
Article Figures & Data
Figures
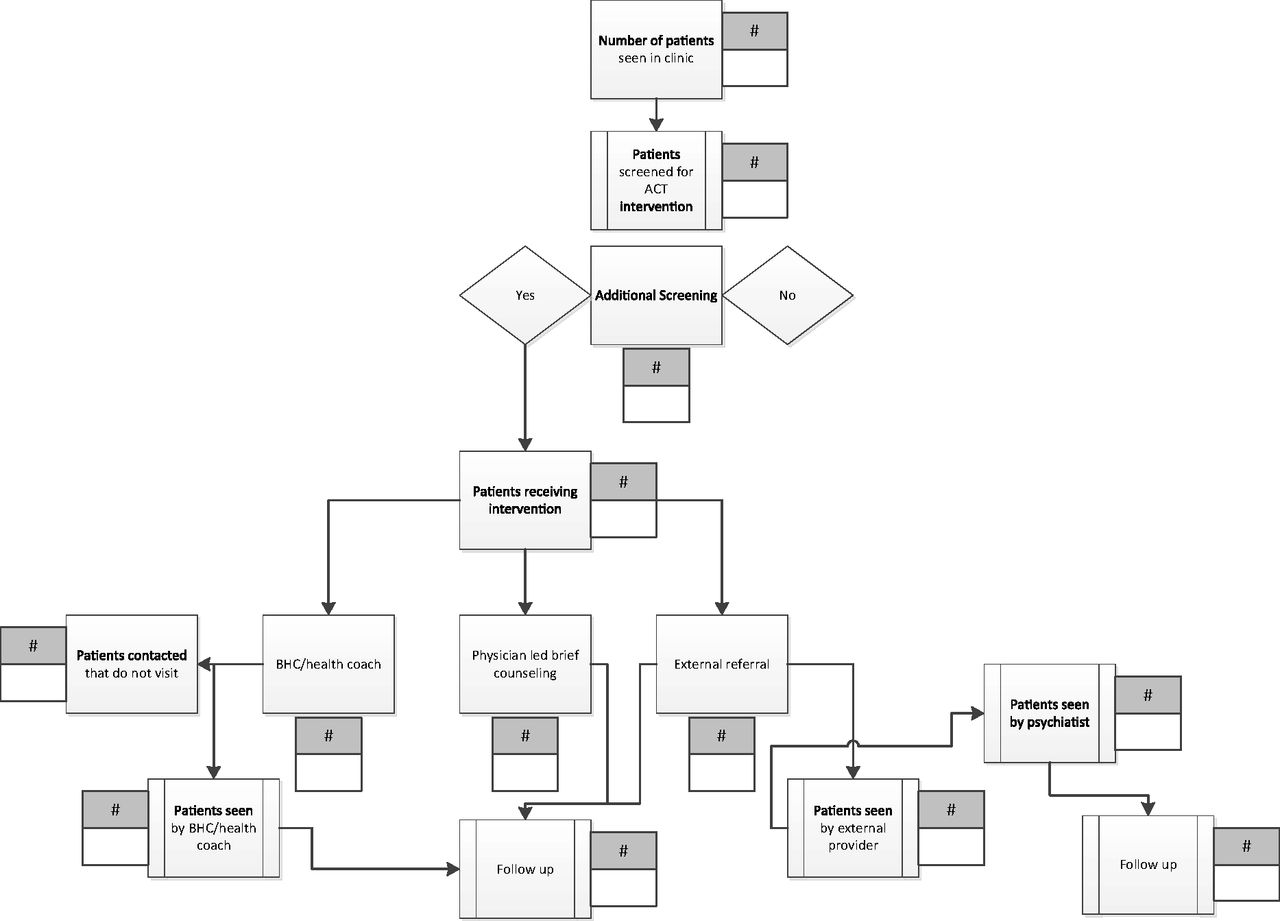
- Appendix Figure 1.
Example of an intervention process diagram. Adapted from an open access article published by Balasubramanian et al. in Implementation Science http://www.implementationscience.com/content/10/1/31. ACT, Advancing Care Together; BHC, behavioral health clinician.
