
Abstract
Introduction: To address unnecessary use of antibiotics for uncomplicated acute respiratory infection, we implemented a standardized care pathway composed of: (1) academic detailing of primary care providers, and (2) telephonic care from nurses.
Methods: To evaluate the intervention, we performed a retrospective time series study and cost analysis at a primary care provider network in the Pacific Northwest with 118 providers at seven sites. The main outcomes were: (1) antibiotic rate, (2) provider visits avoided, and (3) cost savings from the payer and health care system perspectives. Data were collected for January 2, 2010 to November 30, 2013, with the interventions occurring on March 1, 2012.
Results: There were 54,283 acute upper respiratory infection visits (34,678 [64%] female; average age, 52.1 years). After the intervention, nurse phone consultation involved 13.8% (3,289 of 23,769) of care episodes. The intervention was associated with a 16.5% absolute decrease in antibiotic rate (95% CI, −0.205 to −0.125; P < .001), after adjustment. Post intervention, 1983 of 23,769 (8.3%) episodes did not require any provider visit (1,133 per year). Single institution cost savings to payers exceeded $175,000.
Conclusions: Implementation of nurse phone care and provider academic detailing was associated with lower inappropriate antibiotic usage and fewer unnecessary provider visits.
Acute respiratory infection (ARI) is the third most common reason for outpatient medical care visits in the United States,1 responsible for >50 million provider visits per year from 1995–2006.2 Most ARIs are self-limited viral illnesses that are not responsive to antibiotics, with antibiotics only considered appropriate if there are signs of pneumonia (eg, rales, high fever), bacterial sinusitis, or other bacterial infection.3,4,5 Evidence-based care for ARI therefore focuses on symptomatic relief, generally with nonprescription cough suppressants and decongestants,5 for which a provider visit is unnecessary.
Despite lack of efficacy, antibiotic prescription for uncomplicated ARI is common, occurring in up to 46% of provider visits,7 resulting in high cost to the health care system as well as potential adverse effects for the individual.3 Further, unnecessary antibiotic use contributes to increase in antibiotic-resistant organisms, exacerbated by the use of broad-spectrum antibiotics in >50% of prescriptions.7 Unnecessary prescription of antibiotics for ARI is driven by many factors, including patient expectations,8,9 physician training and specialty,10 insurance coverage,11,12 and direct-to-consumer drug advertising.13 Avoidance of antibiotics in ARI is now recognized as an indicator of quality in primary care practice.14
Efforts at improving the appropriateness of antibiotic use have focused on addressing provider training through academic detailing, including presentation of evidence to providers on the appropriate and inappropriate use of antibiotics for ARI, often coupled with feedback on group and/or individual antibiotic prescribing rates. Academic detailing has been shown in several studies to be moderately effective in decreasing unnecessary antibiotic prescription.15,16
