
Article Figures & Data
Figures
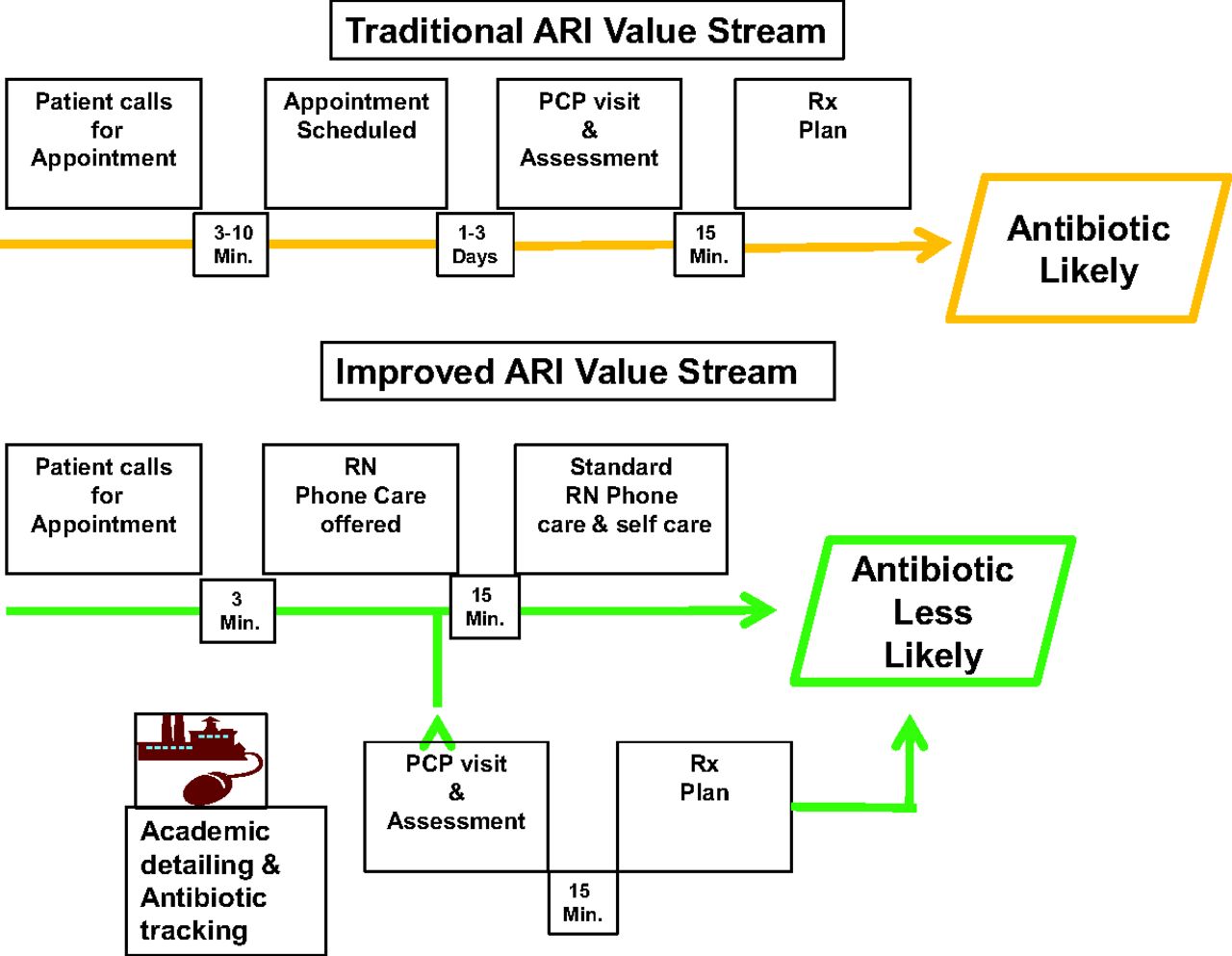
- Figure 1.
Traditional and improved care pathways for acute respiratory infection (ARI). PCP, primary care provider; Rx, prescription; RN, registered nurse.
