
Abstract
Hypertriglyceridemia is a commonly encountered lipid abnormality frequently associated with other lipid and metabolic derangements. The National Cholesterol Education Program recommends obtaining a fasting lipid panel in adults over the age of 20. The discovery of hypertriglyceridemia should prompt an investigation for secondary causes such as high fat diet, excessive alcohol intake, certain medications, and medical conditions (eg, diabetes mellitus, hypothyroidism). In addition, patients should be evaluated for other components of the metabolic syndrome. These include abdominal obesity, insulin resistance, low high-density lipoprotein (HDL), high triglyceride, and hypertension. Hypertriglyceridemia is classified as primary hypertriglyceridemia when there are no secondary causes identified. Primary hypertriglyceridemia is the result of various genetic defects leading to disordered triglyceride metabolism. It is important to treat hypertriglyceridemia to prevent pancreatitis by reducing triglyceride levels to <500 mg/dL. Furthermore, lowering triglycerides while treating other dyslipidemias and components of the metabolic syndrome will reduce coronary events. However, it is controversial how much isolated hypertriglyceridemia correlates directly with coronary artery disease and further studies are needed to clarify whether treatment for this condition leads to meaningful clinical outcomes. Therapeutic lifestyle changes (TLC) are the first line of treatment for hypertriglyceridemia. These changes include a low saturated fat, carbohydrate-controlled diet, combined with alcohol reduction, smoking cessation, and regular aerobic exercise. High doses of omega-3 fatty acids from fish and fish oil supplements will lower triglyceride levels significantly. When patients do not reach their goals by TLC, drug therapy should be started. In cases of isolated hypertriglyceridemia, fibrates are initially considered. When elevated low-density lipoprotein levels accompany hypertriglyceridemia, 3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitors are preferred. In patients with low HDL levels and hypertriglyceridemia, extended release niacin can be considered. A combination of the medicines may be necessary in recalcitrant cases.
Hypertriglyceridemia is defined as an abnormal concentration of triglyceride in the blood. According to the National Cholesterol Education Program Adult Treatment Panel (NCEP ATP III) guidelines, a normal triglyceride level is <150 mg/dL (Table 1).1 In the United States, the prevalence of hypertriglyceridemia defined as a triglyceride level >150 mg/dL is ∼30%.2,3 Hypertriglyceridemia may be primary or secondary in nature. Primary hypertriglyceridemia is the result of various genetic defects leading to disordered triglyceride metabolism. Secondary causes are acquired causes, such as, high fat diet, obesity, diabetes, hypothyroidism, and certain medications.
Classification of Triglyceride Levels
Hypertriglyceridemia is a risk factor for pancreatitis and it accounts for 1 to 4% of cases of acute pancreatitis. Although a few patients can develop pancreatitis with triglyceride levels >500 mg/dL, the risk for pancreatitis does not become clinically significant until levels are >1000 mg/dL.1,4,5 More importantly however, hypertriglyceridemia is typically not an isolated abnormality. It is frequently associated with other lipid abnormalities and the metabolic syndrome (abdominal obesity, insulin resistance, low high-density lipoprotein (HDL), high triglyceride, and hypertension), which are linked to coronary artery disease.3
Considering the current obesity epidemic, there will be a significant rise in the incidence of the metabolic syndrome. Thus, primary care physicians will encounter hypertriglyceridemia more frequently and should be familiar with the evaluation and management of this common disorder.
Pathophysiology
Dietary triglycerides are absorbed by the small intestine, secreted into the lymph system, and enter the systemic circulation as chylomicrons via the thoracic duct. Muscle and adipose tissue remove some of the triglyceride from the chylomicron and the chylomicron remnant is taken up by the liver and metabolized into a cholesterol rich lipoprotein. Although most of the triglyceride found in blood is absorbed from the small intestine, the liver produces and secretes a small amount of triglyceride. Apolipoproteins are proteins associated with lipids that assist with their assembly, transport, and metabolism. Defects in any of these structural proteins or the enzymes they interact with may result in a clinical dyslipidemia.