We also identified that the face-to-face provider visit in ARI may also potentiate the use of unnecessary antibiotics, and may not be necessary. Since uncomplicated ARI is a self-limited illness, patients with uncomplicated ARI may receive telephone care from nurses, without the possibility of antibiotic prescription, and avoid unnecessary provider visits. Nurse phone care has been previously explored in other settings, including pediatrics, adult primary care, and emergency/acute care,17⇓⇓–20 with variable results. In 2002, Richards18 reported a randomized clinical trial of nursing phone care for minor illnesses and identified decreases in the number of patients requiring immediate provider visits. However, they also reported a greater number of patients in the nurse care arm requiring provider visits for follow-up care.18 Implementation of an urgent care phone service as part of the National Health Service in Great Britain, in contrast, was not associated with significant changes in the number of subsequent provider visits.20
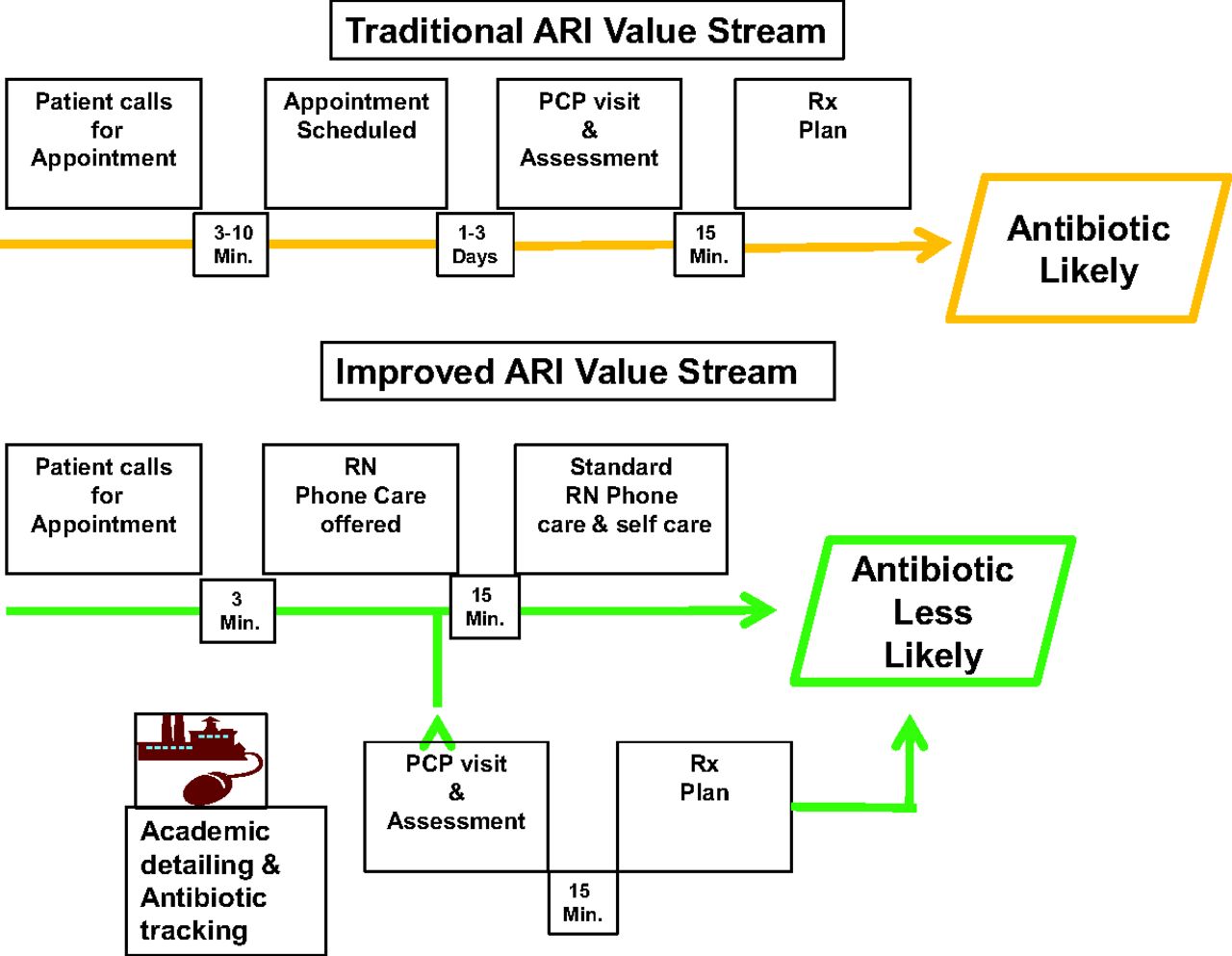
To provide evidence-based care for patients with ARI, but without unnecessary provider visits and unnecessary antibiotics, we developed and implemented a new ARI care pathway (Figure 1). Patients with uncomplicated ARI were offered telephone consultation with a nurse instead of a provider office visit. In addition, we engaged in academic detailing of our primary care providers around the appropriate indications for antibiotic in ARI. The purpose of this study was to examine the effectiveness and cost impact of this ARI care pathway.

Traditional and improved care pathways for acute respiratory infection (ARI). PCP, primary care provider; Rx, prescription; RN, registered nurse.
Methods
This study was conducted as part of a quality improvement project and was considered exempt from review by our institutional review board. The setting was seven urban and suburban outpatient primary care clinics with 118 primary care providers from a single health system in the Pacific Northwest.
The quality improvement intervention was developed and implemented using lean principles and encompassed academic detailing and nurse phone care, targeted at root causes of inappropriate antibiotics. We provided academic detailing to all institutional primary care providers, which included education on appropriate indications for antibiotic treatment in ARI, tracking, and local benchmarking of provider antibiotic prescription rates, in January through April 2012, with additional coaching and feedback to 24 physicians with high antibiotic prescribing rates and high patient volumes. Academic detailing took place at regularly scheduled primary care section meetings by the physician and pharmacist running the program at each of the seven clinics. At each site, the presentations included slide presentations with summaries of the medical evidence and guidelines, as well as benchmark data on the institution and the individual providers, with trends. The presentation also included a summary of the regional Washington Health Alliance “Community Checkup,” which provided a comparison of our institution to other regional groups. We estimate that 60–80% of providers attended each session. The additional coaching was primarily through individual email between the project lead provider and each selected provider. This correspondence was more of a conversation, with provision of individual data and reinforcement of the evidence base for the lack of need for antibiotics.
