
Article Figures & Data
Figures
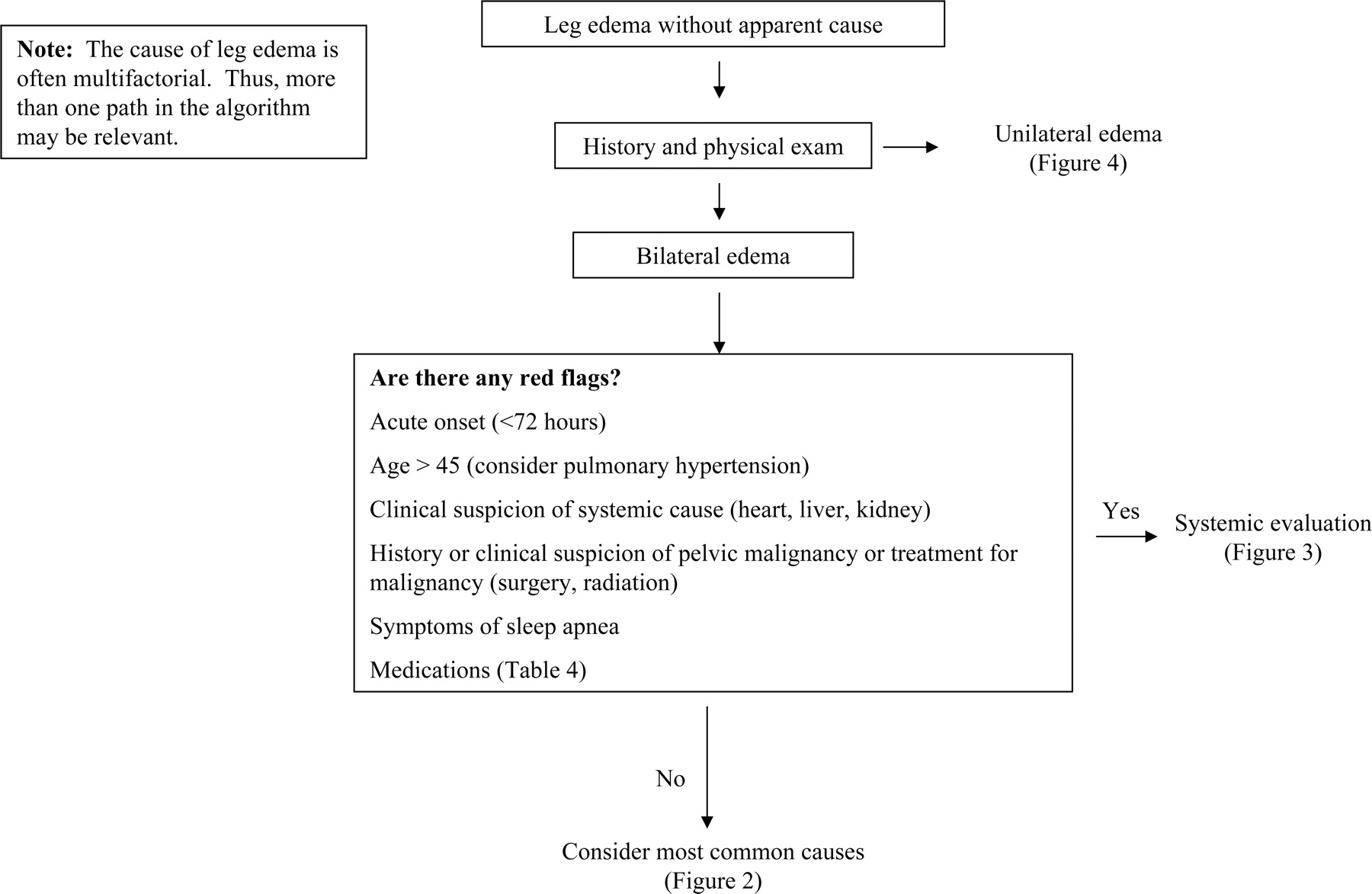
- Figure 1.