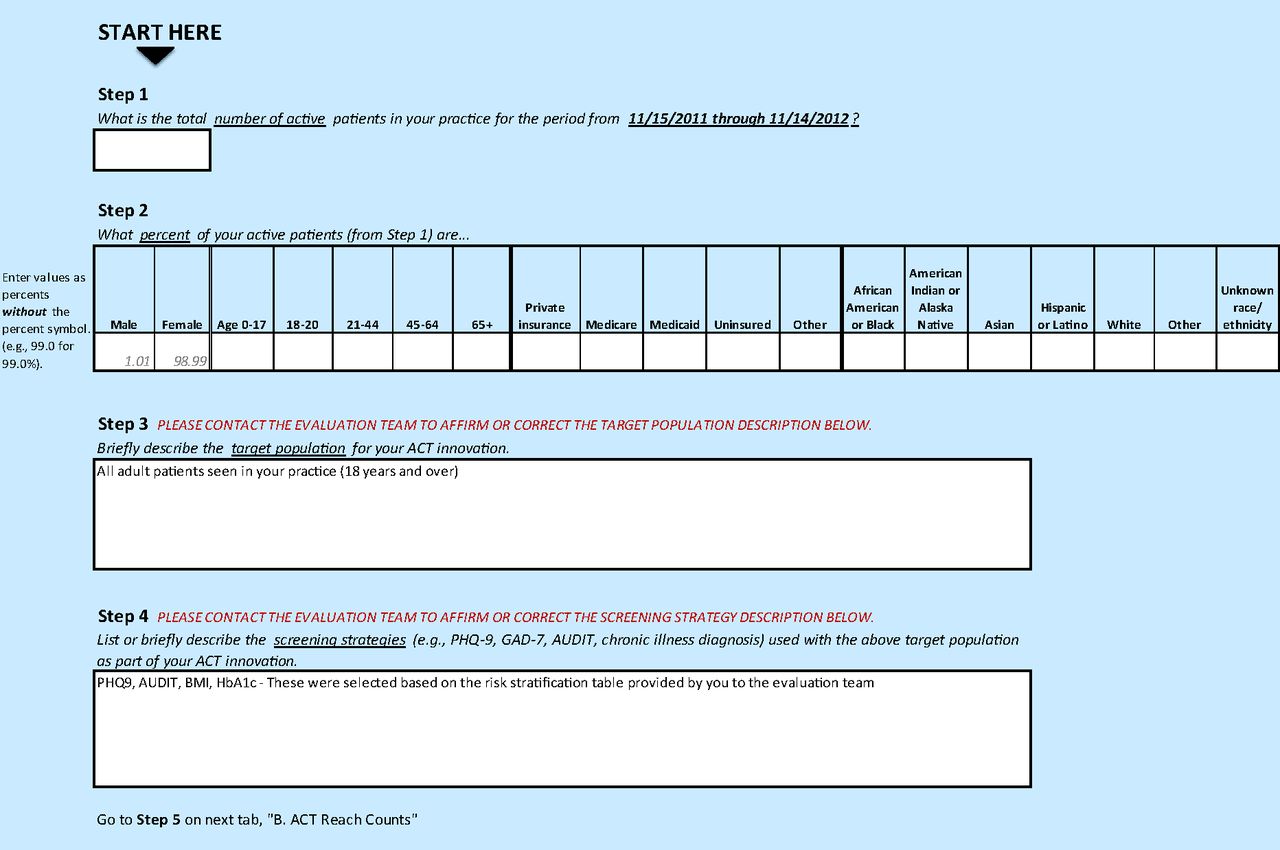
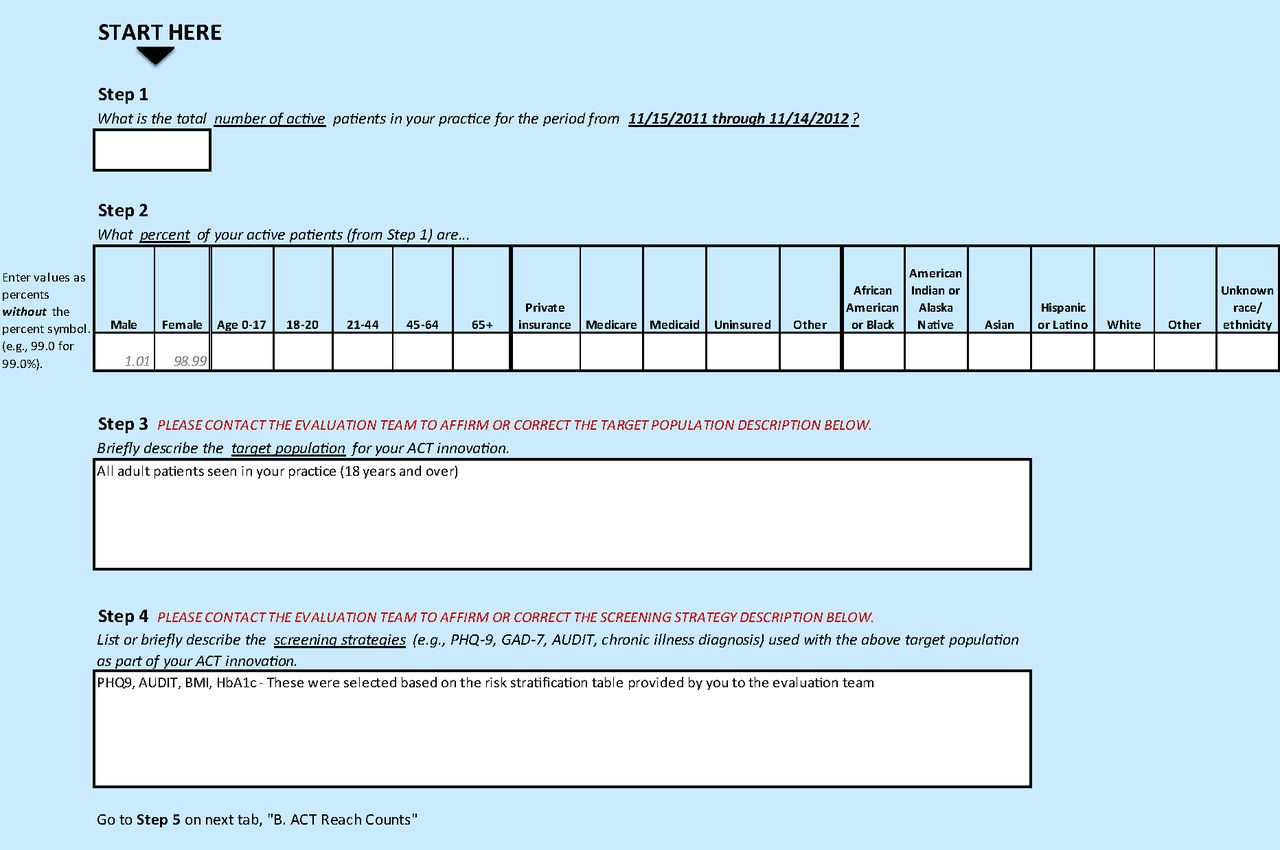
- Appendix Figure 2.
