
Abstract
Newly developed assays that measure the production of cellular interferon gamma are useful diagnostic tools for the diagnosis of tuberculosis and may potentially replace or complement the tuberculin skin test in some circumstances. Importantly, interferon gamma release assays are more specific than tuberculin skin tests. Unfortunately the tests do not differentiate between active or latent infection. In addition, immunocompromised patients are more likely to have indeterminate results. The current interferon gamma release assays test approved in the United States is costly and requires drawing blood and processing within 12 hours of collection. This study discusses the potential benefits and drawbacks in patients, including those who are immunocompromised.
Tuberculosis is the leading cause of death from a curable infectious disease and a major cause of morbidity in the world.1 Almost 9 million new cases were estimated worldwide in 2004, but only half of them were reported.2
In the United States, a significant decline in new cases of tuberculosis was seen in the 1950s, thanks to an accurate national notification system, sanitation improvements, and the availability of specific antibiotics.3 However, a reemergence of the disease, including multidrug-resistant cases, occurred in the 1980s, correlating with the acquired immune deficiency syndrome epidemic and with an overall deterioration in the public health measures for tuberculosis control. The peak incidence during those years seems to have been curtailed since the early 1990s.4 Nevertheless, the constant migratory flux of people from high-prevalence countries makes tuberculosis a problem that is by no means extinct.
The tuberculin skin test (TST) has been used for more than 100 years for the diagnosis of both active and latent tuberculosis.5 The test is based on the intradermal injection of purified protein derivative (PPD), a crude mixture of mycobacterial antigens, including some from the vaccine strain Mycobacterium bovis Bacillus Calmette-Guerin (BCG) and from nontuberculous mycobacteria.6 TST is inexpensive and does not require additional infrastructure to be performed, hence its popularity. However, TST has many drawbacks including a high rate of false-positive results (because it includes mycobacterial antigens that are not specific for M. tuberculosis), a high rate of false-negative results among immunosuppressed patients, a need for patient compliance to return for the test to be read, and subjectivity and interpersonal variability among health care workers when interpreting the results.7 TST also has the potential disadvantage of boosting an anamnestic response with successive tests.8
New tests that measure the production of interferon gamma (IFN-γ) by T-cells after sensitization with M. tuberculosis antigens are available and, at least theoretically, may overcome some of the limitations of the TST.9 The 2 commercially available tests are the T SPOT-TB assay, an enzyme-linked immunosorbent spot or ELISPOT test that uses peripheral blood mononuclear cells, and the QuantiFERON-TB Gold, an enzyme-linked immunosorbent assay (ELISA) that uses whole blood.10,11 The QuantiFERON-TB Gold involves the use of more specific antigens and has replaced the first generation QuantiFERON-TB. QuantiFERON-TB Gold is the only test of its class licensed by the Food and Drug Administration for use in the United States, and consequently will be the focus of this review.8 An excellent review of other IFN-γ assays used for the diagnosis of tuberculosis has been published elsewhere.12 Key differences between the ELISA T-cell–based IFN-γ release assay (ELISA interferon gamma release assays [IGRA]) and the TST are outlined in Table 1.
