
Article Figures & Data
Figures
- Figure 1.
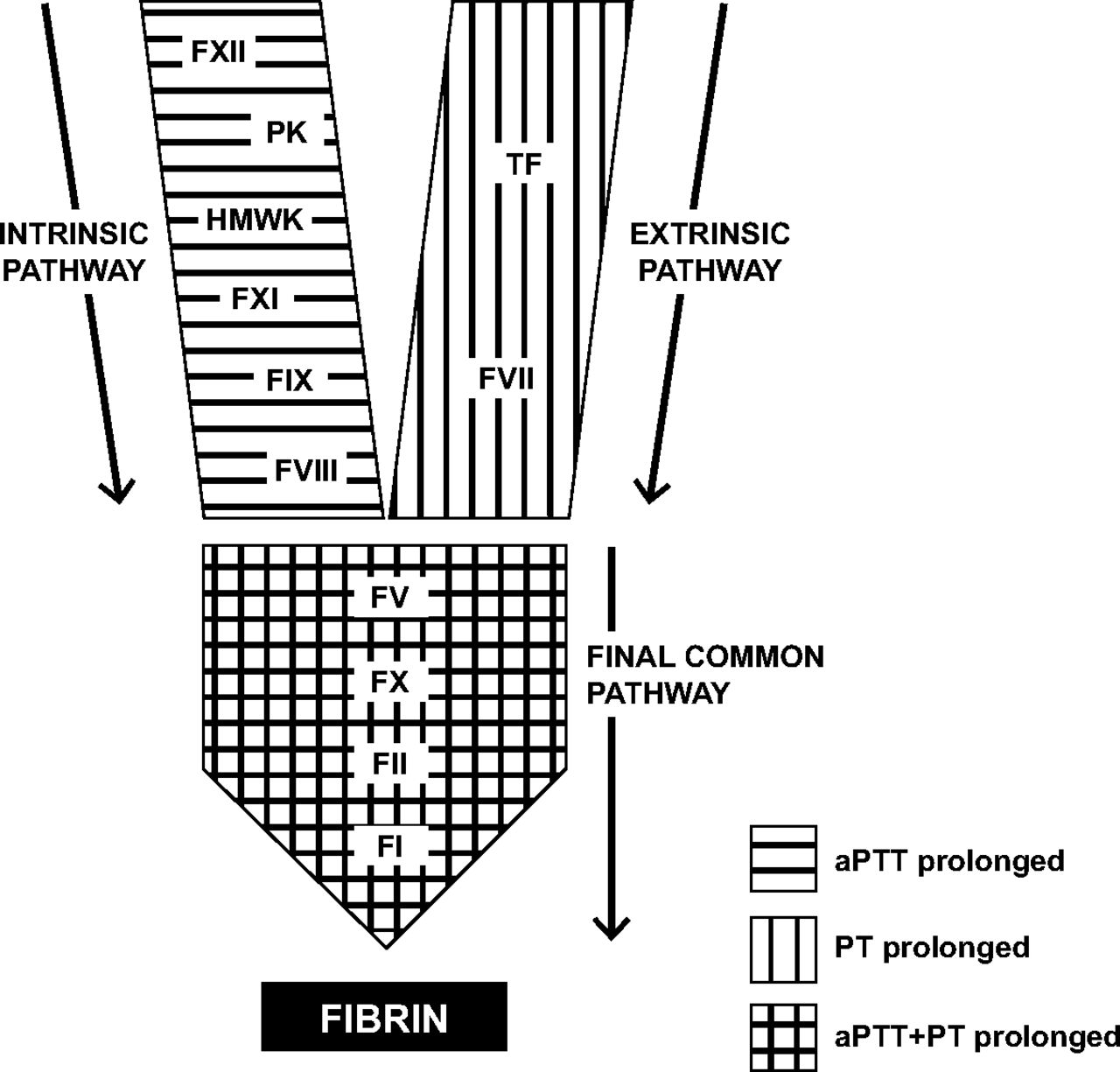
12,29 Simplified schematic of the coagulation “cascade.” The coagulation cascade consists of three pathways: the intrinsic pathway, the extrinsic pathway, and the final common pathway, culminating in the formation of fibrin. This model of coagulation oversimplifies the process of in vivo coagulation but is useful for the correlation of coagulation assay (ie, activated partial thromboplastin time [aPTT], prothrombin time [PT]) abnormalities with specific pathways and, hence, coagulation factors. FI, fibrinogen; FII, factor II; FIX, factor IX; FV, factor V; FVII, factor VII; FVIII, factor VIII; FX, factor X; FXI, factor XI; FXII, factor II; HMWK, high-molecular-weight kininogen; PK, prekallikrein; TF, tissue factor.