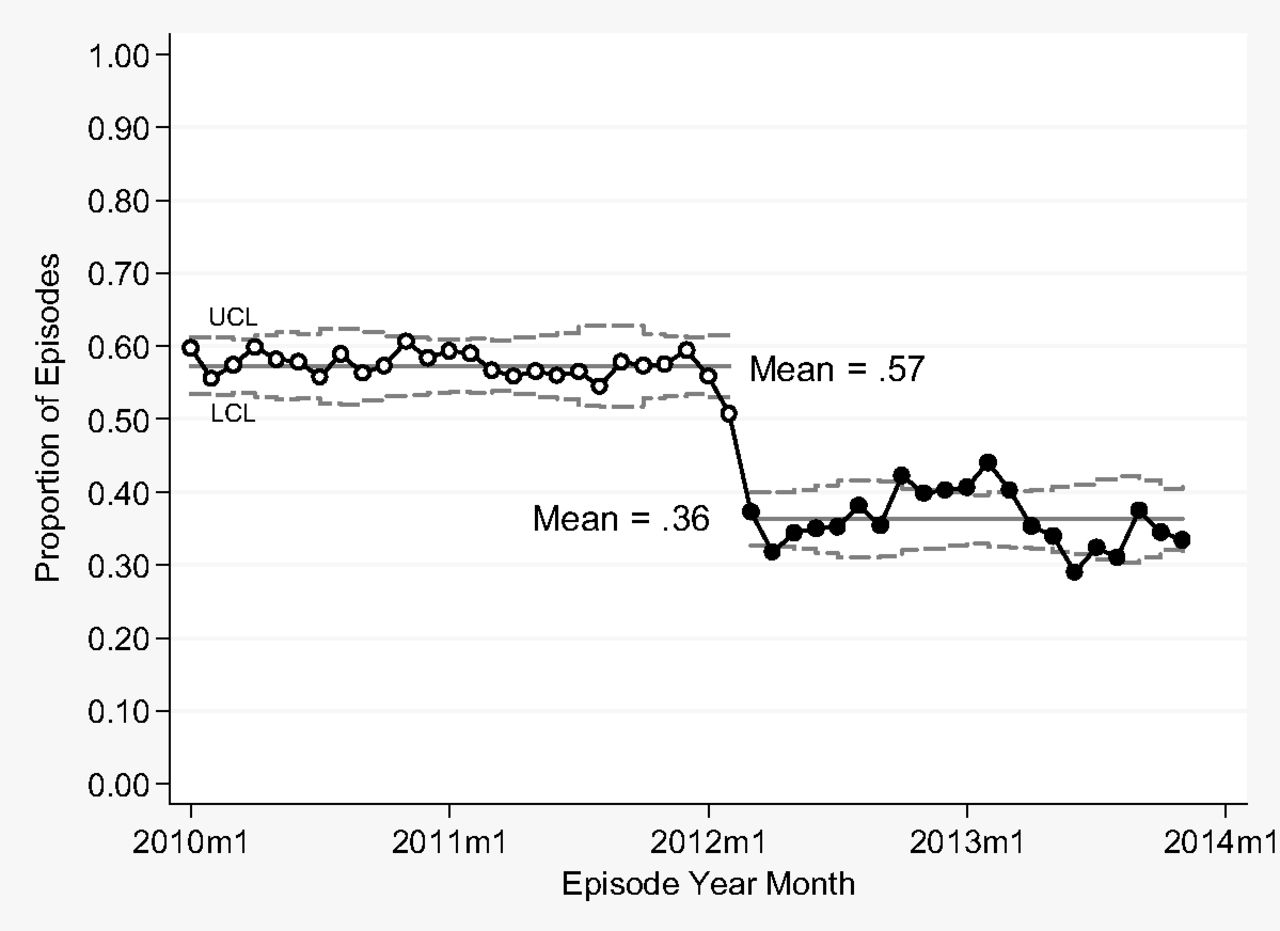
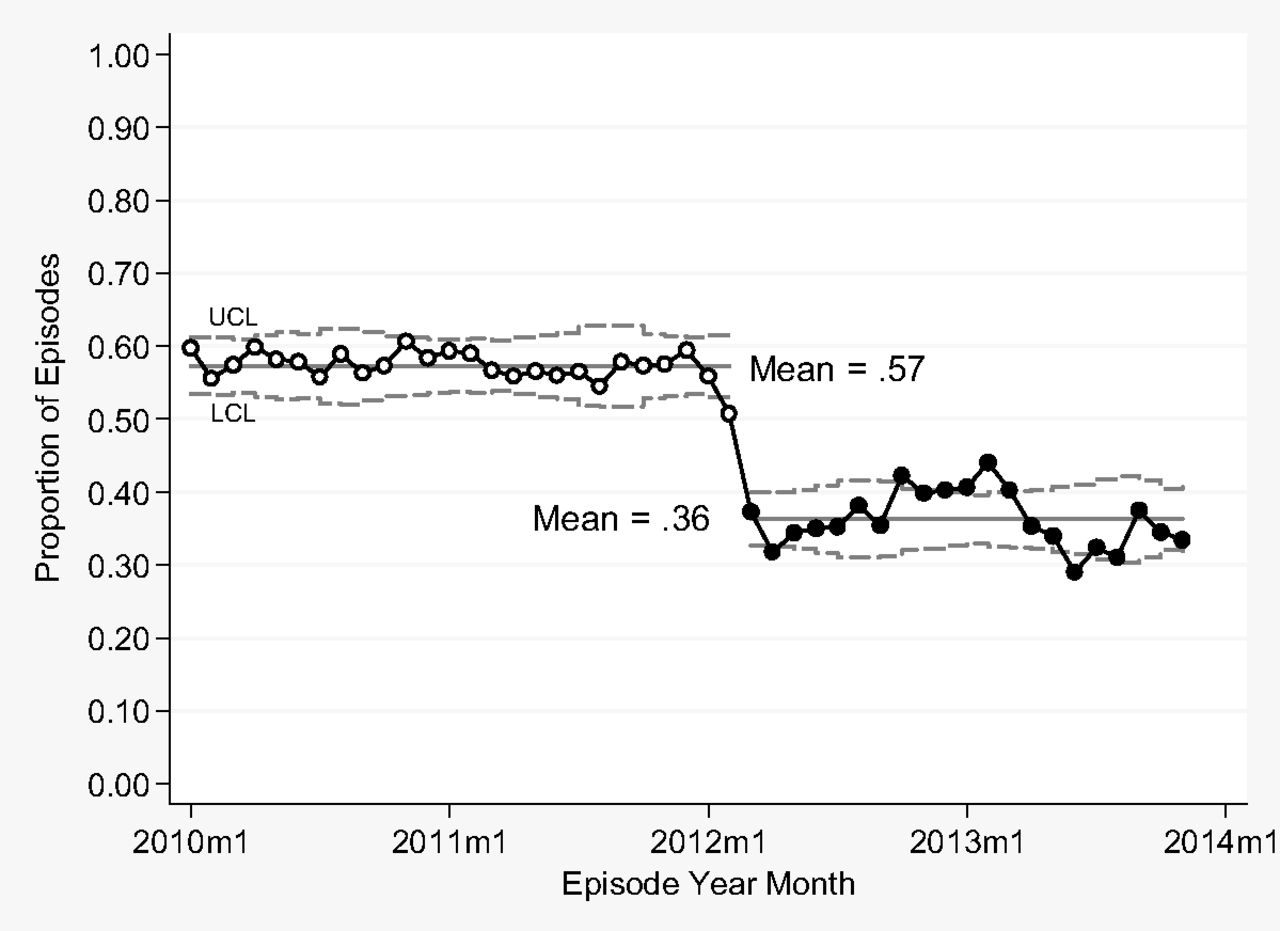
- Figure 2.
Statistical process control P-chart for antibiotic rate by month, January 2010 to November 2013, including both provider visits and nurse provided phone care.