The Fredrickson classification scheme organizes these various primary dyslipidemias into a several categories (Table 2).6 High triglycerides are a component of each of these dyslipidemias except Fredrickson type IIa (familial hypercholesterolemia). In the United States, the 2 most common dyslipidemias are Fredrickson type IIb (familial combined hyperlipidemia) and type IV (familial hypertriglyceridemia). Together, these 2 dyslipidemias account for 85% of familial dyslipidemias.
Fredrickson Dyslipidemia Classification
In contrast to primary hypertriglyceridemia, there are many secondary causes of hypertriglyceridemia. These include medical conditions such as diabetes mellitus, hypothyroidism, obesity, and nephrotic syndrome. In addition, certain medications (Table 3), high carbohydrate diets, and alcohol can cause or exacerbate hypertriglyceridemia. Commonly, hypertriglyceridemia results from a combination of factors. For example, a patient may be found to have familial combined dyslipidemia, obesity, and high alcohol consumption.
Medications That Elevate Triglycerides
Clinical Presentation
The majority of the time, hypertriglyceridemia is discovered after performing a routine lipid profile. However, severe hypertriglyceridemia (>500 mg/dL) may cause pancreatitis, eruptive xanthomas, or lipemia retinalis. In some cases, extremely high levels of chylomicrons can cause chylomiconemia syndrome, which is characterized by recurrent abdominal pain, nausea, vomiting, and pancreatitis. Triglycerides are typically >2000 mg/dL in this condition. Eruptive xanthomas are 1- to 3-mm yellow papules that can erupt anywhere but are usually seen on the back, chest, and proximal extremities. Palmar xanthomas, yellow creases on the palm, may be seen in patients with type III hyperlipidemia. Lipemia retinalis is the visualization of lipemic blood in the retinal blood vessels.
Diagnostic Evaluation
The NCEP recommends obtaining a fasting lipid panel [total cholesterol, low-density lipoprotein (LDL), HDL, and triglycerides] on patients beginning at age 20 and repeated; every 5 years [strength of recommendation (SOR)-C] (Tables 4 and 5).1 In healthy asymptomatic patients without risk factors, it is acceptable to obtain a nonfasting total cholesterol and HDL cholesterol level every 5 years. However, for patients with coronary heart disease (CHD), CHD risk equivalents, familial dyslipidemia, or risk factors for CHD, a fasting lipid panel should be obtained yearly. If the triglyceride level is discovered to be >150 mg/dL, it should be rechecked again after a 12- to 16-hour fast for confirmation. If the triglyceride level is >1000 mg/dL, beta-quantification by ultra centrifugation and electrophoresis can be performed to determine the exact dyslipidemia.
Strength of Recommendations (SORT)
ATP III Adult Lipid Screening Recommendations
The 2 most common dyslipidemias are familial combined hyperlipidemia (type IIb) and familial hypertriglyceridemia (type IV). In type IIb, the total cholesterol, low-density lipoprotein (LDL) cholesterol, and triglyceride levels are all elevated. In type IV, the total cholesterol and LDL levels are typically normal but the triglyceride level is elevated usually between 500 and 1000 mg/dL. Patients with type IV disease are very sensitive to dietary modifications.
The finding of hypertriglyceridemia should prompt an investigation for other components of the metabolic syndrome [SOR-C].3 In particular, patients should be evaluated for fasting hyperglycemia, hypertension, abdominal obesity, and low HDL levels. Thyrotropin level, serum urea nitrogen, creatinine, and urinalysis should be obtained to assess thyroid and renal function (Table 6). Baseline liver function should also be assessed before starting medication. If there is a clinical suspicion of pancreatitis, amylase and lipase levels should be measured. A fasting insulin level can be measured to look for direct evidence of insulin resistance. A fasting insulin level above 15 μU/mL is abnormal. However, a fasting glucose to fasting insulin ratio provides a more sensitive and specific assessment of insulin resistance.7 A normal glucose-insulin ratio is >4.5. Ratios <4.5 suggest insulin resistance.