- Figure 2.
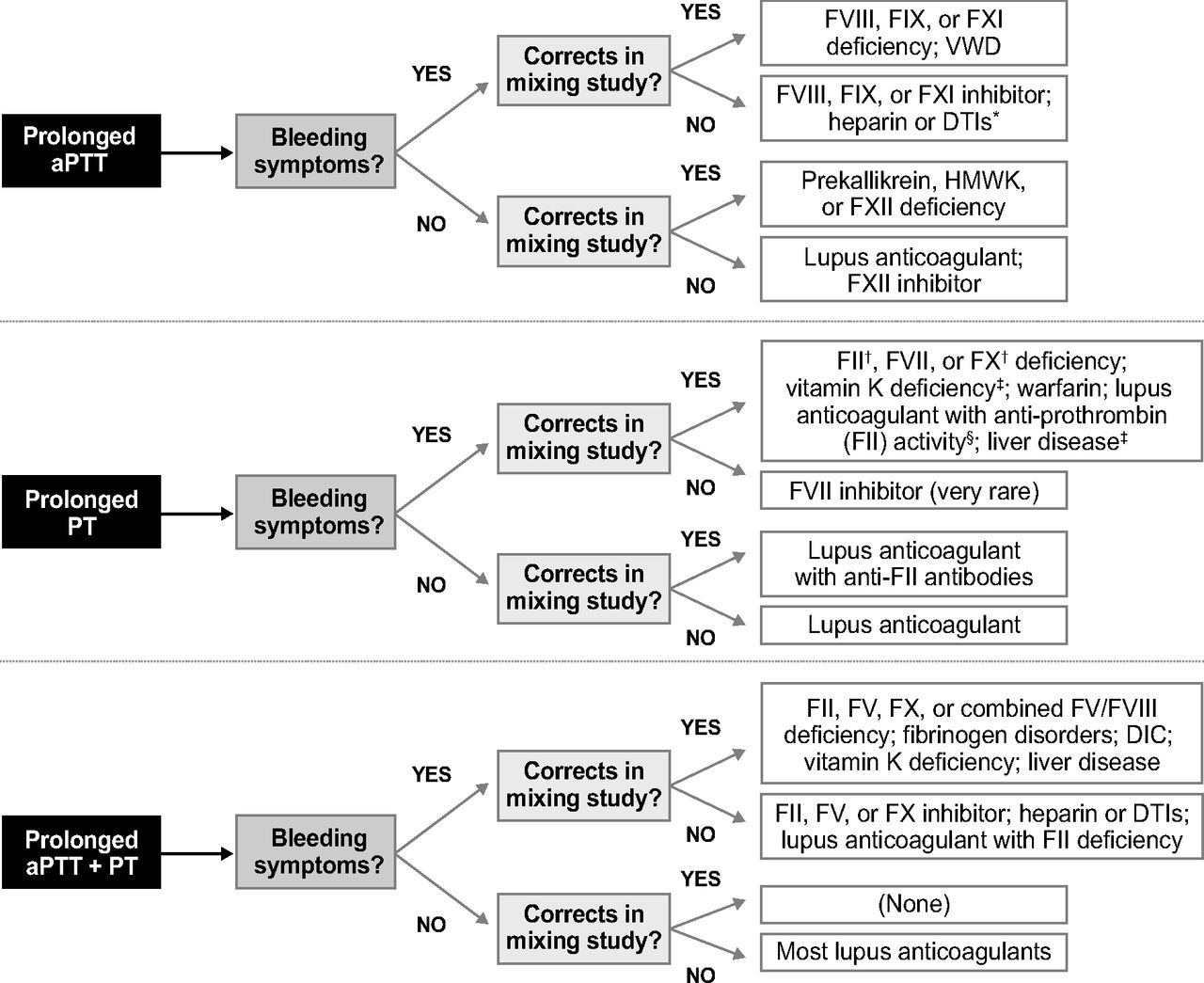
29–32 Differential diagnosis for abnormalities of aPTT and PT. Once the coagulation laboratory study abnormality has been identified, the differential diagnosis may be further narrowed down based on the specific coagulation study abnormalities (activated partial thromboplastin time [aPTT], prothrombin time [PT], or both); the presence or absence of bleeding symptoms; and the results of the mixing study. Note that prolonged incubation may be required for accurate mixing study results. *PT may also be prolonged by heparin (at high doses) or direct thrombin inhibitor (DTIs). †aPTT may also be prolonged in FII and FX deficiencies. ‡aPTT may also be prolonged in the setting of advanced liver disease or vitamin K deficiency. §Applies to 10% of lupus anticoagulants. DIC, disseminated intravascular coagulation; FII, factor II; FIX, factor IX; FV, factor V; FVII, factor VII; FVIII, factor VIII; FX, factor X; FXI, factor XI; FXII, factor XII; HMWK, high-molecular-weight kininogen; VWD, von Willebrand disease.