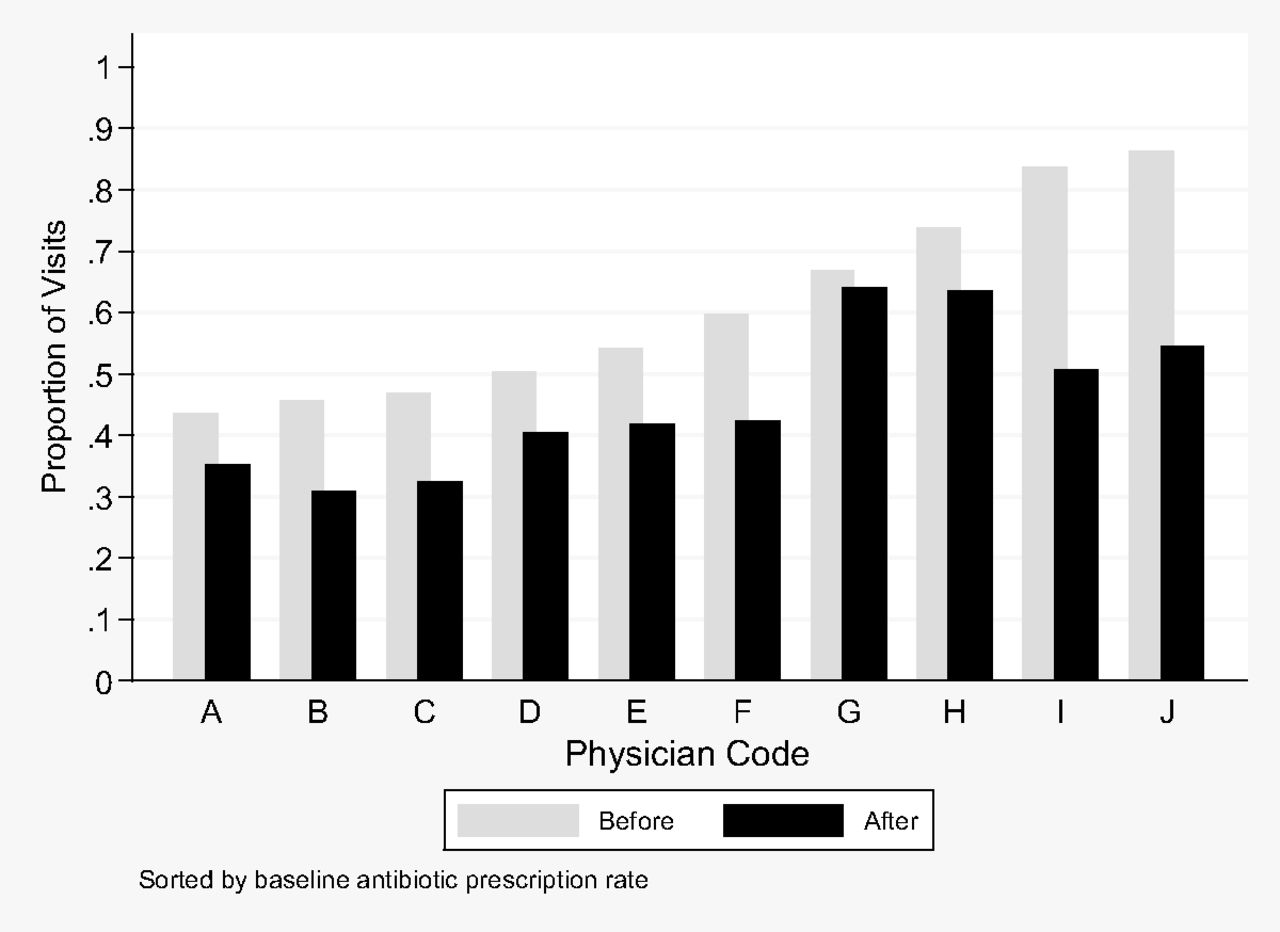
- Figure 3.
Proportion of antibiotics for visits for acute respiratory illness (ARI) by established patients before and after the ARI value stream intervention, for 10 providers with the highest volume (N = 12,083 visits). All differences were significant (P < .001) except provider G (P = .30).

Tables
Variable Total Before Intervention (January 1, 2010 to February 28, 2012) After Intervention (March 1, 2012 to November 30, 2013) P Value Number (total) 56,266 32,497 23,769 Number per month 1,155 1,250 1,132 .25 Age, mean years (SD)* 52.1 (16.4) 51.4 (16.1) 53.2 (16.7) < .001 Gender (% female)* 34,678 (64) 20,845 (64) 13,833 (63) .12 Diagnosis code (%)* < .001 Sinusitis 16,932 (31) 11,102 (34) 5830 (27) < .001 Cough 9,344 (17) 4,567 (14) 4,777 (22) < .001 Acute bronchitis 6,649 (12) 5,217 (16) 1,432 (7) < .001 Other ARI 21,358 (39) 11,611 (36) 9,747 (45) < .001 ↵* In the 54,283 with provider visits.
