM data compared with historic data if the analyst or programmer selected 250.00 (ICD-9-CM) instead of 249.00 (ICD-9-CM). The concept of convoluted reveals this complex relationship, where additional analysis is required to ensure successful transition. Since many providers are now focusing special payments and incentives based on disease registries, convoluted codes that are tied to registries or disease management need even more attention to ensure minimal disruption.
While subclass-to-class transition is labeled as easy, some of the implications can have a wide effect on family physicians. For example, “Depression disorder NEC” (ICD-9-CM code 311; Figure 1), is mapped together with “Depressive disorder psychosis unspecified” (ICD-9-CM code 296.20). However, in the data set, “Depression disorder NEC” (ICD-9-CM code 311) is used 239 times where “Depressive disorder psychosis unspecified” (ICD-9-CM code 296.20) is used 17 times. If the family medicine physicians use educational tools to map the ICD-9-CM codes to ICD-10-CM, a question that remains to be answered is whether all family medicine physicians will label the 256 visits with the ICD-10-CM diagnosis of “Major depressive disorder, single episode, unspecified” (code F32.9). Or, if a physician is searching in ICD-10-CM for the diagnosis via a keyword search for depression or mood, will they select code F32.9 or choose a different diagnosis, such as “unspecified mood disorder” (ICD-10-CM code F39)? The challenge with the change in codes and selecting an even more generic description of the patient's condition is the ability for the health system to provide comprehensive services to the patient.
Another possible concern with the transition to ICD-10-CM is the potential increase in time required to code. Experience in Australia and Canada, which use less complex versions of ICD-10, have demonstrated an increased time to code in ICD-10, even after a year of experience.12,13 A recent study demonstrated that professional coders could need up to 75% more time to code in ICD-10-CM because of the increased size and complexity of coding.14 In another study, professional coders still took 50% more time to code in ICD-10-CM compared with ICD-9-CM after a year of experience.15 Professional coders currently charge approximately $3.25 per encounter (Gerald King, personal communication). If the increase in time is directly reflected in the cost for each coder, each encounter would increase by $1.62. If a family medicine doctor has 90 encounters a week and works 50 weeks in a year, the increase in cost totals $7,312 because of the increased time for the professional coders. Alternatively, the onus to code accurately could be placed on the physician, which would not directly increase the cost of care but could decrease time available to treat patients, which is a much more costly consideration.
The clinically incorrect mappings are relatively few (0.2% of the codes). As an example, the diagnosis code “type 2 diabetes mellitus of unspecified type uncontrolled without mention of complication” (ICD-9-CM code 250.02) with an incorrect mapping to ICD-10-CM will likely have a significant impact on diabetes registries for disease management in family medicine, complicating the concept even further compared with the challenges with ICD-9-CM code 250.00 described above.
There are some limitations to this study. The Medicaid data set was collected from only a single state. The claims for the state of Illinois may not be representative of the nation. In addition, the mapping to evaluate the impact of the transition to ICD-10-CM was provided by CMS. A number of commercial providers have also published transition mapping between ICD-9-CM and ICD-10-CM, which are protected by copyright and legal agreements. The evaluation of the transitions are the opinions of 3 family medicine physicians, and the complexity of medicine is reflected in their disagreements and how no transition to ICD-10-CM was considered incorrect by all 3 clinicians.
Complex mapping rates in family medicine are similar to those of pediatrics, whose convolution rate was 1 in 4.6 By contrast, family medicine mapping is slightly more complex than the 18% convolution rate of oncology.4
Every family medicine physician and practice have different patient disease burdens. The use of specific diagnosis codes is affected by local and regional variations. The good news is that, for the first year, CMS will not deny claims because of a lack of specificity.7 To help prepare for both the transition and eventual denial of claims for lack of specificity, we recommend that physicians evaluate their commonly used ICD-9-CM diagnosis codes and use one of the many free tools to see what ICD-10-CM codes are affiliated. The Health care Financial Management Association16 as well as the American Medical Association1 have provided a number of tools and educational materials to help family medicine physicians' transition to ICD-10-CM. Another tool provided by CMS is a clinical concept list for family medicine, which provides an initial overview of ICD-10 for family medicine physicians.17
In family medicine, 0.2% of the codes are clinically incorrect, but they are related to only <1% of the overall visits and <1% of the overall cost of care delivered. With ICD-10-CM offering up to 80,000 unique diagnosis codes, the small percentage of error within this subgroup of diagnosis codes seems quite benign.
Notes
This article was externally peer reviewed.
Funding: ADB and YAL are supported in part by the Center for Clinical and Translational Sciences of the University of Illinois (NIH 1UL1RR029879–01, NIH/NCATS UL1TR000050), the Institute for Translational Health Informatics of the University of Illinois at Chicago, and the Office of the Vice-President for Health Affairs of the University of Illinois Hospital and Health Science System.
Conflict of interest: ADB has been a speaker for Epic Corporation. Epic had no input into this paper or research.
- Received for publication May 1, 2015.
- Revision received August 6, 2015.
- Accepted for publication August 25, 2015.




{kind=link}
{kind=link}