Comparison of QuantiFERON-TB Gold and Tuberculin Skin Testing
ELISA T-Cell–based INF-γ Release Assay
The test is based on the principle that T-cells from a whole blood sample, when exposed and incubated with a specific M. tuberculosis antigen, will produce IFN-γ.13 The ELISA-IGRA uses the culture filtrate protein 10 (CFP-10) and the early secretory antigenic target 6 (ESAT-6) as stimulating antigens.12 CFP-10 and ESAT-6 are encoded within the region of difference 1 of the M. tuberculosis genome, and they are more specific for M. tuberculosis than PPD because they are not shared with BCG strains or common nontuberculous mycobacteria.14 Therefore, the advantage of this test is the potential ability to discriminate between tuberculosis infection and previous use of BCG vaccine or atypical mycobacteria reactivity.15
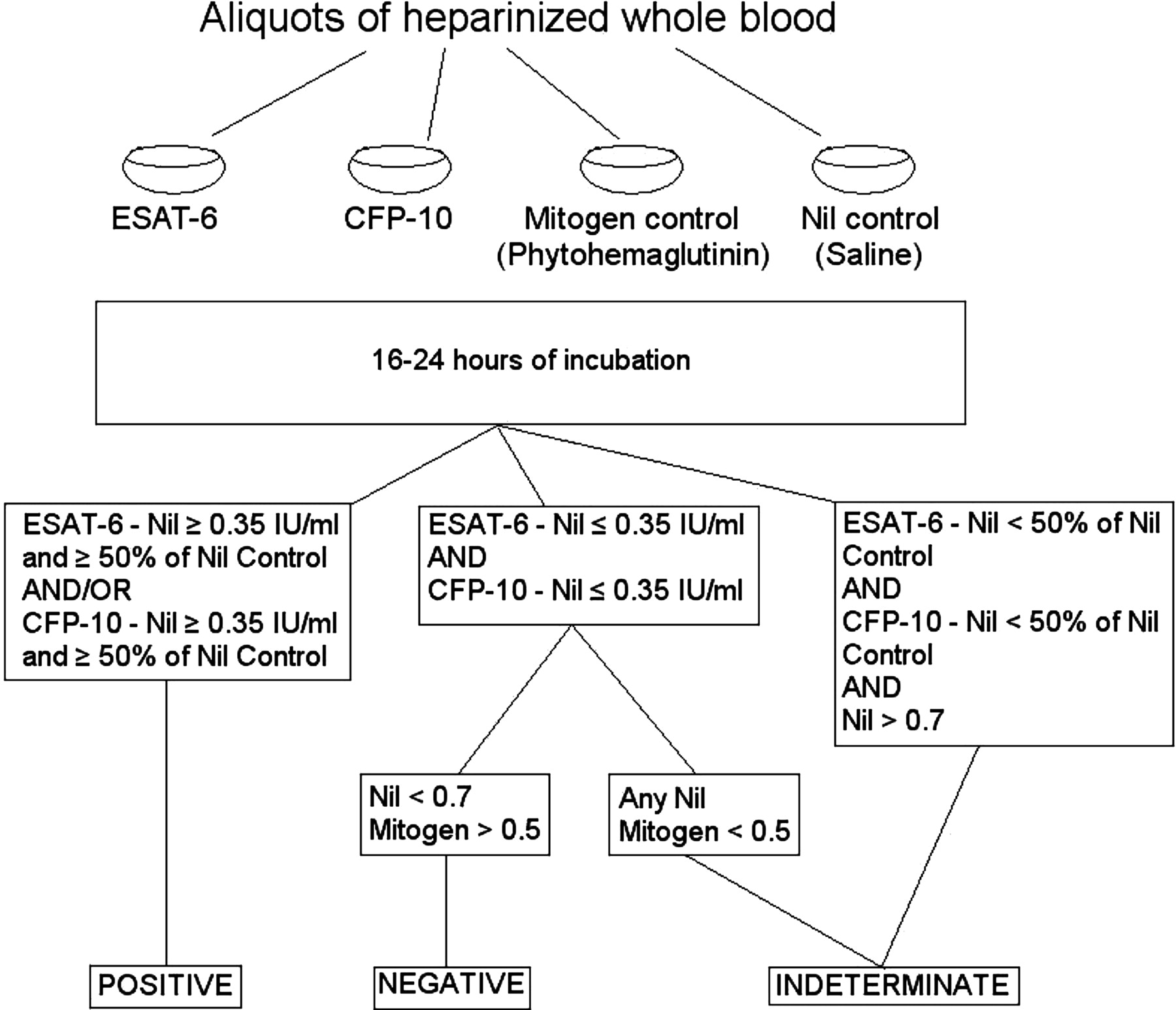
The test is performed by obtaining whole heparinazed blood and incubating it with peptide cocktails simulating ESAT-6 and CFP-10 proteins. Other antigens, such as phytohemaglutinin and saline, are used as controls. The former is a mitogen that, after stimulating plasma, serves as an IFN-γ positive control for each specimen; the latter is a control that adjusts for heterophile antibodies in serum or plasma, which are known to cause interference with immunoassays.8,16 After 16 to 24 hours, the production of IFN-γ is measured by ELISA. The test is reported as positive, negative, or indeterminate (Figure 1). Indeterminate results can be caused by reduced lymphocyte count in the blood sample or reduced lymphocyte activity because of an intercurrent illness (such as human immunodeficiency virus [HIV] infection, malignancy, or renal dysfunction); prolonged specimen transport or improper specimen handling; and incorrect addition of the mitogen.16,17 A significant drawback of the test is that the sample needs to be processed within 12 hours of collection; otherwise, the white cells will lose viability.16 A variant of the ELISA-IGRA called “QuantiFERON-TB Gold in tube” uses blood-collection tubes (which are precoated with control and test antigens) as incubation vessels, thus minimizing blood handling and simplifying the blood stimulation step. This device is only approved in Europe, Asia, and Australia.16,18

Procedure and result interpretation of ELISA T-cell–based gamma release essay. ESAT-6 and CFP-10 refer to specific antigens coded by the esat-6 and lhp genes of Mycobacterium tuberculosis. For indeterminate results, the test may be repeated if there is evidence of potential technical errors, such as storage at incorrect temperature, pipetting errors, etc.