Tables
Personal history of bleeding and description of bleeding events Frequency Severity (including need for any medical or surgical treatments) Anatomic location Spontaneous or provoked Complete medication history, including OTC medications (many of which contain aspirin or NSAIDs) History of excessive or prolonged bleeding after trauma or surgery (including dental procedures) History of menorrhagia* (including age of onset) or excessive postpartum bleeding in women Family history of any of the above bleeding sequelae or of a known heritable bleeding disorder (or consanguinity in cases of autosomal recessive disorders8) Personal or family history of blood product transfusion and the reasons for transfusion, if known Personal history or symptoms of any conditions associated with coagulopathy (eg, liver disease) or with specific bleeding disorders (eg, malignancy or autoimmune disease in acquired hemophilia) History of recurrent miscarriage in women† Personal or family history of thrombotic events‡ ↵* Menorrhagia is defined by heavy menstrual bleeding of more than 7 days' duration7; >80 mL of blood loss per menstrual cycle7; needing to change sanitary pads or tampons more than hourly11; or passage of clots >1.1 inch in diameter.11
↵† Recurrent miscarriage may be a feature of some congenital factor (eg, factor XIII) and fibrinogen deficiencies.10
↵‡ Arterial or venous thromboses may be a feature of some congenital factor (eg, factor XI, factor VII, fibrinogen, factor V, and factor XIII) deficiencies.9
NSAID, nonsteroidal anti-inflammatory drug; OTC, over the counter.
- Table 2. Differential Diagnosis and Diagnostic Features of Quantitative Platelet Disorders
Mechanism of Thrombocytopenia Differential Diagnosis Comments Impaired production Hematologic malignancies20 Often accompanied by abnormalities in other marrow cell lines (ie, red and white blood cells) Aplastic anemia41 Other marrow cell lines affected as well Myelodysplasia20 May be accompanied by abnormalities in other marrow cell lines; bleeding may occur at higher platelet counts than expected Drugs/toxins41,42 For example, alcohol, chemotherapeutic agents, radiation Viral marrow suppression or damage42 For example, because of EBV, parvovirus, HCV, or HIV Gestational thrombocytopenia43 Generally mild [ie, platelet count >70,000/mL] and self-limited, resolving after delivery; exact mechanism of thrombocytopenia unknown—hemodilution and increased platelet turnover may also contribute Liver disease42 Because of reduced levels of thrombopoietin, which is produced by the liver Nutritional deficiencies42 For example, folate, vitamin B12 Inherited thrombocytopenias16,17,19,41 Often present with incidental thrombocytopenia in adulthood; may have family history of thrombocytopenia or personal history of low platelet counts Destruction or consumption Immune Medication, including heparin (most common), various antimicrobial, antiarrhythmic, anticonvulsant, and antifungal agents, and H2 receptor antagonists41 ITP Along with drug-induced thrombocytopenia, accounts for majority of isolated thrombocytopenia in adults16; typically chronic in adults41; may occasionally be accompanied by Coombs positive hemolytic anemia [Evans syndrome]41 Autoimmune disease41 Infection41,45 For example, HIV TTP in presence of ADAMTS13 autoantibodies41,46 Coombs-negative hemolytic anemia and thrombocytopenia; may or may not have associated renal insufficiency, fever, and mental status changes; neurological symptoms vary, ranging from headache and confusion to seizures and stroke-like symptoms Nonimmune HUS Relatively uncommon but life-threatening cause of thrombocytopenia; classic form consists of microangiopathic hemolytic anemia, thrombocytopenia, and renal failure DIC41 Other hallmark laboratory findings include decreased fibrinogen, elevated fibrin degradation products, and a positive D-dimer Sepsis42 HELLP syndrome44 Serious intrapartum condition characterized by hemolysis and elevated liver enzymes in addition to thrombocytopenia; frequently coexists with preeclampsia; may recur in subsequent pregnancies Physical destruction41,42 For example, valvular disease, cardiopulmonary bypass, cavernous hemangiomas (eg, in Kassabach-Merritt syndrome) Sequestration Splenomegaly41,42 ADAMTS, a disintegrin and metalloproteinase with thrombospondin type 1 motives; DIC, disseminated intravascular coagulation; EBV, Epstein-Barr virus; HCV, hepatitis C virus; HELLP, hemolysis, elevated liver enzymes, and low platelets; HIV, human immunodeficiency virus; HUS, hemolytic uremic syndrome; ITP, idiopathic thrombocytopenic purpura; TTP, thrombotic thrombocytopenic purpura.