Under the ARI care pathway, we offered established patients who called to schedule visits for ARI-related symptoms nurse phone care instead of provider visits. Established patients were those who had been seen by one of our primary care providers in the past 24 months. Scheduling clerks followed standard telephonic templates to identify appropriate patients and offer nursing phone care. Phone care was immediate from one of two onsite call center nurses, with patients retaining the option to schedule a subsequent provider visit. For lower-risk patients, nursing phone care consisted of confirmation of uncomplicated ARI, patient education about the self-limited nature of the disease, and counseling regarding self care including nonprescription analgesics and decongestants. The triage protocol and counseling was defined on a standard nursing triage tool (appendix) that was developed based on published nursing triage sources.6,21 Phone care nurses did not prescribe antibiotics or other medications. For higher-risk patients (age >65 years, immunosuppression, or chronic illness including chronic obstructive pulmonary disease, diabetes, or heart failure, or pregnancy) and those with markers of more serious illness (fever ≥101°F, severe throat, ear, or sinus pain, or other symptoms suggesting pneumonia, influenza, or pertussis) nurses scheduled provider visits, on the same day when possible. Implementation of nursing phone care was completed by March 1, 2012, which served as the implementation date for this study. Before this date, nurse phone care was limited to management of chronic illnesses rather than acute conditions such as ARI. Patients were scheduled for appointments by clerks without nurse or provider involvement.
To determine the effectiveness of the ARI care pathway, we performed a retrospective cohort study with time series analysis. The analysis included established patients 18 years old and older who visited or phoned an outpatient clinic for ARI-related symptoms between January 2, 2010 and November 30, 2013. ARI was defined as acute sinusitis (primary diagnosis ICD9 codes 461 and 473), cough (786.2), bronchitis (466 and 490) or other upper respiratory infection (460, 464, and 465), based on the criteria for eligibility for nurse phone care, and adapted from previous research on antibiotics in ARI.22 Influenza, otitis media, and pharyngitis were excluded. This broad definition of ARI was used to avoid confounding from changes in physician coding behavior during the course of the study.
The primary outcome was the antibiotic rate, defined as the number of acute respiratory infection visits that resulted in an antibiotic prescription as a proportion of the total number of episodes of ARI for which an established patient received care (either by nursing phone care or provider visit). Before the intervention, the number of episodes was equal to the number of provider visits for ARI. However, after the intervention, the number of episodes was the number of visits plus the number of visits avoided, determined from the number of patients who underwent nurse phone care without a subsequent primary care provider visit for any reason within 28 days. This outcome demonstrates the combined effects of the academic detailing and nurse phone care. As secondary outcomes, we also report the number of ARI visits avoided, the total number of ARI primary care visits, and the rate of antibiotic prescribing for individual physicians before and after the intervention. All data were extracted from the electronic medical record, including demographics, visit codes, and medication prescriptions, and from nursing call logs when no provider visit occurred. We also confirmed through review of the electronic medical record that no patients in the nurse phone care cohort required subsequent care at our emergency department or urgent care centers.
The results were analyzed using statistical process control charts and time series regression models. In the time series regression model, we adjusted for the effects of seasonal variability in ARI and underlying temporal trend toward decrease in antibiotic rates independent of the intervention. In addition, we adjusted for autocorrelation in the regression time series using the Prais-Winsten approach in STATA v.12.0 (College Station, TX).
We also performed cost analysis of the program, based on the incremental costs (or savings) compared with not having the new ARI care pathway. However, because costs vary depending on the perspective of the analysis, we performed separate analyses from the perspective of the health care payer (ie, health plan, government), and the health system delivering care. From the perspective of the health care payer, costs (or savings) included the incremental cost savings from decreased ARI-related clinic visits and prescribed antibiotics. We determined the total number of provider visits (including the initial visit and any subsequent visits within 28 days) and antibiotic prescriptions (within 28 days) under the ARI care pathway, and compared them to baseline measures before the intervention. We assumed clinical outcomes were unchanged, as uncomplicated ARI is a self-limited illness.3⇓⇓–6
Cost analysis from the health care delivery system perspective included, in addition, the cost of nurses to perform the phone care, and cost of the academic detailing program. We assumed in the analysis (and confirmed with our data) that primary care providers were in shortage, and that visits avoided for ARI would be replaced by visits for other patients for appropriate non-ARI care, thus incurring no cost to the health care system. Because the nurses were already on site at the call center, and because we attempted to be conservative in our cost estimation, we included nurse salaries, but did not include indirect costs (ie, office space) for the nurses in our cost estimates. We also estimated the startup and maintenance costs for the program. These included the initial costs for training the provider and pharmacist responsible for the academic detailing (through attendance at a 2-day national meeting), as well as the annual costs for the academic detailing itself. The academic detailing took approximately 2 hours for each provider, generally combined with section meetings. An additional 24 providers received an additional hour of one-on-one training from the physician running the program. Total time for the physician leading the academic detailing was approximately 32 hours per year, and for the pharmacist was approximately 50 hours per year. There was no additional cost to the system for measurement of antibiotic rates, given that this information is already collected and publically reported as part of the regional Washington Health Alliance Community Checkup.23 However, some computer systems analyst time was required to be able to provide this information for the benchmarking in a timely manner.