Advancing Care Together (ACT) REACH reporter.
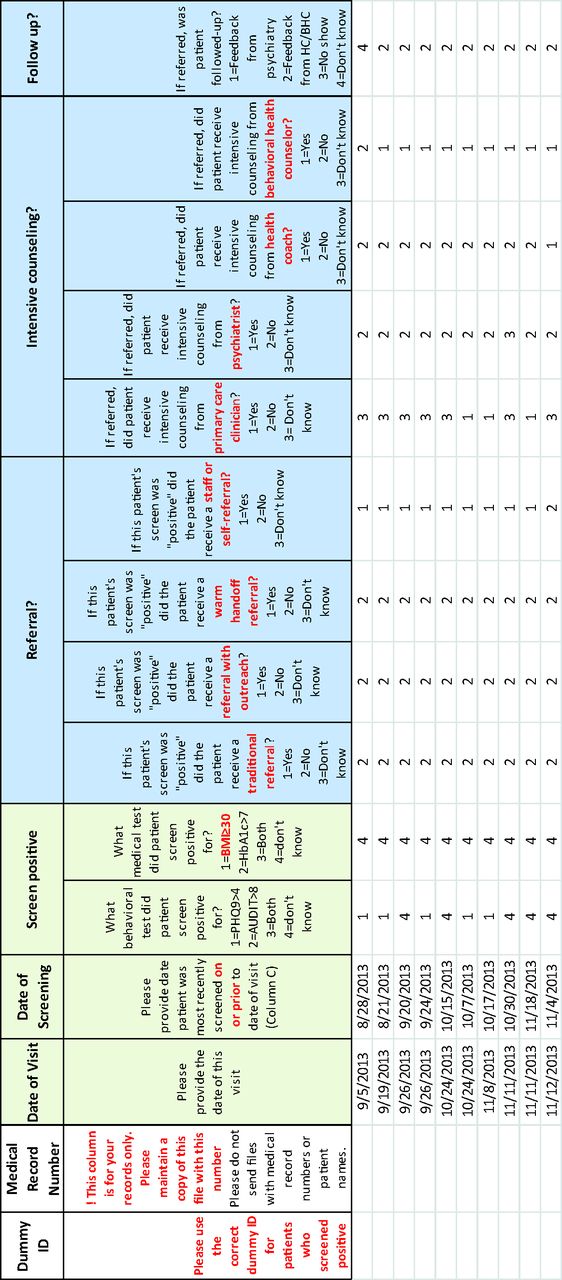
- Appendix Figure 3.