- Table 3. Bleeding Disorders and Associated Conditions Presenting With Normal Initial Hematologic Laboratory Study Results
Condition Recommended Screening Tests VWD23* VWF antigen, VWF ristocetin cofactor activity, and FVIII activity assays FXIII deficiency59 Quantitative functional FXIII assay (ammonia-release or amine-incorporation assay) Fibrinolytic disorders (α2-antiplasmin and PAI-1 deficiencies)13,56,57,60 Specific functional (activity) and antigen assays Collagen disorders (eg, EDS, BJHS)58 Hypermobility assessment tools (eg, Beighton score, Brighton criteria)58 ↵* Initial hematologic laboratory studies will be normal in only some cases of von Willebrand disease (VWD). Nevertheless, additional screening tests should be performed before excluding VWD based on a normal activated partial thromboplastin time or Platelet Function Analyzer, when clinically indicated.
BJHS, benign joint hypermobility syndrome; EDS, Ehlers-Danlos syndrome; FXIII, factor XIII; FVIII, factor VIII; PAI, plasminogen activator inhibitor; VWF, von Willebrand factor.
Thrombocytopenia due to impaired platelet production Platelet count thresholds for platelet transfusion Prophylactic transfusion: <10,000/μL* Coverage for invasive procedures Minor invasive procedures (eg, LP, CVC placement, epidural anesthesia, endoscopy with biopsy, or liver biopsy): 50,000/μL† Major surgery in noncritical sites: 50,000–100,000/μL‡ Major surgery in critical sites (eg, eyes, brain): 100,000/μL Active bleeding: 50,000–100,000/μL Autoimmune thrombocytopenia Platelet transfusion should only be undertaken in instances of serious or life-threatening bleeding (eg, gastrointestinal or intracranial hemorrhage) Large amounts of platelets may be required to boost the platelet count, given the shortened survival of the transfused platelets; concomitant administration of immune-modulating therapies (eg, steroids or IVIG) may attenuate this process, resulting in a more rapid rise in platelet count Platelet function disorders For active bleeding or hemostatic surgical coverage Eliminate or mitigate any factors contributing to platelet dysfunction (eg, medications, underlying conditions) Desmopressin may be considered in patients with inherited platelet function disorders, particularly storage pool defects, or in patients with uremia Platelet transfusion may be considered when the above measures are not indicated or are unsuccessful ↵* In some cases, the platelet count threshold for prophylactic transfusion may be higher (eg, in patients with sepsis, acute bleeding, other coagulation abnormalities, or necrotic tumors receiving aggressive treatment) or lower (eg, in patients at risk for platelet alloimmunization or refractoriness because of frequent transfusions).69,70
↵† The threshold for platelet transfusion before bone marrow aspiration and biopsy is unknown.69 It has been suggested that, even in the presence of severe thrombocytopenia, this procedure may be performed without prior platelet transfusion, provided that adequate surface pressure is applied.70
↵‡ Platelet count threshold will vary depending on the type and extent of surgery and presence of factors that may affect platelet function (eg, uremia, medications, extracorporeal circulatory support for surgery, comorbid conditions).69,70
CVC, central venous catheter; IVIG, intravenous immunoglobulin; LP, lumbar puncture.