Algorithm for leg edema.
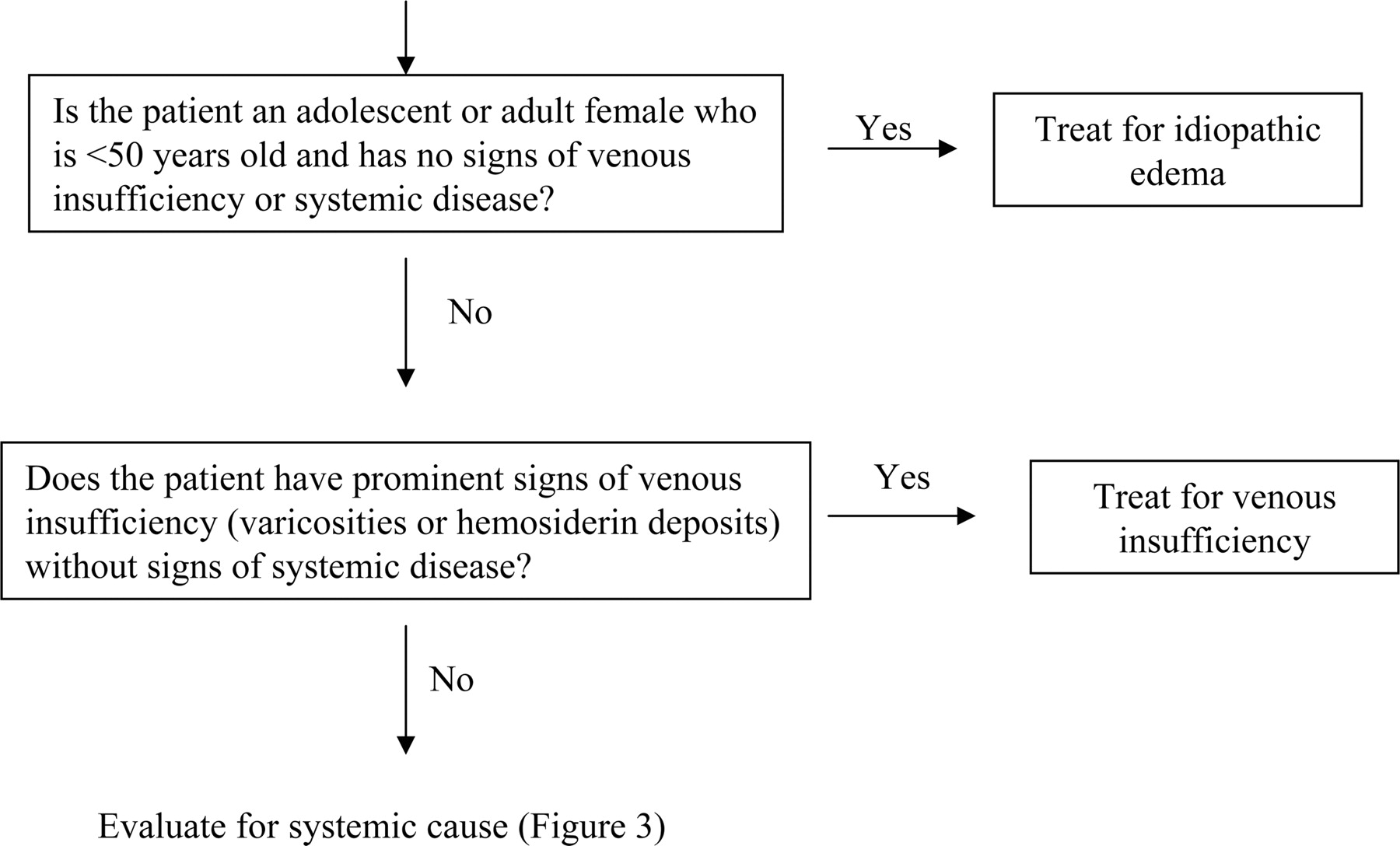
- Figure 2.
