
Abstract
Background: Health literacy screening is often not performed in clinical settings. One possible reason is the concern about the time involved in performing such assessments. Our objective was to measure the time required to administer the Newest Vital Sign (NVS) literacy assessment instrument to English-speaking primary care patients.
Methods: The NVS was administered to 78 consecutive English-speaking patients in an outpatient primary care clinic. The length of time to complete the NVS was timed with a stopwatch.
Results: The average time to complete the NVS was 2.9 minutes (95% confidence limit, 2.6–3.1 min).
Conclusion: The NVS is a health literacy screening tool of sufficient brevity to be considered for use in primary care practices.
Health literacy is the degree to which a person has the ability to obtain, process, and understand health information needed to make appropriate health decisions.1–3 It involves the ability to use and interpret text, documents, and numbers.
People with limited literacy have less knowledge about their health problems,4–10 higher hospitalization rates,11,12 higher health care costs,13–16 and worse health status17–22 than people with adequate literacy. These associations are seen in a variety of studies involving different populations, and they are present even after adjusting for potentially confounding sociodemographic variables. If clinicians have knowledge of the literacy skills of their patients, they can tailor health information so that it is provided in a format that their patients can understand.23
Despite the aforementioned implications of limited health literacy, there is currently no universally accepted method for assessing literacy in clinical settings. Some clinicians use level of education as a surrogate marker of literacy, but education level overestimates actual literacy skills.24 Other clinicians who screen for literacy do so by asking patients how well they read, but this approach is also inaccurate because the majority of patients who have limited literacy report they read “well.” Other clinicians do not screen for literacy for fear of offending patients, citing concerns that people with limited literacy are ashamed of this limitation25–27 and might, therefore, be unwilling to undergo a literacy assessment. Evidence suggests otherwise, however: a recent study involving nearly 600 patients indicates that fully 99% of patients seen in both public and private practice settings readily participated in literacy screening, and there was no decrease in patient satisfaction in practices that undertake such screening.28 Another small study indicated that patients do not object to literacy screening if questions are asked in a sensitive way.29
Finally, the time needed for literacy assessment may also be an obstacle to screening, especially given that the average primary care office visit lasts only 17 minutes.30 The Test of Functional Health Literacy in Adults, a widely used health literacy assessment tool, has good psychometric characteristics and is available in both English and Spanish, but the time required for administration limits it functionality in practice: 18 to 22 minutes for the full version and 7 to 10 minutes for the short version.31,32 The other commonly used tool, the Rapid Estimate of Adult Literacy in Medicine, can be administered in less than 3 minutes, but it is only available in English.33
A new brief instrument for literacy screening in health care settings, The Newest Vital Sign (NVS), is available in both English and Spanish and has recently been validated.34 The validation study for the NVS showed that, when compared with the Test of Functional Health Literacy in Adults, the NVS's area under the receiver–operator characteristics curve for predicting limited health literacy was 0.88 for the English version and 0.71 for the Spanish version; these values are higher than those of many commonly used clinical screening methods such as the CAGE questionnaire to detect alcohol abuse35,36 and breast self-examinations to screen for cancer.37
According to information provided in the validation study, the English version of the NVS can be administered in an average of 3 minutes, but this time estimate was based on a series of only 24 timed administrations. Our objective was to confirm the length of time required to administer the NVS in English by administering it to a larger sample of patients.
Methods
The University of Arizona Human Subjects Protection Program approved the study methods. All participants gave informed consent.
Participants
Participants were consecutive patients being seen by residents and attending physicians in a university-based primary care clinic. The patients’ physicians were not involved in selection or recruitment of study participants. A single researcher (KJ) approached patients, explained the nature of the study, and requested their participation. The researcher approached all patients during the days when she was available in the clinic during the time period of the study.
All participants were 18 years of age or older and read English as their first or primary language. Subjects were excluded if they were younger than 18, if they were unable to meaningfully converse with the researcher in English, or if they were being seen in clinic for an acute emergency that precluded participation in a research project.