Basic Laboratory Evaluation for Confirmed Hypertriglyceridemia
Treatment
A major reason to treat hypertriglyceridemia is to prevent pancreatitis. The triglyceride level should be reduced to <500 mg/dL to prevent this serious disease [SOR-B].1,4,5 The relationship between triglycerides and cardiovascular disease is less clear. There have been multiple conflicting studies regarding the role of triglycerides and the development of CHD.8–12 Hypertriglyceridemia is clearly associated with CHD in univariate analysis. However, many multivariate studies have shown that its risk is markedly attenuated after adjustment for other strong CHD risk factors, namely, low HDL levels and increased small, dense LDL particles. These findings have led some researchers to believe that hypertriglyceridemia serves more as a proxy for abnormal cholesterol levels and cholesterol sub-fractions of which hypertriglyceridemia is frequently associated.13 Most interventions aimed at lowering the triglyceride level also raise the HDL level, which is well known for reducing coronary events [SOR-B].9,10 A recent review of the literature concluded that treating isolated hypertriglyceridemia does not prevent coronary events.14 However, a thorough search for other components of the metabolic syndrome is recommended.
On the other hand, there have been many other studies that have shown hypertriglyceridemia to be an independent risk factor for CHD even after adjustment for HDL and LDL.915–17 Furthermore, the NCEP considers hypertriglyceridemia to be an independent risk factor for CHD and calls for medical treatment in cases where therapeutic lifestyle changes (TLC) are not adequate to reduce the triglycerides to appropriate levels.1 Although the extent to which hypertriglyceridemia causes CHD is controversial at present, the authors feel that because most cases of hypertriglyceridemia are associated with abnormal cholesterol sub-fractions and are frequently found in patients with CHD risk factors, treatment of hypertriglyceridemia is often warranted in conjunction with the necessary treatment of the other lipid derangements. In cases where hypertriglyceridemia is found to be the only lipid abnormality, treatment is still important to prevent pancreatitis when triglycerides are markedly elevated.
The treatment of hypertriglyceridemia begins with TLC. Specifically, a low fat, carbohydrate-controlled diet should be adopted. Saturated fat should not make up more than 7% of total daily calories, carbohydrates should be restricted to 50% to 60% of daily calories, and simple sugars like sucrose should be avoided.1 Patients may also consider increasing intake of oily fish (eg, salmon, mackerel, herring) to at least 2 servings per week.18 Alcohol should be greatly