Costs of ARI-related clinic visits were estimated from the average private insurance payment for a primary care visit in the United States, adjusted to 2012 dollars.24 Antibiotic costs were estimated from the medication national average retail price.25 Because of the many assumptions and uncertainty in the estimates, we performed one-way sensitivity analyses based on the 95% CIs of the major estimates, including the number of visits prevented, antibiotics prevented, number of physicians undergoing academic detailing, and nursing time devoted to phone care.26 We did not discount due to the short timeframe of the analysis.
Nursing costs were estimated by time motion study of the call center nurses and the nursing call logs. Individual nurses were observed and timed, for a total of 32 hours. The annual nursing cost for ARI phone care was then calculated from the proportion of nurse time spent on ARI phone care multiplied by the average annual wages for nurses. Annual nursing wages were determined from the US Department of Labor, Bureau of Labor Statistics Occupational Employment Statistics for May 2012.27 Analyses were performed using StataMP v.12. (College Station, TX).
Results
Between January 2, 2010 and November 30, 2013, there were 54,283 patient visits for ARI to primary care at one of the seven study clinics. The mean age of the patients with a visit to any of the clinics was 52.1 years and 34,678 (64%) were female. Patients were somewhat older (53.2 vs 51.4 years, P < .001) postintervention. The frequencies of the primary clinical diagnoses were 16,932 (31%) sinusitis, 9,344 (17%) cough, 6,649 (12%) acute bronchitis, and 21,358 (39%) acute ARI, with significant changes in use of specific diagnosis codes before and after the intervention (Table 1). There were 118 primary care providers, including 100 family practice and general internal medicine physicians (84.7%), 11 nurse practitioners (9.3%), and seven physician assistants (5.9%). The providers had completed professional school an average of 20 years prior (range, 1 to 40 years), were 57% female (67/118), and had an average age of 48 years. The median number of patient visits per provider in the study time frame was 383.