When Is the IFN-γ Assay Indicated?
The test is licensed by the Food and Drug Administration as an aid in the diagnosis of both active tuberculosis and latent infection.8 The test can be used on all occasions when a TST is used, including contact investigations, evaluation of immigrants who have received BCG vaccination, and TB screening of health workers.18–21 Consequently, the test should prompt the same response as a positive TST: basically exclusion of active tuberculosis and/or consideration of treatment of latent tuberculosis.8
The ELISA-IGRA cannot differentiate between latent or active tuberculosis. That differentiation needs to be done in the context of a thorough clinical and radiologic evaluation to determine which of the 2 conditions is present. In addition, indeterminate and false-negative test results may occur in immunosuppressed patients.17,22 A study of 318 patients showed that the majority of the 21.4% with indeterminate results were very young or very old (younger than 3 or older than 80 years old); were receiving immunosuppressive therapy (cancer chemotherapy, systemic steroids, or antitumor necrosis factor α agents); or were patients with cancer, HIV infection, or renal failure.17
Although the proteins used in the assay are specific for M. tuberculosis, they are also seen in some nontuberculous mycobacteria, including M. kansasii, M. szulgai, and M. marinum. False-positive results in the setting of these infections is likely.8 For example, in a small study that included 7 patients infected with M. marinum, 5 patients infected with M. kansasii, and 7 long-term owners of tropical fish tanks (likely exposed to M. marinum), more than 50% of them had a detectable IFN-γ response to either ESAT-6 or CFP-10 as measured by either ELISA or ELISPOT.23 It also seems that L-ESAT, a M. leprae antigen homolog to the T-ESAT-6 seen in M. tuberculosis, has significant cross-reactivity and may induce the production of IFN-γ, therefore making the test less useful in populations in which leprosy is endemic.24 Leprosy is considered endemic, but with low prevalence, in Louisiana and Texas, particularly among South East Asian immigrants.25 The ESAT gene cluster is also present in M. avium; however, evidence of false-positive ELISA-IGRA tests with this infection is lacking.26
How Does the Test Behave in the General Population?