reduced or stopped altogether, along with smoking cessation if indicated. Discontinuation of any offending medications should be considered as well. Titration upwards to a goal of at least 30 minutes of aerobic exercise 5 days a week is greatly beneficial. If present, diabetes and hypothyroidism should be treated accordingly. These measures often have a dramatic effect on triglyceride levels and can lower it hundreds of points.1
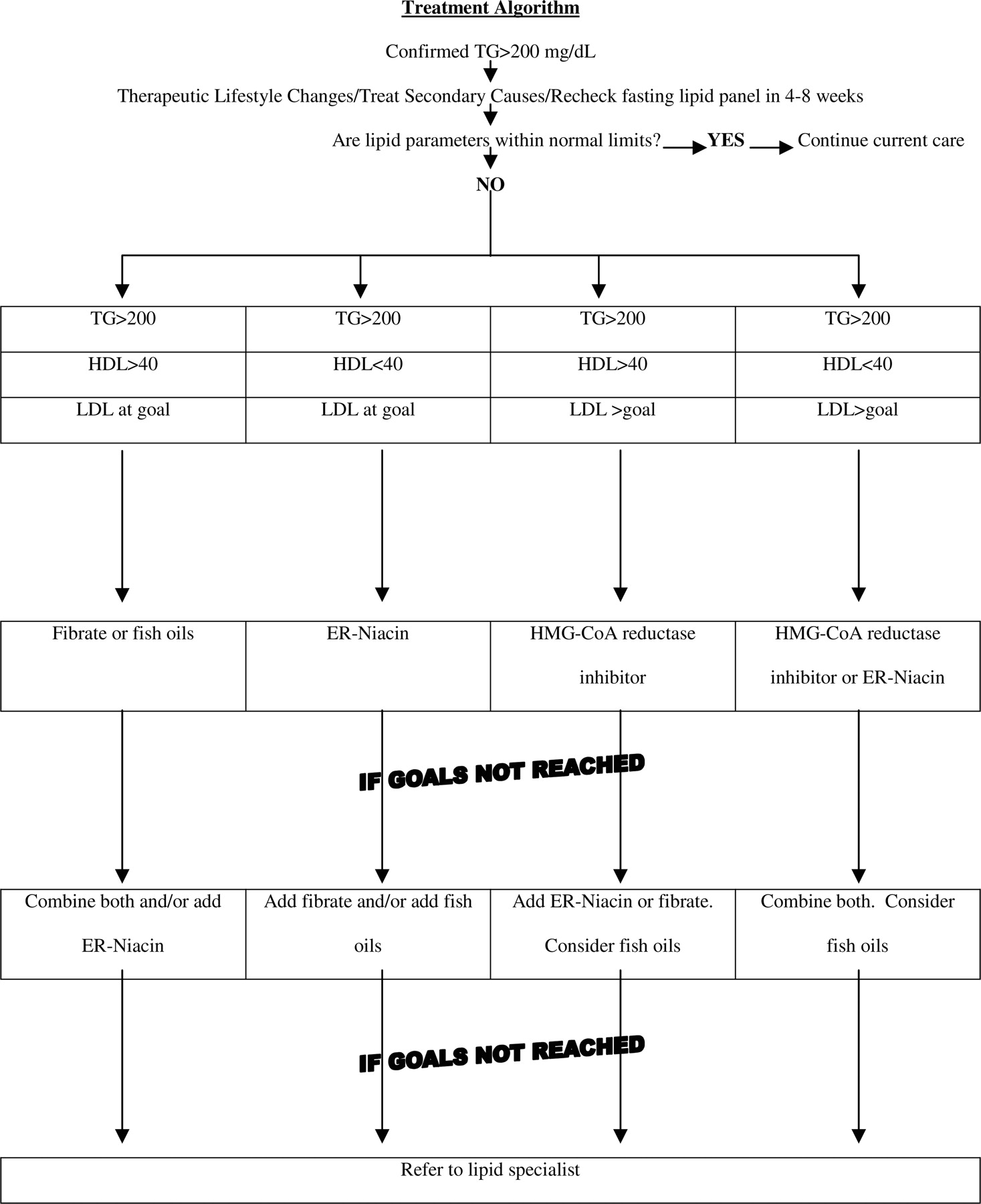
If TLC and control of secondary medical conditions are not adequate to lower the triglyceride level to <200 mg/dL, then medical therapy is warranted (Figure 1). When triglyceride levels range between 200 mg/dL and 500 mg/dL, treatment should be directed primarily toward normalizing the LDL cholesterol.1 Once the LDL is at goal, a secondary endpoint is the non-HDL cholesterol (total cholesterol-HDL). Non-HDL goals are 30 mg/dL higher than LDL goals. A tertiary treatment goal, particularly in the setting of CHD or CHD risk equivalents, is to raise the HDL to >40 mg/dL. The benefit of medically treating triglyceride levels between 200 mg/dL and 500 mg/dL when the other lipid sub-fractions are normal is less clear and medical management in these patients should be individualized (Table 7).14
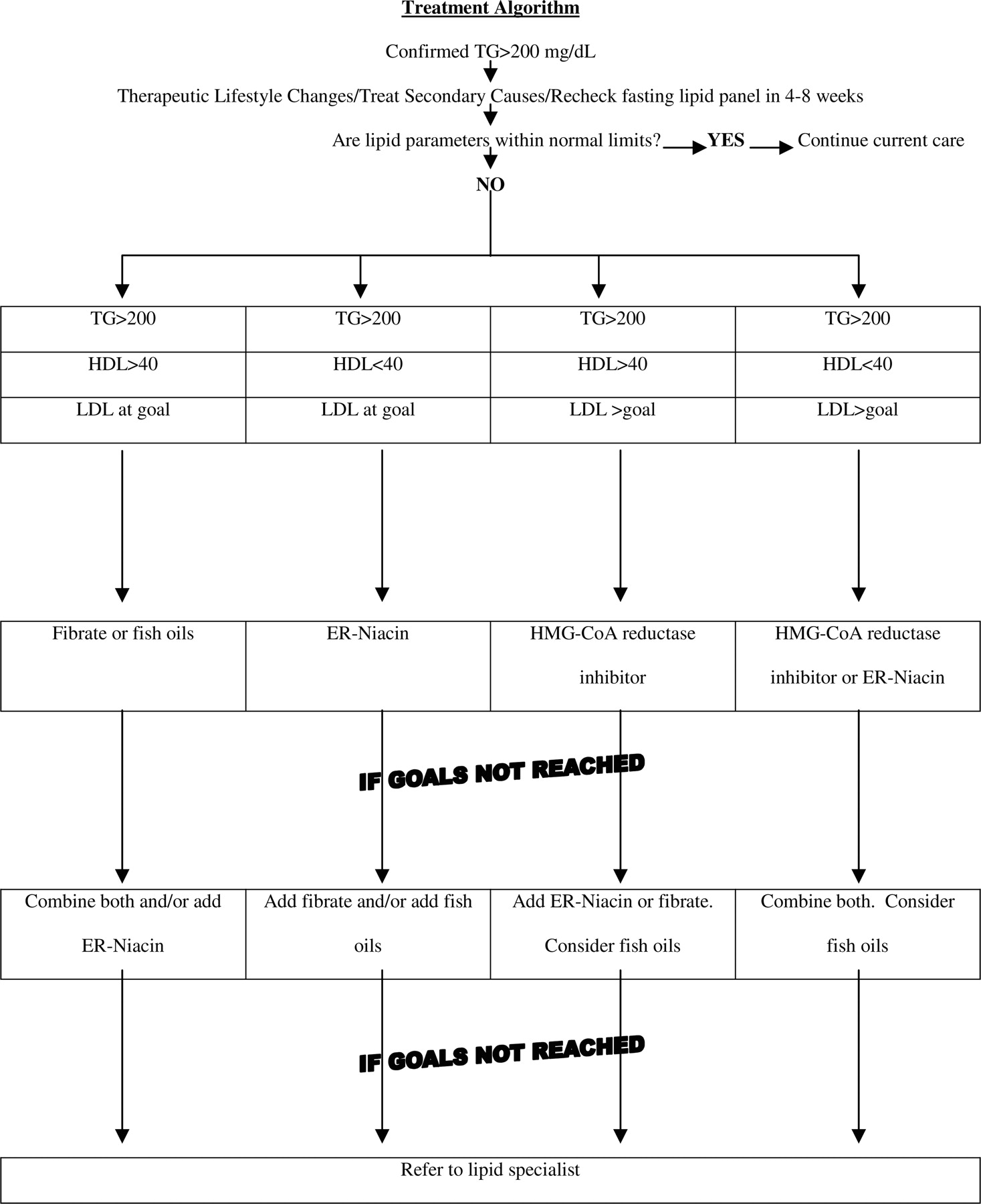
Treatment Algorithm.
Treatment Guidelines for Hypertriglyceridemia.