Overall, the proportion of ARI-related clinic visits with antibiotics was 51% (27,427/54,283). The antibiotic rate varied by clinical diagnosis, with antibiotics prescribed for sinusitis in 89% (15,047/16,932), for bronchitis in 73% (4,886/6,649), for cough in 31% (2,929/9,344), and for other ARI in 21% (4,565/21,358). The proportion of visits with antibiotics was also related to age; 52% (22,151/42,438) of patients less than or equal to age 65 years received antibiotics, whereas only 45% (5,276/11,845) of patients greater than 65 years old received antibiotics (P < .001).
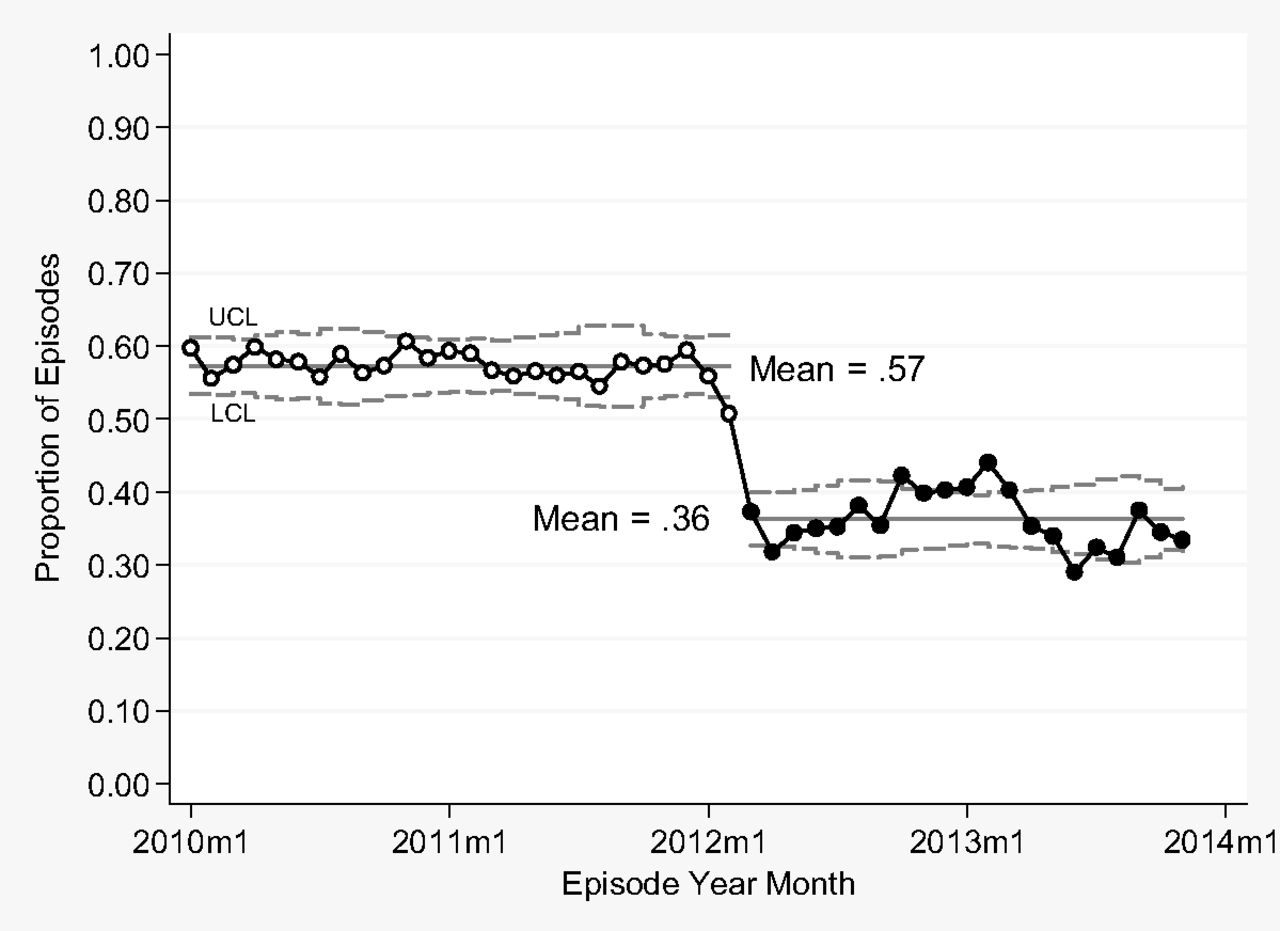
For the primary outcome, the ARI value stream was associated with a 29.4% decrease in the antibiotic prescribing rate per episode of ARI (absolute decrease −16.5 percentage points, 95% CI: −20.5, −12.5; P < .001), following adjustment for seasonality and underlying trend toward decrease in antibiotic prescribing. The unadjusted decrease was 36.7% (absolute decrease −21.0 percentage points, 95% CI, −22.8, −19.2; P < .001, Figure 2). The winter season (October to March) was associated with a 4.2% higher antibiotic prescribing rate (absolute increase 0.023 percentage points, 95% CI, 0.0050, 0.041; P = .014). There was a small but statistically significant decrease in antibiotic rate over time before the intervention (−0.0017 percentage points per month, 95% CI, −0.032, −0.0025; P = .0023).
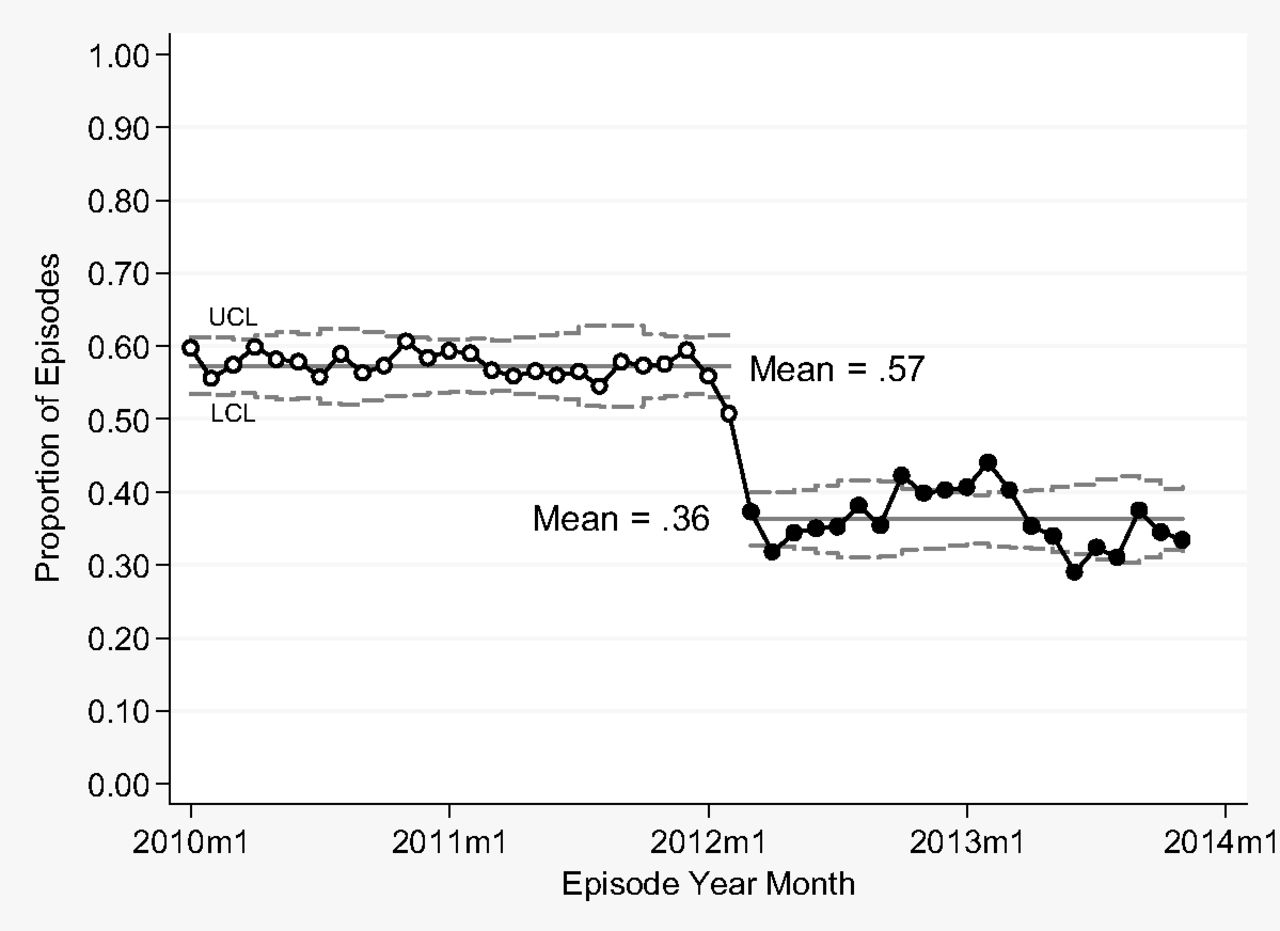
Statistical process control P-chart for antibiotic rate by month, January 2010 to November 2013, including both provider visits and nurse provided phone care.
During the intervention period, nurse phone care involved 13.8% (3,289 of 23,769) of ARI care episodes, of whom 1306 had a clinic visit with a ARI-related primary diagnosis within 28 days of the phone call, leaving 1983 (8.3%) of all 23,769 ARI episodes in which patients underwent phone care without a visit (provider visits avoided). The mean number of days from the phone call to the clinic visit was 1.0 days, with a majority of visits (77%) occurring on the same day or the next day after the phone call. We found no evidence that patients who underwent initial nurse phone care required more subsequent health care.
The total number of ARI episodes did not change significantly after the intervention (1250 to 1132 per month, decrease of 9.4%, P = .25). However, the total number with provider visits (exclusive of phone care) did decrease 17.0% (from 1250 to 1037, P = .035). This decrease in the number of provider visits occurred despite a moderately severe flu season in 2012 to 2013 following the intervention.28 The rate of antibiotic prescribing among patients with provider visits and the change at the time of the intervention varied between providers (Figure 3), with all high-volume providers demonstrating decreases.
