
Article Figures & Data
Figures
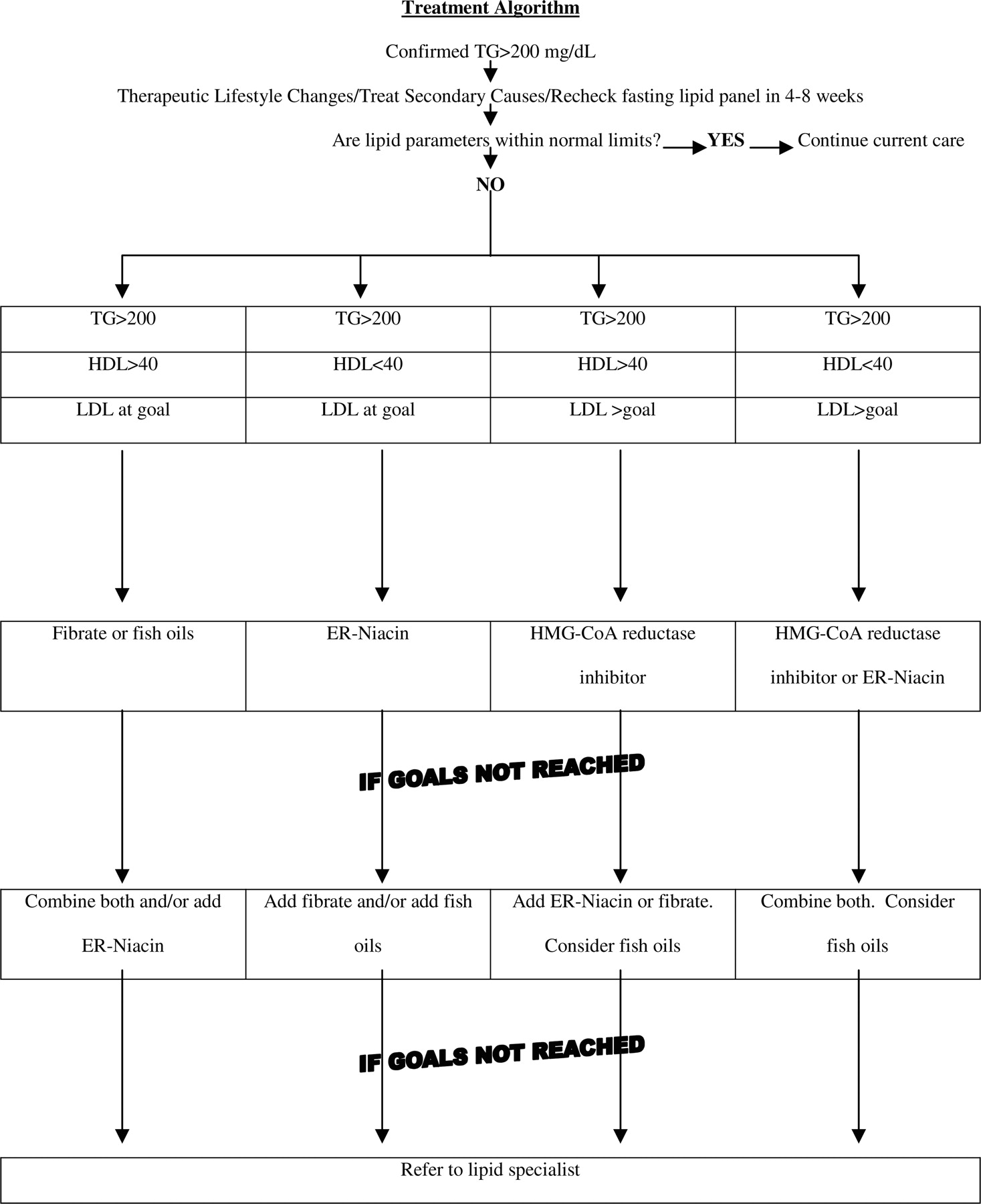
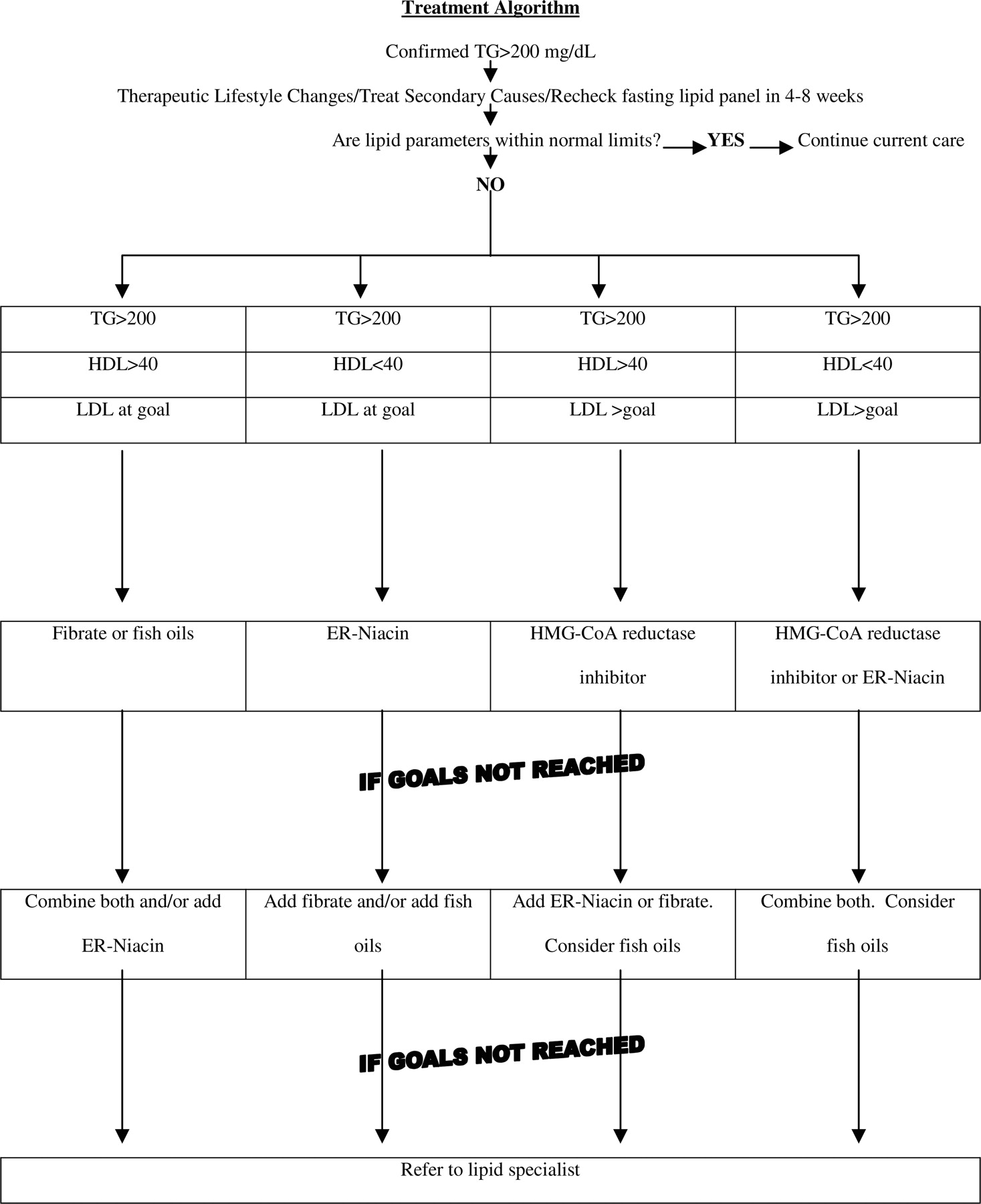
- Figure 1.
Treatment Algorithm.
Tables
Classification Triglyceride Level (mg/dL) Normal <150 Borderline high 150 to 199 High 200 to 499 Very high >500 Type Elevated Lipoprotein Total Cholesterol Level Triglyceride Level Relative Frequency I CM* Normal ++ <1% IIa LDL ++ Normal 10% (FHC) IIb LDL/VLDL ++ + 40% (FCH) III IDL + + <1% IV VLDL Normal to+ ++ 45% (FHT) V CM + ++ 5% VLDL * CM, chylomicron; LDL, low-density lipoprotein; VLDL, very low-density lipoprotein; IDL, intermediate density lipoprotein; FHC, familial hypercholesterolemia; FCH, familial combined hyperlipidemia; FHT, familial hypertriglyceridemia.
+ Mild to moderate increase.
++ Moderate to severe increase.
Atypical anti-psychotics Beta blockers Bile acid binding resins Estrogen (in higher dose oral contraceptives and unopposed oral estrogen) Glucocorticoids Immunosuppressants Isotretinoin Protease inhibitors Tamoxifen Thiazides Key Clinical Recommendations Strength of Recommendation References Obtain fasting lipid panel on patients beginning at 20 years old C 1 Search for other components of metabolic syndrome in patients with high triglycerides C 3 Decrease triglycerides