Example of a patient tracking sheet.


Tables
Site ID Type Ownership Provider FTEs Patient Sex, % Patient Ethnicity/Race, % Insurance Type, % Primary care Behavioral health Women Latino Black White Medicare Medicaid Uninsured Private 14 Multi-specialty group Hospital system, HMO, and not for profit 18.7 0.6 58 7 12 55 32 0.4 0 67 13 Multi-specialty group Clinician 13.6 1.0 59 7 0.6 85 15 8 6 69 4 Community health center Private not for profit 11 2 61 61 1 34 5 36 37 15 16 Single specialty group Hospital system 9 1.4 62 22 37 20 9 67 19 3 12 Multi-specialty group Hospital system 3.15 0.9 67 21 10 58 57 10 15 3 7 Multi-specialty group Clinician 10 0.5 43 6 0.04 94 11 20 7 62 10 Single specialty group Clinician 4.8 0.5 56 11 7 56 10 0 5 85 9 Solo Clinician 2 0.5 55 40 0 60 6 5 69 20 17 Single specialty group Federally qualified health center 6 2 53 34 0.9 63 12 20 36 29 18a Single specialty group Not for profit 0.4 22.8 64 17 2 76 12 36 43 6 19a Solo Not for profit 2.2 7.9 61 11 0.2 82 23 37 19 13 ↵a Mental health clinics.
Site ID Integration Strategy Target Population Method of Assessment Assessment Measures Used 4 This practice embedded psychology doctoral trainees in prenatal clinic Pregnant patients seen at clinic In waiting room by BHCs Completion of PHQ9, GAD7, AUDIT, HbA1c 7 This primary care practice automated screening for behavioral health needs using a tablet. A psychologist with a private, colocated practice became an employee who provided traditional mental health services in the practice. Patients ≥18 y seen at clinic In waiting room using tablet devices Completion of PHQ2 followed by PHQ9, if PHQ2 positive 10 This private primary care practice partnered with a CMHC to hire a BHC. The practice also expanded health coaching services. Patients ≥18 y seen at clinic In waiting room using paper-based survey, then transition to tablet devices Completion of PHQ9, GAD7, AUDIT 9 A small primary care practice added a traditional mental health therapist from a private mental health agency to provide colocated care and brief interventions. Patients ≥18 y seen at clinic In waiting room using paper-based survey, then transition to tablet devices Completion of PHQ9, GAD7, AUDIT, and to assess tobacco use. 17 An FQHC with a colocated mental health therapist added a colocated substance use counselor from a collaborating CMHC. Patients ≥18 y seen at clinic In waiting or exam room by medical assistants Completion of PHQ9 and SBIRT 19 This practice screened patients using a tablet device that was programmed to directly transfer entered data to an EHR-linked interface accessible to providers. Further, a PC clinician/MA team, and a BHC were embedded in the practice to provide primary care and BH services. Patients ≥18 y seen at clinic In waiting room using handheld tablet devices Completion of PHQ9, GAD7, AUDIT, BMI, HbA1c 16 This primary care practice expanded their existing integrated care model by working with a research team to develop and implement a screening form for patients to self identify behavioral health needs. English and Spanish-speaking patients ≥18 y seen at clinic In waiting room using paper-based survey Completion of a newly developed “Improve your Health” survey 12 A postdoctoral training program provides colocated mental health services in an FQHC serving seniors. A computerized cognitive and psychological screening program was developed and implemented. Patients ≥50 y seen for an annual wellness or medically necessary visit Clinical discretion by primary care providers Completion of a newly developed cognitive screening tool called CaPS 13 This private primary care practice expanded their partnership with a private mental health agency to provide integrated care. First, an urgent consult schedule was created for BHC services. Over time, services expanded to enable full-time BHC coverage within the practice setting. Patients ≥18 y seen at clinic for an annual, diabetes, or hypertensive exama Clinical discretion by primary care providers, then transitioned to systematic in waiting room using paper-based survey Completion of PHQ2 14 A BHC was embedded in a primary care setting with multiple clinics (e.g., family medicine, pediatrics). BHC provides brief counseling and helps connect patients to specialty MH services within the large, integrated health system or to external resources. Patients ≥18 y seen at clinic Clinical discretion by primary care providers Referral to a behavioral health counselor 18 A primary care team (including PA, MA, care coordinator, and substance use counselor) were embedded in a CMHC. Clients without primary care physician on record Clinical discretion by mental health providers Referral to the primary care team Abbreviations: BH, behavioral health; BHC, behavioral health clinician; CaPS, Cognitive and Psychological Screen; CMHC, community mental health center; FQHC, federally qualified health center; PC, primary care; AUDIT, Alcohol Use Disorders Identification Test; PHQ, patient health questionnaire; GAD, generalized anxiety disorder; HbA1c, glycosylated hemoglobin; BMI, body mass index; SBIRT, screening, brief intervention, and referral to treatment; PA, physician assistant; MA, medical assistant.