Common causes.
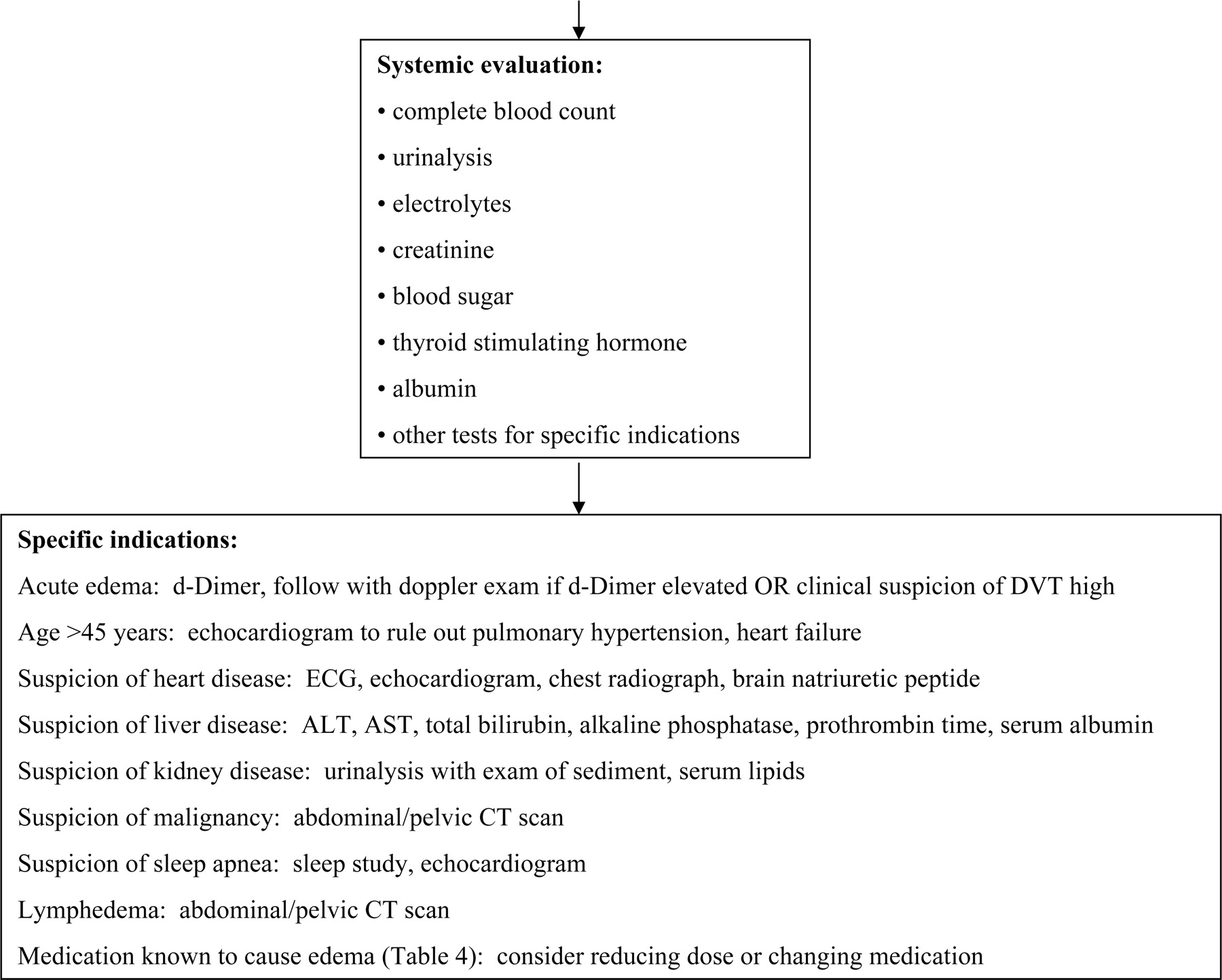
