
Article Figures & Data
Figures
- Figure 1.
Printed version of the reminder form.
- Figure 2.
Number of encounters with varying numbers of reminders.
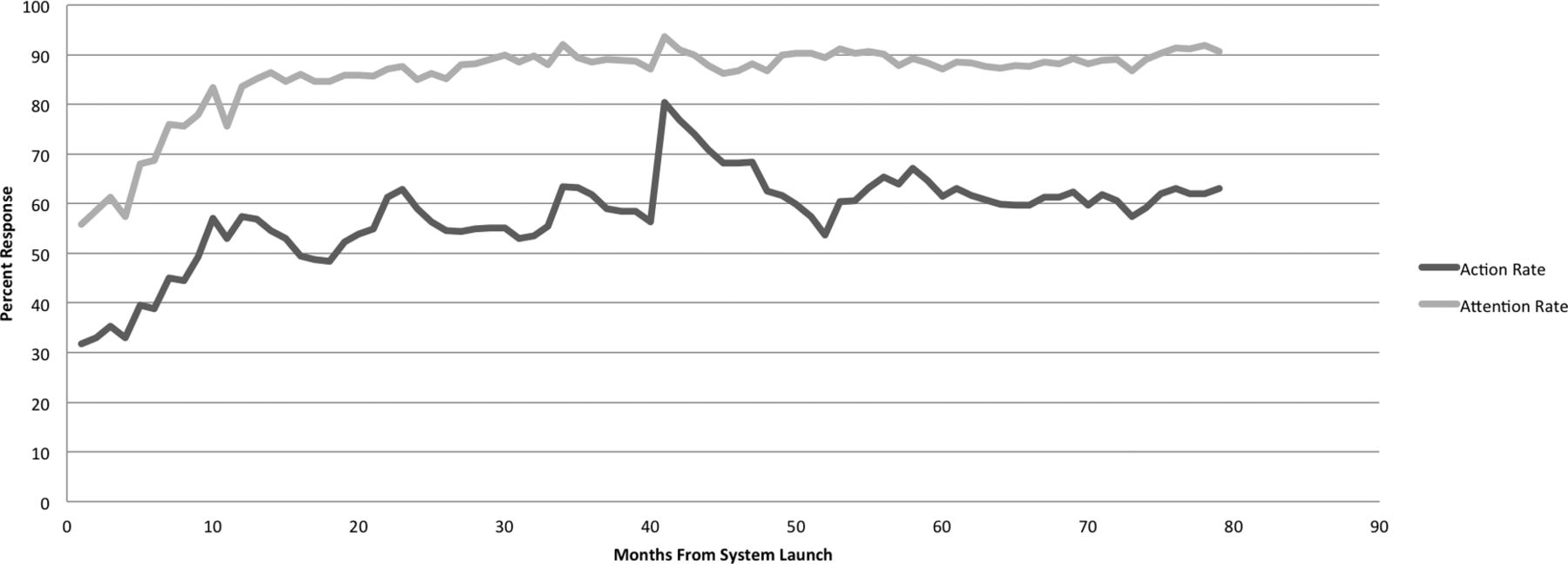
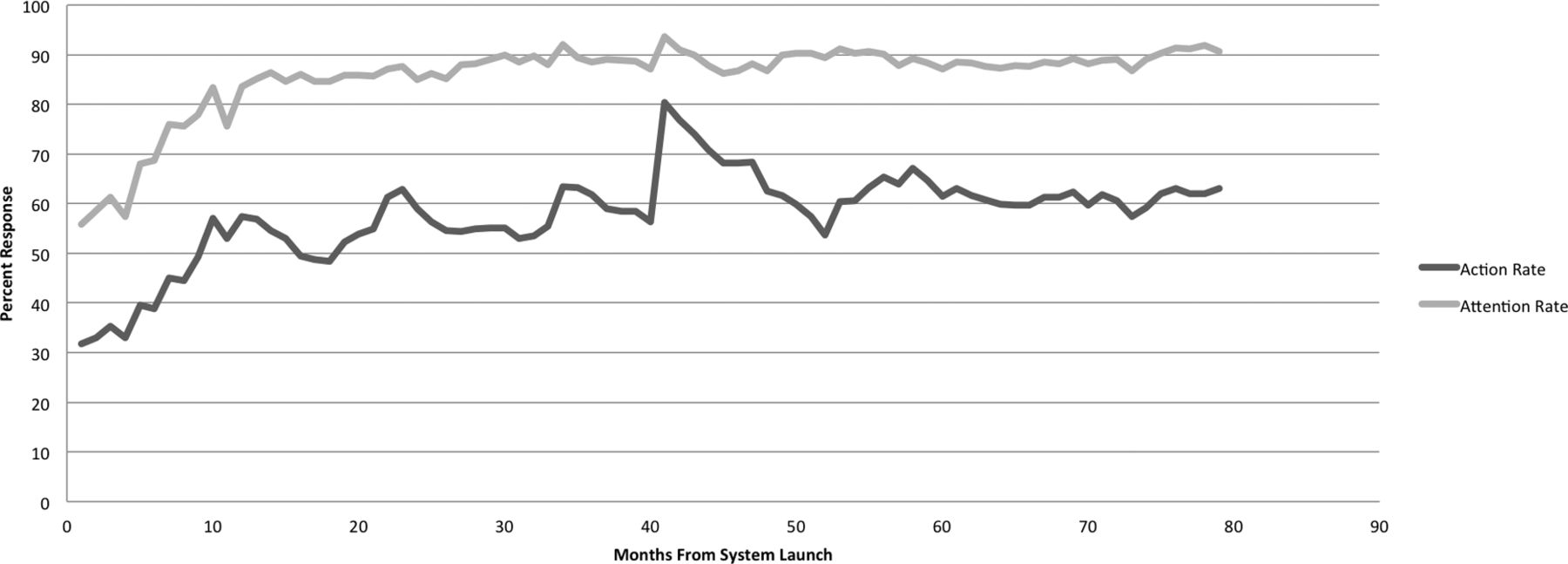
- Figure 3.