Both the ELISA-IGRA and TST tests are useful in the identification of tuberculous infection, but they measure different responses: the former detects the in vitro release of IFN-γ, the later measures an in vivo-type intradermal response.6,11 Both tests have a good level of agreement, at least among patients at risk in industrialized countries. The largest prospective comparison study to date, done using the QuantiFERON-TB test, included 1226 patients and showed 83.1% concordance between the 2 tests (κ = 0.60).27 It seems that the ELISA-IGRA results and the size of induration of the TST are directly correlated. People with a TST of <5 mm are more likely to have indeterminate ELISA-IGRA results when compared with patients with a larger induration.17 In addition, the concordance of both tests is lower among BCG-vaccinated people as compared with unvaccinated individuals (κ = 0.09 vs κ = 0.56, respectively).17 In countries with a higher prevalence of nontubercular mycobacterial infections, the correlation between the tests may decline; for example, a report from Korea described a poor correlation between the test in healthy volunteers with and without risk factors for tuberculosis exposure (κ = 0.08–0.17), even when correcting the cutoff value for TST to >15 mm.20
ELISA-IGRA seems to be highly specific for active tuberculosis, as defined by the number of patients without tuberculosis who have negative ELISA-IGRA. In 4 studies that addressed this issue, the specificity ranged between 97% and 100%.6,15,28,29 Although it has been suggested that IGRA detects IFN-γ released from T-cells that have recently encountered antigens in vivo rather than from persistent memory T-cells, the use of this test for follow-up purposes and to document the cure of tuberculosis remains controversial.30,31
In areas where tuberculosis is endemic, it has been suggested that ELISA-IGRA offers increased specificity in the diagnosis of M. tuberculosis infection at the cost of some sensitivity.32 In fact, in head-to-head comparisons between the TST and IFN-γ assays, the highest sensitivity corresponded to the TST, followed by IFN-γ assays based on PPD, and lastly IFN-γ assays based on specific region of difference 1 antigens (such as ELISA-IGRA).12 The sensitivity of ELISA-IGRA in people with active tuberculosis, based on 4 case-control studies and 1 cross-sectional study, varies between 72% and 89%.6,15,28,29
The first study that directly compared ELISA-IGRA with conventional microbiologic methods for the diagnosis of active tuberculosis was published in 2005.29 Previous studies calculated sensitivity and specificity in patients with microbiologically proven active tuberculosis, but this study enrolled patients prospectively and analyzed data without knowing the final diagnoses. The sensitivity for ELISA-IGRA was 85%, compared with only 42% for microscopy and 59% for culture. ELISA-IGRA was of particular use in patients with active extrapulmonary tuberculosis who were microscopy-negative and culture-negative. On the other hand, among healthy controls without exposure to tuberculosis, ELISA-IGRA had a specificity of 97% (so the majority of uninfected patients did have a negative ELISA-IGRA). The specificity dropped to 60% when patients who were being ruled out for tuberculosis were tested because a high number of them had latent tuberculosis. In conclusion, in a clinical setting, the ELISA-IGRA will be highly sensitive but unable to differentiate between latent and active disease.
Because of the absence of a criterion standard for the diagnosis of latent tuberculosis, it is difficult to determine whether the ELISA-IGRA performs better than the TST.27 Studies of sensitivity in latent tuberculosis are mainly based on previous information obtained for the old QuantiFERON-TB. In fact, one of the first reports that assessed the liberation of IFN-γ after exposure to tuberculin was performed in Australia and showed a specificity of 98% and a sensitivity of 90%.33 An outbreak of tuberculosis in a secondary school with low prevalence of latent tuberculosis in Leicestershire, United Kingdom, gave investigators the opportunity to compare the sensitivity of the IFN-γ–based test with TST.34 Although the IFN-γ test used was an ELISPOT, the antigens used were the same as those used in the QuantiFERON-TB Gold assay. The agreement between TST and ELISPOT was high (κ = 0.72; 95% CI, 0.64–0.80; P < .0001); however, for students with discordant results, ELISPOT was a stronger predictor of M. tuberculosis exposure compared with an isolated positive TST. The conclusion was that ELISPOT was more accurate than TST for the detection of latent tuberculosis, and presumably more sensitive. The performance characteristics of the ELISA-IGRA are listed in Table 2.