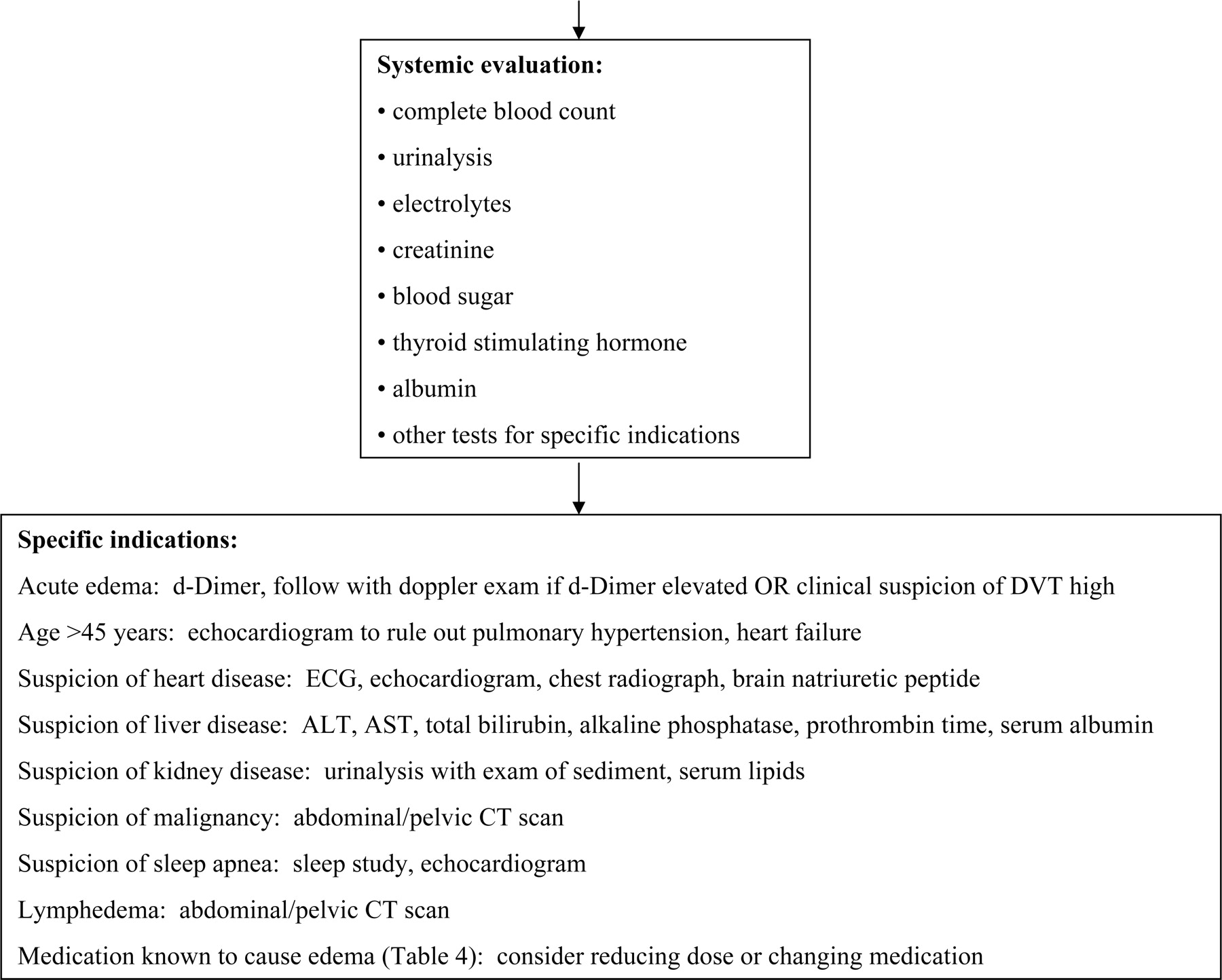
- Figure 3.