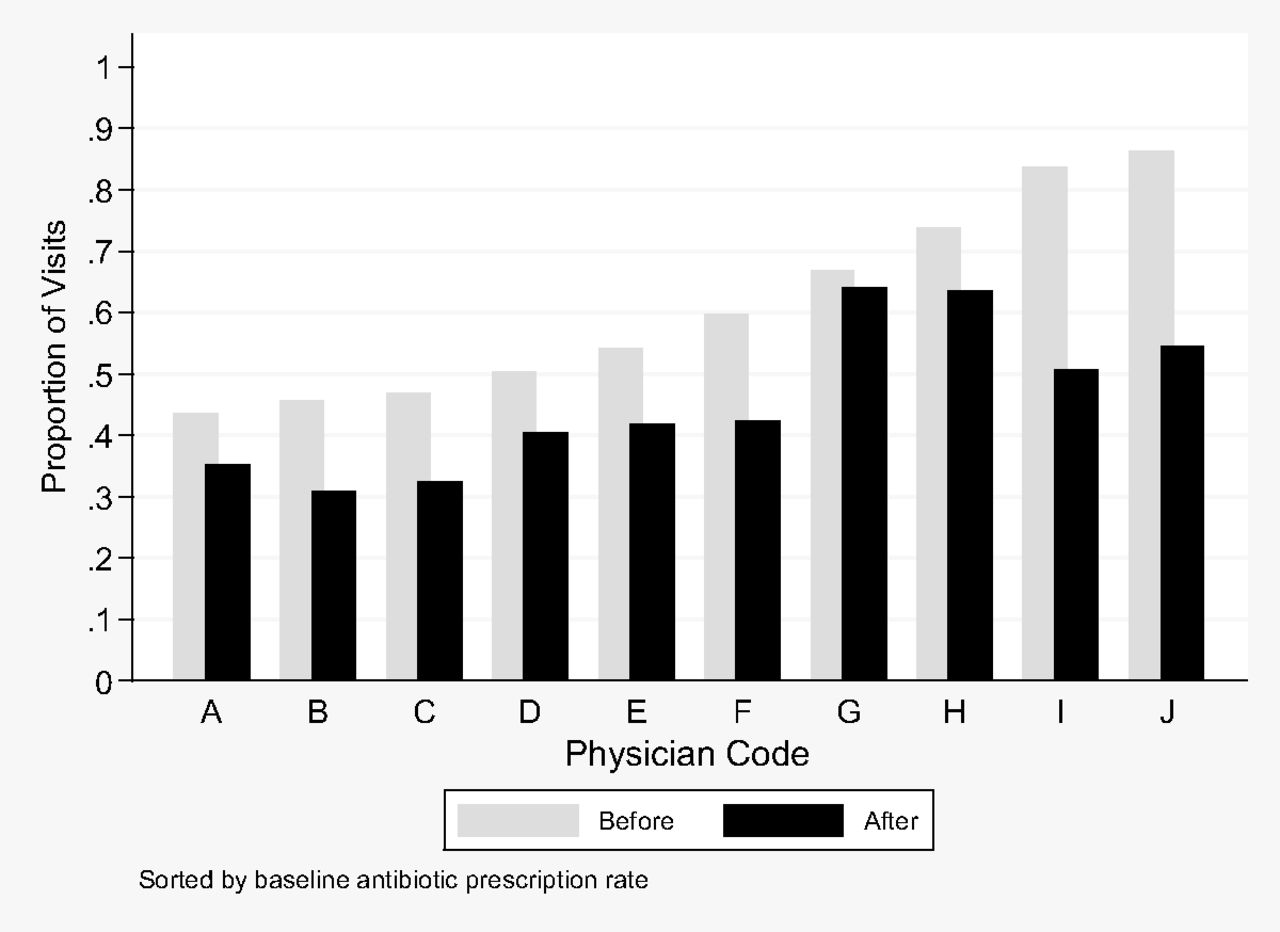
Proportion of antibiotics for visits for acute respiratory illness (ARI) by established patients before and after the ARI value stream intervention, for 10 providers with the highest volume (N = 12,083 visits). All differences were significant (P < .001) except provider G (P = .30).
Cost savings from the ARI value stream accrued to health care payers (including both health plans and patients) through avoidance of 1133 provider visits and 635 antibiotic prescriptions in the first year of the ARI value stream totaled greater than $156,000. Additional savings from academic detailing included decreased costs from avoided antibiotic prescribing of an estimated $22,000 per year, for total annual cost savings of $178,000. From the perspective of the health care delivery system, the ARI value stream resulted in added nursing costs of approximately $76,000 per year (Table 2), based on 46.8% (4055/8672, 95% CI, 45.7%, 47.8%) of calls to the nurses being for ARI. In addition, the cost of academic detailing for the providers (including training of the academic detailing team, provider time, and computer system analyst time was approximately $35,192 per year) (Table 2). Total savings even after reimbursement for nursing and academic detailing costs was an estimated $67,000 per year.
Discussion
Improving the quality of health care can be dependent on doing less rather than more, and often improving quality results in lower cost.29⇓–31 In this article, we demonstrate that implementing a standardized ARI care pathway focused on academic detailing of providers and providing nurse phone care instead of provider visits is associated with a decrease in unnecessary antibiotic prescription, unnecessary provider visits, and lower health care costs. We focused on eliminating the opportunity for the antibiotic prescription through avoidance of unnecessary provider visits. Applying the lean principle of mistake proofing,32 we identified the provider visits as both requisites for unnecessary antibiotic prescription, and unnecessary for quality care. By preventing this visit, we prevented the opportunity for the mistake to occur. Because the intervention