to <500 mg/dL to prevent pancreatitis B 1,4,5 Decrease triglycerides and increase HDL to prevent cardiovascular events B 9,10 Risk Group Begin Screening Frequency Test CHD* 20 1 to 2 years Fasting lipid panel CHD risk equivalent or 2 or more risk factors† Familial dyslipidemia or family history of premature CHD 20 Every 2 years Fasting lipid panel No risk 20 Every 5 years Fasting lipid panel or non-fasting total cholesterol/HDL * CHD, coronary heart disease; HDL, high-density lipoprotein.
† Risk factors: cigarette smoking, hypertension or taking blood pressure medication, HDL <40, first degree relative with coronary artery disease (men <55, women <65), age (men >45, women >55).
Serum urea nitrogen Creatinine Fasting glucose Fasting insulin level (if metabolic syndrome is suspected) Liver function Thyrotropin Urinalysis Initiate therapeutic lifestyle changes (weight loss/exercise) first
Reduce triglyceride level to less than 500 mg/dL to prevent pancreatitis
Primary aim of medical therapy is to reach LDL* goal
Secondary aim of therapy is to reach non-HDL goal
In patients with CHD or CHD risk equivalents, tertiary aim of therapy is to reach HDL goal.
* LDL, low-density lipoprotein; HDL, high-density lipoprotein; CHD, coronary heart.




{kind=link}