ARI, acute respiratory illness; SD, standard deviation.
Cost Area Cost Detail ‖Cost Estimate Calculations Cost savings for nursing phone care per year* ARI-related clinic visits Visits avoided (21 months)‡ 1983 Visits avoided per year (95% CI for sensitivity analysis) 1,133 (1,101, 1,159) Avoided visit average cost $133 Estimate avoided clinic visit costs per year (range in sensitivity analysis from 95% CI of visits avoided) $150,708 ($146,433, $154,147) Antibiotics Antibiotics avoided per year through nursing phone care 1133 × 0.56§ = 635 Average cost of antibiotic $9.61 Estimate avoided cost per year (range from 95% CI of visits avoided above) $6,098 ($5,925, $6,237) Total (range in sensitivity analysis) Costs avoided $156,806 ($152,358, $160,384) Cost savings for academic detailing per year* Antibiotics Antibiotics avoided per year through academic detailing (number of ARI visits × difference in antibiotic rate before and after intervention) 13,584 × 16.5%=2,241 Sensitivity analysis on antibiotics avoided from 95% CI for difference in antibiotic rate (from text) 13,584 × 12.5%=1,698 13,584 × 20.5%=2,785 Average cost of antibiotic $9.61 Total (range in sensitivity analysis) Antibiotic costs avoided $21,539 ($16,317, $26,763) Cost for academic detailing† Start-up costs Training (2-day course on academic detailing, including tuition, lodging, salary, and travel for physician and pharmacist one-time cost, amortized) $4,391 Annual costs Benchmark data computer program development (8 hours per year) $438 Preparation and presentation of academic detailing to providers (yearly cost: 32 hours for physician, 50 hours for pharmacist) $13,265 Provider cost to receive detailing per year (2 hours per provider (70 ± 9 providers) with 24 receiving an additional hour) $17,098 ($15,220, $18,975) Total per year (including amortized start-up costs) $35,192 ($33,315, $37,069) Cost expenditures for nursing phone care per year† Nurse-provided phone care Two nurse salaries per year $161,680 Percent of phone care for ARI (95% CI) 46.8% (45.7%, 47.8%) Total (range in sensitivity analysis) Estimate added cost per year $75,666 ($73,888, $77,283) Total savings to health care payers per year* Cost savings from visits avoided (from above) $156,806 ($152,358, $160,384) Antibiotic costs avoided (from above) $21,539 ($16,317, $26,763) Overall annual savings at Virginia Mason (range in sensitivity analysis) $178,345 ($168,675, $187,147) Annual savings per 1,000 episodes of ARI at Virginia Mason (range in sensitivity analysis) $13,129 ($12,417, $13,777)) Total cost to delivery system per year Nursing phone care costs (from above) $75,666 ($73,888, $77,283) Academic detailing costs (from above) $35,192 ($33,315, $37,069) Total costs $110,858 ($107,203, $114,352) Total savings to health care payers per year if nurse care and academic detailing were reimbursed $67,487 ($54,323, $79,944) ↵* Cost analysis from the payer perspective.
↵† Cost analysis from the healthcare delivery perspective.
↵‡ Number of patients with nurse phone care without subsequent provider visit.
↵§ Baseline rate of antibiotic use.
↵‖ Values represent estimated cost savings and expenditures.
ARI, acute respiratory illness; CI, confidence interval.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Barriers and facilitators to reduce low-value care: a qualitative evidence synthesis
- Effectiveness of standardised preoperative assessment and patient instructions on admission blood glucose for patients with diabetes undergoing orthopaedic surgery at a tertiary referral hospital
- Effectiveness of a multi-component quality improvement intervention on rates of hyperglycaemia
- Data Supporting Key Components of Family Medicine--Scope, Continuity, Interprofessional Care, and More