occurs at the time of scheduling, before provider involvement, we succeed in lowering antibiotic prescription rates even among providers who are not responsive to academic detailing. Our findings are supported by previous reports in the pediatric literature detailing decreases in antibiotic rates for ARI attributable at least in part to decreasing numbers of provider visits.2,33
The setting likely affected the success of the project. The intervention was performed at a single health care system, with a strong focus on quality improvement, and nurses, and staff who are all salaried employees, making for aligned incentives. Lean concepts, 34⇓–36 including standard work and mistake proofing, are familiar to our staff and providers, enhancing our ability to effect change.
We acknowledge the limitations of our analysis. We are unable to determine whether patients in the study received care at other institutions. However, we did limit the analysis to individuals who were established patients to decrease the likelihood of care at other sites. A concern with telephonic care is that patients will not receive provider visits when they are necessary, resulting in worse health outcomes. We believe this to be unlikely for several reasons. First, we offer nurse phone care only to patients who meet predefined low-risk criteria, where antibiotics are unnecessary.3,4 In addition, the nurses elicit histories from the patients and schedule provider face-to-face appointments when indicated. Patients are given the option to call back for a provider visit if symptoms worsen or do not improve. Thus, the program does not provide a substantial barrier to patients seeing providers subsequent to the nursing care. We also may have underestimated the value of the intervention as there is education for the patients that occurs in the context of the nurse phone care. We anticipate that this education may lead patients to avoid provider appointments for future episodes of uncomplicated ARI, and therefore also avoid unnecessary antibiotics. In addition, by avoiding unnecessary patient visits we decrease opportunities for patients to spread the cold virus to others. This potential additional benefit could not be captured in our analysis. Finally, the nurse phone care was dependent on availability of a call center nurse, which was not always the case during the busy ARI season, limiting complete implementation.