Systemic evaluation.
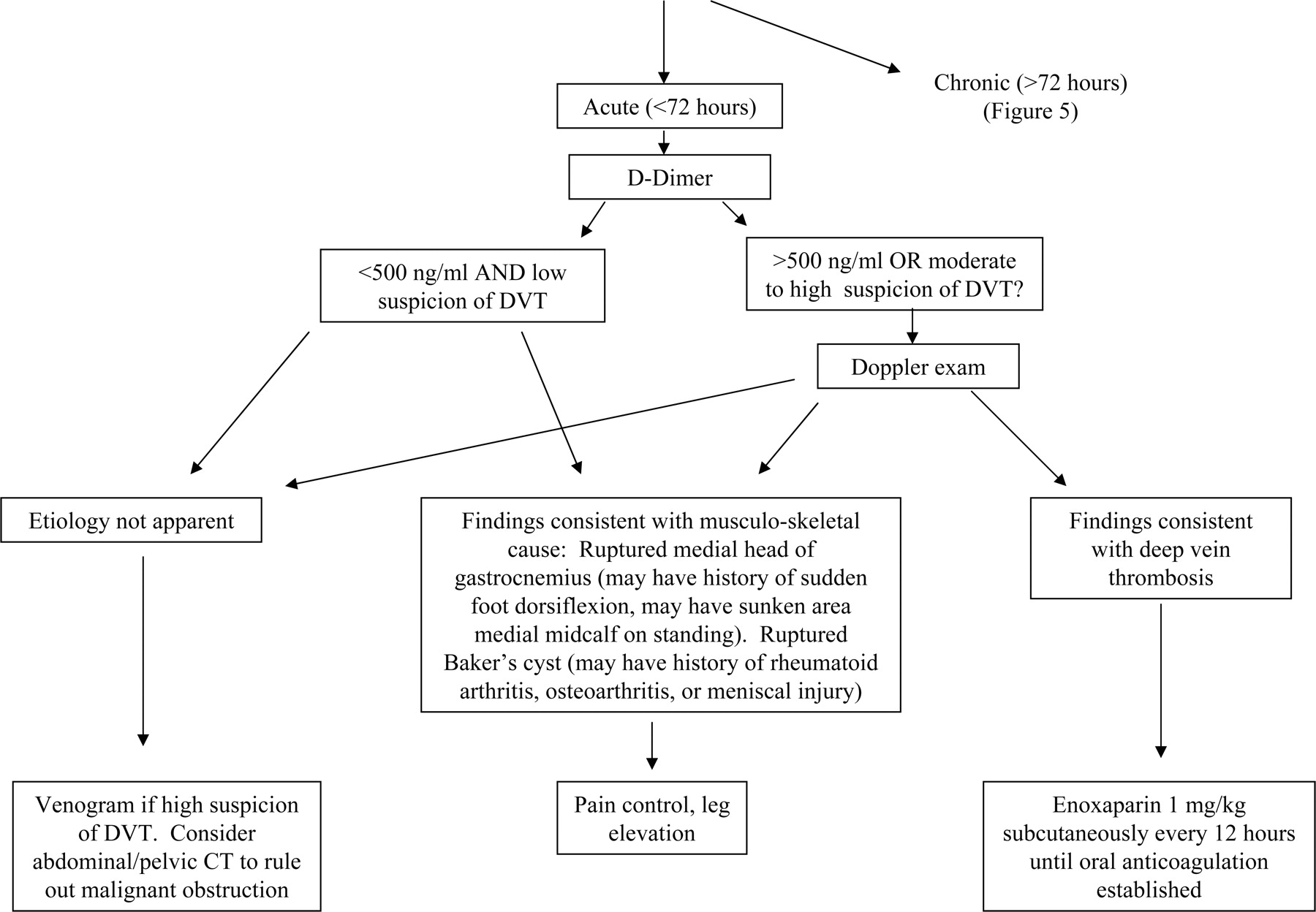
- Figure 4.