Instrument
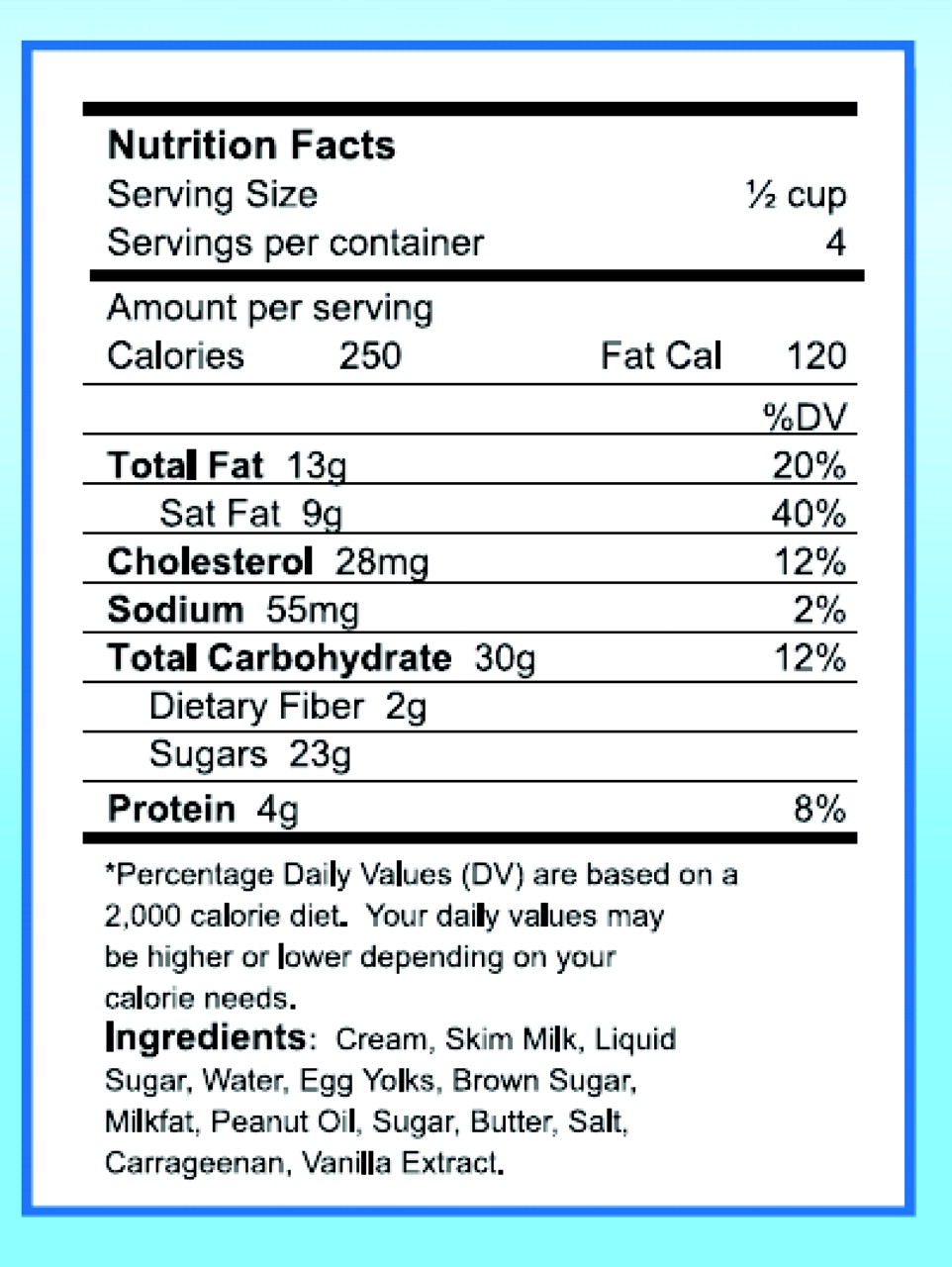
Administering the NVS involves presenting patients with a nutrition label (Fig. 1) and then asking patients 6 questions about the content of the label. The questions ask patients to compute the number of calories in various amounts of food; to interpret the effect on daily fat and carbohydrate consumption if the amount of the food is changed; to identify ingredients in the food; and to determine whether the food can be consumed if an individual is allergic to one of those ingredients.

The nutrition label used in the Newest Vital Sign assessment.
Scores range from 0 to 6, depending on the number of correct responses. Scores of 0 to 1 indicate that low health literacy is likely, scores of 2 to 3 indicate the possibility of low health literacy, and scores of 4 to 6 indicate adequate health literacy.34 In this study, the NVS was administered by a single researcher (KJ), using methods provided with the instrument.38
Measures
During administration of the NVS, the researcher used a stopwatch measure the amount of time it took for participants to complete the NVS assessment. Demographic information about each participant was also collected.
Results
A total of 78 consecutive patients were recruited. All patients asked to participate agreed to do so. Their average age was 44 years (S.D. = 16, range 21 to 81). Other demographic characteristics of the participants are shown in Table 1.
Demographic Characteristics of Patients
Timing of the NVS was reported as mean (SD) and 95% confidence limits.39 The average time to complete the NVS was 2.9 minutes (SD, 1.03 min; 95% CL, 2.67–3.13). The average NVS score was 3.7 (SD, 1.9) out of a maximum score of 6.
Discussion
Timing of the NVS in this larger sample of English-speaking patients is consistent with timing reported in the initial NVS validation study. The NVS takes approximately 3 minutes to complete. The short time required to perform the assessment, combined with the results of a recent study showing that 99% of patients agree to literacy assessment in practice,28 indicate that the NVS is suitable for literacy screening in clinical settings.
The findings of this study are limited, however, by the fact that we included only English-speaking patients and thus cannot comment on the length of time it takes to administer the NVS in Spanish. In the validation study, the average time for a series of 36 Spanish-speaking patients was slightly longer than for English-speaking patients (3.4 vs 2.9 min). It is reasonable to assume that a larger series of Spanish-speaking patients would show a similar time requirement.
A second limitation may be the educational background of our population; 81% had completed a high school or greater level of education. It is possible that the NVS would take longer to administer in a population of patients with a lower education level. However, education level has repeatedly been shown not to correlate well with literacy. Indeed, approximately one quarter of people who score at the lowest level of literacy in national surveys have completed high school.24 This makes the education level of our participants of less concern when applying our results to less-educated populations.
Conclusion
The English version of the NVS can be administered to patients in approximately 3 minutes. Future research should address timing of the Spanish version of the NVS, how best to administer the NVS in primary care practice, and how, or if, physicians change their methods of communication with patients based on NVS results.
Notes
This article was externally peer reviewed.
Funding: none.
Conflict of interest: Dr. Weiss has received research grants from Pfizer, Inc. to develop and test the Newest Vital Sign literacy assessment instrument.
- Received for publication September 21, 2007.
- Revision received January 18, 2008.
- Accepted for publication January 28, 2008.




{kind=link}