PHQ2 was used to screen for depression; PHQ9 was used to screen or monitor for depression; GAD7 was used to screen or monitor for anxiety disorder; AUDIT was used to screen or monitor for alcohol use; DAST was used to screen or monitor for substance use; BMI was used to screen or monitor for obesity; and HbA1c was measured to monitor for diabetes.
↵a Target population changed midstream.
Site ID Measure of Reach No. Target Patients No. Patients Assessed Screening REACHa (%) 4 Completion of PHQ9, GAD7, and AUDIT 65 51 78.5 7 Completion of PHQ9, GAD7, AUDIT, and to assess tobacco use 1876 287 15.3 10 Completion of PHQ9, GAD7, AUDIT, and HbA1c 1868 1609 86.0 9 Completion of PHQ2 followed by PHQ9 if PHQ2 is positive 546 498 91.0 17 Completion of PHQ9 and SBIRT 2519 1491 59.2 19 Completion of PHQ9, GAD7, AUDIT, BMI, and HbA1c 440 396 90.0 16 Completion of a newly developed “Improve your Health” survey 887 182 20.5 12 Completion of a newly developed cognitive screening tool called CaPS 942 34 3.6 13 Referral to behavioral health provider 1700 206 12.1 14 Referral to a behavioral health counselor 14,879 169 1.1 18 Referral to the primary care team 773 17 2.2 Total 24,906 6529 26.2 CaPS, Cognitive and Psychological Screen; AUDIT, Alcohol Use Disorders Identification Test; PHQ, patient health questionnaire; GAD, generalized anxiety disorder; BMI, body mass index; SBIRT, screening, brief intervention, and referral to treatment.
↵a Screening REACH is defined as percentage of target patients who were assessed for integrated care.
- Table 4. Receipt of Integrated Services for Patients Assessed Over a 3-Month Period Among ACT practices
Site ID Method of Identifying Patients Method to Track Patients No. Patients Screened Positive or Meeting Specific Criteria No. Patients Received Services Integrated Care Services REACHa (%) 4 Systematic Manual 23 21 91.3 7 Systematic EHR 69 62 89.9 10 Systematic Created new EHR template 689 176 25.5 9 Systematic Manual 261 Data not available — 17 Systematic Manual 289 44 15.2 19 Systematic Created new EHR template 267 126 47.2 16 Clinical discretion Manual 180 148 82.2 12 Clinical discretion Manual 33 32 97.0 13 Clinical discretion Manual 41 41 100.0 14 Clinical discretion EHR 169 169 100.0 18 Clinical discretion Manual 17 17 100.0 Total 2038 836 41.0 ACT, Advancing Care Together; EHR, electronic health record.
↵a Integrated care services REACH defined as percentage patients who received integrated services out of those screened positive or meeting specific criteria.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Outcomes of Integrated Behavioral Health with Primary Care
- From Our Practices to Yours: Key Messages for the Journey to Integrated Behavioral Health
- Strategies to Support the Integration of Behavioral Health and Primary Care: What Have We Learned Thus Far?
- Advancing Care Together by Integrating Primary Care and Behavioral Health
- Integrated Care: Tools, Maps, and Leadership
- Understanding Care Integration from the Ground Up: Five Organizing Constructs that Shape Integrated Practices