In cases of isolated hypertriglyceridemia, fibrates, such as gemfibrozil and fenofibrate, may be used because they are potent reducers of triglycerides. Furthermore, fish oil supplementation may be added to augment the fibrate treatment, and in some cases, the patient may elect to try fish oil supplementation as first line. Fish oils have a dose-dependent effect and many patients will need 2 g to 4 g a day of fish oil supplementation to achieve goals. Omega-3 fatty acids (4 g per day) will reduce triglyceride levels by 30%.19,20 However, at this dosage, omega-3 will elevate the LDL by 5% to 10% and will have little effect on the HDL.20 Fish oil capsules can be taken at any time of the day, with or without food, together or in divided doses. However, as the capsules dissolve in the stomach and release the oil, many people experience a “fishy burp.” Taking the capsule at bedtime, freezing them, taking enteric-coated capsules, or taking them with food may minimize or eliminate this problem.21
In many circumstances, the LDL is elevated in addition to the triglycerides. In these cases, the 3-hydroxy-3-methylglutaryl coenzyme A (HMG-CoA) reductase inhibitors (statins) should be used to lower the LDL to the patient’s goal based on NCEP ATP III guidelines.1 Niacin or fibrates may be added if the LDL and/or the triglycerides remain too high. However, physicians should add fibrates with great caution as combining them with the HMG-CoA reductase inhibitors increases the risks of severe myopathy and hepatoxicity. This combination particularly should be avoided in the elderly, in patients with acute or serious chronic illnesses (especially chronic renal disease), in those undergoing surgery, and in patients receiving multiple medications.22
For other mixed dyslipidemias involving high triglycerides and low HDL, niacin may be considered. There are 3 available preparations of niacin: immediate acting, long acting, and extended release. Immediate acting niacin must be taken 3 times daily and is associated with flushing, hyperglycemia, and gastrointestinal side effects. The long-acting preparation can be taken once daily and has less flushing. However, with its absorption time lasting generally greater than 12 hours, it carries a higher risk of hepatotoxicity and therefore is not recommended. The best preparation of niacin to be prescribed is extended release (ER) niacin.23 ER niacin has a lower rate of flushing and no additional risk of hepatotoxicity as is found with the long-acting preparations. Furthermore, ER niacin can be dosed once daily resulting in better adherence because it is typically absorbed over 8 to 12 hours. ER niacin has been shown to lower the triglyceride level by ∼25% and raise the HDL level by almost 30%.24 To prevent flushing, a low starting dose of niacin should be taken immediately after the evening meal and increased at monthly intervals. In addition, aspirin (325 mg) may be taken 30 to 60 minutes before any form of niacin to further reduce the incidence of flushing. Niacin should be used with caution in patients with diabetes (including glucose intolerance) and gout as it may increase blood sugar and uric acid levels, respectively. Niacin is contraindicated in patients with active peptic ulcer disease.
Finally, it is important to note that patients with severe hypertriglyceridemia (over 1000 mg/dL) often need a combination of medicines to achieve their goal (Figure 1). In addition, they will benefit from strict adherence to TLC including a very low fat diet and complete abstinence from alcohol. If patients do not reach their goals with the above treatment regimens, a referral to a lipid specialist and medical dietician may be warranted. In addition, keep in mind that some physicians may be tempted to add bile acid binding resins to help treat elevated total cholesterol and LDL. However, these medications can worsen triglyceride levels and should not typically be used in patients with significantly elevated triglycerides.25,26
Follow Up
If medical treatment is started, patients may have their lipids tested as soon as 1 to 2 months after initiating treatment because the full effect of the medicines are seen within this time interval. Furthermore, this allows for titration of the medicines to appropriate levels in an expedient manner.26 This testing interval may continue until the therapeutic goal is reached. Once stable, the interval between testing can be extended to every 6 months. It is reasonable to monitor liver enzymes concurrently with every lipid draw while on lipid medications. Patients taking niacin should also have their blood sugar and uric acid levels checked routinely as indicated.
While treating patients for hypertriglyceridemia, patients should be monitored for development of the metabolic syndrome. Specifically, patients should have their blood pressure, fasting blood sugar, and weight measured at regular intervals. Clinicians should encourage patients to adhere to their diet and exercise program. Referral to a dietician is recommended for formal medical nutrition therapy if patients fail informal dietary counseling. Finally, every attempt should be made to help patients stop smoking cigarettes and reduce their alcohol intake.
Notes
Conflict of interest: none declared.
- Received for publication August 17, 2005.
- Revision received October 24, 2005.
- Accepted for publication October 31, 2005.




{kind=link}