Sensitivity and Specificity of QuantiFERON-TB Gold and Agreement Between QuantiFERON-TB Gold and Tuberculin Skin Testing
ELISA-IGRA in Patients with Immune Dysfunction
HIV Co-Infection
The importance of the relationship between AIDS and tuberculosis cannot be overemphasized. In immunocompetent patients with latent tuberculosis, the lifetime risk of developing active disease is approximately 10%. However, in people with HIV infection it becomes 10% per year.35 In addition, active tuberculosis is more difficult to treat in HIV-infected patients because of complex drug–drug interactions between antiretroviral and antituberculous medications, increased pill burden, and increased risk of toxicity.36 Unfortunately, people with HIV infection may be prone to indeterminate IFN-γ test results as a consequence of the inability to mount a satisfactory T-cell response.26,37 In addition, in patients with AIDS treated with antiretroviral therapy, the functional capacity of the CD4+ cells to produce IFN-γ may remain impaired even after immune recovery and increase in the absolute and relative CD4+ cell count.38 Studies of the role of IGRA in patients with HIV/tuberculosis co-infection are lacking.
A study using ELISPOT in Zambia showed that the test had high sensitivity in HIV-infected patients; however, 4 patients with active tuberculosis did not have any response. There was no significant difference in the mean lymphocyte count of these patients compared with responders, but no comparison of CD4+ cell counts was performed.39 In this study, the sensitivity for active tuberculosis dropped from 100% in healthy people to 90% in HIV-infected patients, and the sensitivity for latent tuberculosis among HIV-infected patients was poor, falling from 80% in healthy people to 36% among HIV-infected patients.
Other Immunosuppressive Conditions
Very limited information is available for other immunosuppressed populations. Conditions such as hematologic and solid organ malignancies, diabetes mellitus, chronic renal failure, and the use of corticosteroids, antineoplastic drugs, immunosuppressants (for chemotherapy and organ transplantation), and tumor necrosis α antagonists may affect the response to TST and also may affect the result of ELISA-IGRA because of decreasing production of IFN-γ.8 For example, when evaluating the routine use of ELISA-IGRA among unselected patients in an Italian hospital, those who were receiving immunosuppressive therapies had higher odds ratio (odds ratio, 3.35; 95% confidence interval, 1.84–6.08) of having indeterminate results compared with patients who were not receiving such therapy.17 Although it may be disappointing that ELISA-IGRA is associated with indeterminate results, the lack of mitogen response may warn about the possibility of an underlying immunosuppressant (a piece of information that cannot be obtained with a TST) and may alert the clinician of the need to search more extensively for tuberculosis infection among patients at risk.37
The performance of the IGRA has not been evaluated in patients with impaired immune function.
In summary, ELISA-IGRA should be used with caution among HIV-infected and other immunosuppressed patients. A positive or negative result is helpful, but an indeterminate result does not rule out tuberculosis infection. An indeterminate result in the absence of a mitogen response may suggest anergy rather than absence of infection.
Potential Drawbacks
Although ELISA-IGRA has several advantages when compared with TST, it may be several times more expensive.20 In a study in San Francisco, the cost of an ELISA-IGRA was calculated at approximately $37.39 per patient.39 Most of the cost was incurred by the laboratory, but additional costs such as phlebotomy, specimen transport, and processing were included. This is in comparison with $9.79 for a TST as estimated by the Center for Medicare Services.40 However, the price listed for TST does not take into consideration the cost of a second visit to read the results and the transportation and work-force related costs for the patient.