Unilateral edema.
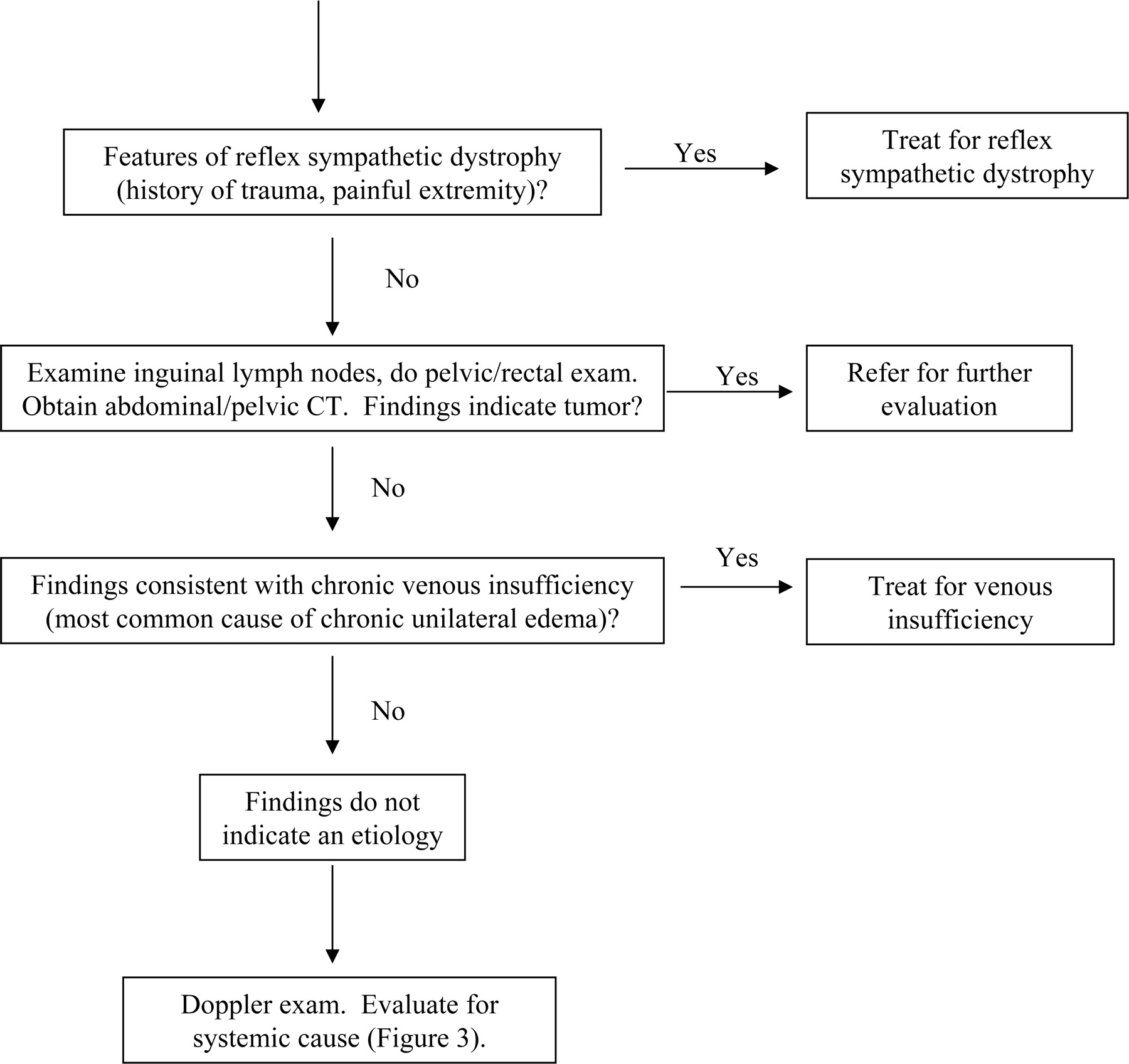
- Figure 5.