We were unable to assess patient satisfaction, an important quality indicator. However, the program is voluntary. Patients may elect to proceed with provider visits at any point in the process. Therefore we would anticipate that satisfaction with care would not be adversely affected. In addition, we anticipate patients deriving other benefits, including time savings from not having to travel to a clinic, and potentially not losing wages due to a provider visit. We did not include these in the cost analysis as it is not clear if individuals with ARI symptoms would be or even should be at the workplace. The cost estimates may therefore underestimate the benefit from the societal perspective. The cost analysis from the health care system is more complex, as our cost model is based on excess demand for primary care providers, so that substitution of nurse care for an un-needed provider visits does not result in lower volumes for the primary care providers. This is the case in our market, and nationally, but may not be true at all settings.
The ARI value stream was associated with substantial savings to the health care payer under the current fee for service model. Whereas we estimate $178,000 per year at our institution, if extrapolated to the 44 million visits annually in the United States for ARI, estimated national savings would be greater than $550 million. However, cost analysis varies depending on the perspective of the analysis.26 Neither the ARI value stream nurse phone care nor academic detailing is currently reimbursed under most fee-for-service payment models in the United States. Hence, though these are not costs to the health care payer, they do represent costs from the perspective of the health care delivery system.26 Were health care payers to reimburse for these services, the overall system would still save greater than $200 million per year nationally.
Our institution undertook this intervention as a method to improve care at relatively low cost. In addition, we were motivated by high demand for primary care, contributing to delays for patients seeking care. It is difficult to define a methodology under fee for service health care to identify which nursing calls potentially supplant provider visits and therefore should be reimbursed, versus other calls that are in addition to standard care. However, as systems move toward accountable care organizations and other models with sharing of risk between providers and payers, use of lower-cost nurse phone care and academic detailing may make financial sense for the provider organization. In addition, to financially support these efforts, one could design pay-for-performance or gain-sharing arrangements, whereby payers could reimburse providers for nurse phone care based on the number of calls that did not lead to visits, or for better performance on antibiotic prescribing in ARI.
Although most commonly delivered through traditional face-to-face encounters with providers, more convenient options for care of patients with ARI have increased in popularity.37 These newer options include kiosks in retail stores and feature encounters with midlevel providers in nontraditional settings. Although potentially decreasing costs by using less expensive providers, and improving convenience of care, such approaches carry the disadvantage of potentially leading to higher use of unnecessary antibiotics and increasing unnecessary visits.37,38
An additional potential consequence of implementation of the ARI value stream was the confounding effect on quality metrics. The Washington Health Alliance in our region provides a publicly reported dashboard of health care delivery system quality metrics, including rates of antibiotic prescription in acute bronchitis.23 A similar metric is also employed as part of the Federal Physician Quality Reporting System.14 By avoiding ARI-related provider visits, we effectively decreased the denominator for the quality metric, and may therefore spuriously inflate the prescribing rate. We also believe that the local quality improvement efforts directed at unnecessary antibiotics in ARI may have had the unintended consequence of changing the coding behavior of primary care providers. We observed a change in coding of ARI conditions with lesser use of the acute bronchitis codes later in the study, which may be a response to the Washington Health Alliance public reporting effort.23 To capture all relevant patients and prevent bias from coding changes, our data included a range of possible ARI codes.
In conclusion, implementation of an ARI care pathway with delivery of nurse phone care and academic detailing efforts aimed at decreasing physician antibiotic prescribing was associated with better quality care at lower cost. We observed an 8.3% decrease in the number of provider visits, and a 29.4% decrease in unnecessary antibiotic prescriptions, with substantial savings to the health care system.
Notes
This article was externally peer reviewed.
Funding: none.
Conflict of interest: CCB receives book royalties from Springer Publishing for Evidence-Based Imaging textbooks. The other authors have no conflicts to declare.
- Received for publication July 9, 2014.
- Revision received October 23, 2014.
- Accepted for publication November 10, 2014.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Barriers and facilitators to reduce low-value care: a qualitative evidence synthesis
- Effectiveness of standardised preoperative assessment and patient instructions on admission blood glucose for patients with diabetes undergoing orthopaedic surgery at a tertiary referral hospital
- Effectiveness of a multi-component quality improvement intervention on rates of hyperglycaemia
- Data Supporting Key Components of Family Medicine--Scope, Continuity, Interprofessional Care, and More