One of the main values of the ELISA-IGRA is its high negative predictive value. A negative test in a healthy patient excludes tuberculosis infection. However, as with other diagnostic tests, the positive predictive value depends on the prevalence of M. tuberculosis in the population that is being tested.8,29
ELISA-IGRA does not differentiate between active or latent tuberculosis. This determination should be based on the presence of symptoms (chronic cough, fever, hemoptysis) and the findings on a chest radiograph.
The threshold for deciding when a TST is positive depends on the risk factors of the patient population. For example HIV-infected patients have a positive TST at 5 mm, health care workers at 10 mm, and the general public at 15 mm. Current guidelines for interpretation of the results for the ELISA-IGRA are the same for all patient populations. The results are reported as positive, negative, or indeterminate. An indeterminate result is unhelpful in the diagnosis of tuberculosis infection (although, as mentioned before, the absence of mitogen response may suggest anergy).
Unanswered Questions and Further Directions
The advantage of ELISA-IGRA is that by improving specificity it will reduce the number of false-positive results among BCG-vaccinated people or those exposed to nontuberculous mycobacteria, thus avoiding additional costs and potential toxicity of drugs used for the treatment of latent tuberculosis. In addition, it may increase the identification of more cases of latent tuberculosis before progression to active disease. These advantages need to be balanced with increased laboratory costs, which are a result of dedicated equipment and personnel training requirements.41 Performing the test in diagnostic laboratories in developed countries is feasible, as documented by experience in the United States and Europe,9,17,40 but also in some resource-poor settings such as South Africa and India.42,43 In San Francisco, among 4143 patients, usable results (either positive or negative) were available from 92%, compared with only around 47% to 60% (at most 84% in selected locations) of patients returning for the reading of a TST.40 Additional studies in economic evaluation and decision analyses are required in this area.
It has been hypothesized that after active tuberculosis treatment the levels of IFN-γ production will decrease. However, several reports using ELISPOT have been contradictory, with some suggesting a decrease in the ESAT-6 response and others showing persistent elevation or even increased response.31,44 Measurement changes of ELISA-IGRA after treatment of both latent and active tuberculosis, and the ability of the test to detect reinfection, are areas of research that have been encouraged by the Centers for Disease Control and Prevention.8 Finally, large prospective longitudinal studies are needed to clearly identify factors that influence test performance, particularly among immunosuppressed patients and children.
Conclusions
“Take home” points are outlined in Table 3. In summary, the ELISA-IGRA is a new assay based on in vitro detection of IFN-γ that may replace PPD as a diagnostic tool for latent and active tuberculosis. The test is more specific and does not require patients to return for a second visit (as TST demands). Cost, technical limitations, and limited data in the most vulnerable groups, such as children and immunosuppressed patients, may prevent the immediate replacement of the TST. In addition, the test can only aid in the diagnosis of active tuberculosis, which must still be made by clinical and microbiologic evaluations.
Take-Home Points
Acknowledgments
We are indebted to Ms. Deanna Hansen for her invaluable help in preparing the manuscript.
Notes
This article was externally peer reviewed.
Funding: This manuscript was supported by Diversity Supplement Funding awarded to Dr. Madariaga by the University of Nebraska Medical Center.
Conflict of interest: Dr. Madariaga reports receiving research grants or contracts or was a consultant for Pfizer and Bavarian Nordic. Dr. Jalali reports receiving research grants or contracts or was a consultant for GlaxoSmithKline. Dr. Swindells reports receiving research grants or contracts from or was a consultant for Abbott Pharmaceuticals, Bristol-Myers Squibb, Novartis Pharmaceuticals Corporation, Tibotec Therapeutics, and Pfizer. None of the entities mentioned above sponsored or had any role or influence in the preparation of this manuscript.
- Received for publication April 25, 2007.
- Revision received August 15, 2007.
- Accepted for publication August 20, 2007.




{kind=link}