Chronic unilateral edema.



Tables
Unilateral Bilateral Acute (<72 hours) Chronic Acute (<72 hours) Chronic Deep vein thrombosis Venous insufficiency Venous insufficiency Pulmonary hypertension Heart failure Idiopathic edema Lymphedema Drugs Premenstrual edema Pregnancy Obesity Unilateral Bilateral Acute (<72 hours) Chronic Acute (<72 hours) Chronic Ruptured Baker’s cyst Secondary lymphedema (tumor, radiation, surgery, bacterial infection) Bilateral deep vein thrombosis Renal disease (nephrotic syndrome, glomerulonephritis) Ruptured medial head of gastrocnemius Pelvic tumor or lymphoma causing external pressure on veins Acute worsening of systemic cause (heart failure, renal disease) Liver disease Compartment syndrome Reflex sympathetic dystrophy Secondary lymphedema (secondary to tumor, radiation, bacterial infection, filariasis) Pelvic tumor or lymphoma causing external pressure Dependent edema Diuretic-induced edema Dependent edema Preeclampsia Lipidema8 Anemia Unilateral Bilateral Acute (<72 hours) Chronic Acute (<72 hours) Chronic Primary lymphedema (congenital lymphedema, lymphedema praecox, lymphedema tarda) Primary lymphedema (congenital lymphedema, lymphedema praecox, lymphedema tarda) Congenital venous malformations Protein losing enteropathy, malnutrition, malabsorption May-Thurner syndrome (iliac-vein compression syndrome)51 Restrictive pericarditis Restrictive cardiomyopathy Beri Beri Myxedema Antihypertensive drugs Calcium channel blockers Beta blockers Clonidine Hydralazine Minoxidil Methyldopa Hormones Corticosteroids Estrogen Progesterone Testosterone Other Nonsteroidal anti-inflammatory drugs Pioglitazone, Rosiglitazone Monoamine oxidase inhibitors Morning and Evening Weights: Patients should weigh themselves nude and with an empty bladder before food or fluids in the morning and at bedtime. A mean weight gain >0.7 kg is consistent with idiopathic edema. Water Load Test: After avoiding diuretics for at least 10 days, the patient drinks 20 mL/kg body weight (maximum 1500 mL) uniced water over 20 minutes, sometime between 7:30 AM and 9:00 AM. The patient collects urine every hour, starting 1 hour before the oral fluid load and ending 4 hours after. On the first day, the patient should be walking slowly or standing during this 4-hour period. On the second day, the patient repeats the fluid load and urine collection, but should be recumbent during the 4-hour period. In patients with idiopathic edema, less than 55% of water load is excreted in the upright position and more than 65% in the recumbent position. Strength of Recommendation* Diagnostic recommendations Relative frequencies of causes of edema in Tables 1–31,4,53 C Clinical findings that help distinguish venous edema, lymphedema, and lipidema8,9,11,12,21,22,24 C Important components of the patient history9–12,24,54 C Important components of physical exam2,9–12,22,24 C Echocardiogram recommended in patients over age 454 C Medications that cause edema4,13,14,16,17,24,55 C Normal D-dimer rules out deep vein thrombosis25,56 B Use of Doppler exam to confirm or rule out deep vein thrombosis57–59 B Treatment recommendations Diuretics to treat venous insufficiency2 C Horse chestnut seed extract to treat venous insufficiency41–44 B Compression stockings to treat venous insufficiency60 C Diuretics to treat idiopathic edema5,31,46 C * Strength of recommendation classified according to the 3-component SORT system61: A, denotes recommendation based on consistent and good-quality patient-oriented evidence61; B, denotes recommendation based on inconsistent or limited-quality patient-oriented evidence61; C, denotes recommendation based on consensus, usual practice, opinion, disease-oriented evidence, or case series for studies of diagnosis, treatment, prevention, or screening.61