Reminder response rates by time.


Tables
Design principles Reminders must be simple action items, one line only. Absolutely no background, reference, or persuasive material should ever be included. Educating clinicians about and convincing them of the value of the services to be reminded about must take place off line, not in the time-pressured, information-saturated clinic environment.
Multiple response options must be offered. Clinicians should not have to spend time or effort determining how to handle the reminder itself, but focus only on its targeted service. Clinicians must be able to document patient refusal and designate individual patients as not candidates when appropriate.
“False alarms” must be aggressively minimized. They damage the system's credibility, and sorting valid from invalid reminders further adds to cognitive burden. Therefore billing diagnoses should not be used to drive reminders; rather, a clinician-verified problem list should be kept for each patient. Data from as many systems as possible should be imported to capture services provided and avoid triggering reminders for services already provided. Patient preference (refusal) and noncandidate status must suppress reminders (eg, do not issue irrelevant reminders for cervical cytology screening for patients who have had hysterectomies for benign disease).
The system must fit flexibly into the workflows of diverse physicians and teams. Different clinicians place their “windows of opportunity” for attending to additional information stimuli in different places within the visit structure and must accommodate the variable whereabouts of other team members. Some information may be handled outside of the visit, as well. Disrupting task structuring, such as with a “forcing function”20,21 approach requiring a response at a specific time and preventing other work until a response is made, should be avoided.
Implementation principles Support for the system as a whole, and for each new set of reminders to be added, must be gained before reminders are activated.
Reminders must address quality goals determined by clinicians in a group process. Reminders do not address cost-cutting measures or administratively imposed objectives.
Physicians and teams must be able to adapt the system to their own uses, which may not be foreseen by the design team.
Resources to make responding to reminders feasible in busy clinics must be in place before reminders are activated (eg, clinical support staff should be trained and have time allocated to educate patients with asthma and work out asthma action plans with them before initiating reminding for asthma action plans). Implementation may need to involve team members who are not directly part of visit workflows.
Screening and prevention Mammography Colorectal cancer screening Colorectal surveillance for high-risk patients Influenza immunization (elders, chronic disease) Pneumococcal immunization (elders, chronic disease) Lead level screening, children HPV vaccine, adolescents Tdap vaccine, adolescents Meningococcal vaccine Papanicolaou test (interval corresponding to risk level) Document smoking status Smoking cessation counseling (if smoking on problem list) Discuss prostate cancer screening Disease management Diabetes Eye examination Foot examination Microalbuminuria testing A1C testing A1C out of goal range, consider management change Moderate-dose statin Fasting lipid profile LDL out of goal range, consider management change ACE/ARB (if microalbuminuria or renal disease) Coronary heart disease Aspirin β-Blocker Statin Fasting lipid profile LDL out of goal range, consider management change Hypertension (BP out of goal range, consider management change) Heart failure Measure ejection fraction ACE/ARB (if EF <40%) β-Blocker (if EF <40%) Asthma Inhaled steroid (persistent asthma only) Asthma action plan ACE, angiotensin-converting enzyme; ARB, angiotensin receptor blocker; BP, blood pressure; EF, ejection fraction; HPV, human papillomavirus; LDL, low-density lipoprotein.
Sex Male 32,404 Female 49,555 Age (years) 0–9 6,539 10–19 6,388 20–29 12,198 30–39 15,060 40–49 15,216 50–59 12,734 60–69 7,843 70–79 3,292 80–89 1,942 ≥90 747 Variable Odds Ratio 95% Confidence Interval Months since CRS launch 1.005 1.0050–1.0058 Number of clinical problems 1.17 1.1699–1.1755 Number of prompts 1.013 1.01071–1.0149 Age (years) 1.001 1.0008–1.0013 Sex* 0.643 0.6283–0.6590 Sex–months interaction 1.003 1.0029–1.0038 ↵* Female = 1; male = 0.
CRS, clinical reminder system.




{kind=link}
{kind=link}
{kind=link}