Product Composition Indications Comments FFP All coagulation factors Multiple factor deficiencies (eg, in DIC, liver disease) May be required in large volumes to sufficiently boost levels of a single coagulation factor FV deficiency (may supplement with platelet transfusions) Not virally inactivated FXI deficiency (in lieu of FXI concentrate when there is a heightened risk of thrombogenicity [eg, in the peripartum period])70 Other single-factor deficiencies when single-factor concentrates or PCCs are unavailable Cryoprecipitate Concentrate precipitated from FFP; rich in FVIII, VWF, FXIII, and fibrinogen72 Used most often to replace fibrinogen72 May be required in large volumes Not virally inactivated PCCs Highly purified concentrates from pooled normal plasma containing FII, FIX, and FX (±FVII)74,75 FII or FX deficiency Virally inactivated74,75 FIX or FVII* deficiencies when single-factor concentrates are unavailable Contain known amounts of each factor74,75 4-factor PCCs are indicated for warfarin reversal Activated PCCs PCC with FII, FIX, and FX (mainly nonactivated) and FVII (mainly in the activated form) Coagulation factor inhibitors† Single-factor concentrates Plasma derived Respective single-factor deficiencies Treatment of choice for single-factor deficiencies, when available FVIII rFVIIa is indicated as a bypassing agent for FVIII and FIX inhibitors,† as well as for replacing FVII in FVII deficiency Risk for human viral contamination is present but exceedingly low in plasma-derived concentrates because of screening and viral inactivation procedures; it is probably nonexistent in recombinant concentrates FVIII/VWF FIX FXIII Fibrinogen Recombinant rFVIIa rFVIII rFIX rFXIII ↵* Only 4-factor prothrombin complex concentrates (PCCs) may be used for replacement of factor VII (FVII); however, 4-factor PCCs are not universally available.
↵† Although single-factor concentrates may be used for respective low-titer coagulation factor inhibitors (eg, plasma-derived or recombinant factor VIII [FVIII] for FVIII inhibitors), bypassing agents are generally recommended for active bleeding (for which they are considered first-line therapy) and for hemostatic coverage during invasive procedures in patients with inhibitors.
DIC, disseminated intravascular coagulation; FFP, fresh frozen plasma; F, factor; PCC, prothrombin complex concentrate; rF, recombinant factor; VWF, von Willebrand factor.
- Table 6. Nontransfusional Therapies for Treatment or Prevention of Bleeding in Patients With Bleeding Disorders
Antifibrinolytics Include ε-aminocaproic acid and tranexamic acid Interfere with the formation of the fibrinolytic enzyme plasmin from its precursor plasminogen First-line therapy in rare disorders of fibrinolysis (α2-antiplasmin and PAI-1 deficiencies)56 Systemic or topical antifibrinolytics may be used alone to treat or prevent mucosal bleeding in patients with coagulation factor disorders, thus avoiding systemic hemostatic therapies1,66–68,73 Effective, first-line therapy for menorrhagia (with or without hormonal therapies)25,80,85 Tranexamic acid used anecdotally in patients with bleeding disorders, including as an adjunct to factor replacement for major surgery in patients with hemophilia78,81,84 and as a sole systemic hemostatic agent primarily for minor procedures1,66 Also used for treatment of bleeding and for hemostatic coverage for minor surgery in patients with platelet function disorders; may be used adjunctively with platelet transfusion and other nontransfusional therapies in these patients83 Theoretical risk for thrombogenesis; may be increased in patients who receive concurrent factor replacement or who have certain bleeding disorders (eg, dysfibrinogenemia, in which antifibrinolytics are contraindicated) Desmopressin Transiently increases VWF and FVIII levels89 and augments platelet adhesiveness and aggregation68 Agent of choice for treatment or prevention of bleeding in most patients with type 1 VWD; however, patients with type 3 VWD and most patients with type 2 VWD typically require factor concentrates containing FVIII and VWF90 Other desmopressin-responsive bleeding disorders include mild hemophilia A and platelet function disorders, in which the use of desmopressin for surgical coverage has been described21,87; also commonly used for uremic bleeding88 Specifically used for treatment of menorrhagia in women with bleeding disorders25,80,91 Patients, especially children, receiving desmopressin should be closely monitored for hyponatremia22,87 Vitamin K May be used in vitamin K deficiency and for bleeding caused by overmedication with warfarin Widely available and inexpensive Should be given intravenously or orally (not subcutaneously) for best absorption and fastest response92–94 FVIII, factor VIII; PAI, plasminogen activator inhibitor; VWD, von Willebrand disease; VWF, von Willebrand factor.




{kind=link}
{kind=link}