Question Answer Who needs a pelvic and rectal exam to rule out tumor? We recommend a pelvic/rectal exam in patients who present with findings suspicious for tumor, such as unilateral edema, pelvic symptoms, or weight loss. We were unable to find evidence or published opinions on when the pelvic or rectal exam is indicated in patients with edema The pelvic exam has poor sensitivity compared with computed tomography (CT) scan for detection of pelvic tumors that cause leg edema. However, information gained from this part of the exam may complement subsequent radiologic studies. Who needs an abdominal/pelvic CT scan to rule out tumor? An abdominal/pelvic CT scan should be considered in patients over 40 without an apparent cause for edema and in younger patients with suspicious findings (unilateral edema, pelvic signs or symptoms, weight loss). Patients over age 35 with undiagnosed lymphedema should have a CT scan.11 Tumors commonly associated with leg edema include prostate cancer, ovarian cancer, and lymphoma.11,12 Who needs to be evaluated for a systemic cause, and what tests should be done? It is reasonable to obtain a few basic tests in all patients with bilateral leg edema over age 45 because the tests are relatively few and inexpensive. The basic tests include a complete blood count, urinalysis, electrolytes, creatinine, blood sugar, thyroid-stimulating hormone, and serum albumin. An echocardiogram should be considered in patients over age 45, because pulmonary hypertension is a common cause of leg edema and is commonly missed.4 Unilateral edema generally does not require a search for a systemic cause. A search for liver disease is unnecessary in the absence of ascites because leg edema is a late finding in patients with cirrhosis. When should diuretics be used and when should they be avoided? Loop diuretics (eg, furosemide, 40 mg daily) should be used in patients with edema secondary to heart failure or renal failure.62 Patients with ascites and leg edema due to cirrhosis should be treated with spironolactone (starting with 50 mg daily) combined with furosemide (starting with 40 mg daily).63,64 In patients with chronic venous insufficiency, diuretics should be used only after leg elevation and compression stockings have failed. At that point, they should be used sparingly and for brief periods. In patients with idiopathic edema who are taking diuretics, a 3 to 4 week trial off diuretics is indicated. In patients with idiopathic edema who are not already taking diuretics or those who fail to improve off diuretics, spironolactone and thiazides can be used. Long-term furosemide use in patients with idiopathic edema has been associated with impaired renal function.65 Diuretics should be used rarely if at all in patients with lipidema, lymphedema, and deep vein thrombosis.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Cross-sectional study investigating the relationship between pit recovery time and serum albumin levels in bilateral lower extremity pitting oedema
- The Most Frequently Read Articles of 2021
- Combined Use of Calcium-channel Blockers With Ombitasvir/Paritaprevir/Ritonavir Exacerbates Peripheral Edema in Elderly Japanese Patients
- The Most Frequently Read Articles of 2020
- The Most Frequently Read Articles of 2019
- Content Usage and the Most Frequently Read Articles of 2018
- Phlegmasia cerulea dolens from radiation-induced venous stenosis
- Adrenocortical carcinoma presenting as bilateral pitting leg oedema
- Unilateral lower extremity swelling as a rare presentation of non-Hodgkin's lymphoma
- Swollen right leg: Is it deep vein thrombosis?
- Content Usage and the Most Frequently Read Articles in 2010
- Content Usage and the Most Frequently Read Articles in 2009
- A 79 year old woman with a swollen right leg
- Introduction of More Editorial Board Members and New Guest Commentary Feature
- Reliability and Feasibility of Methods to Quantitatively Assess Peripheral Edema
- Introduction of More Editorial Board Members and the Most Frequently Read Articles in 2008
- Inside the March/April 2008 Issue and the Most Frequently-Read Articles in 2007