
Abstract
Because of their frequent encounters with sedentary patients, family physicians are poised to be on the forefront of the medical community’s response to physical inactivity. The purpose of this pilot study was to examine whether the addition of a pedometer to brief physician counseling could help patients increase their ambulatory activity. Ninety four participants recruited from a family medicine clinic were randomly assigned to 2 groups. Both groups received a brief physician endorsement of regular physical activity, a handout on the benefits of an active lifestyle, and 3 follow-up phone calls from a health educator. In addition, the intervention group received a pedometer and was instructed to record their steps daily over the 9-week study period. Measurements were taken for self-reported walking, walking stage-of-change, walking self-efficacy, and pedometer steps (intervention group only). Among completers, mean daily step counts in the pedometer group rose from 6779 at baseline to 8855 at study end. Average individual improvement was 41% over the study period. Both groups significantly increased blocks walked per day, stair climbing versus using the elevator, days per week walking ≥30 minutes, and walking for fun/leisure. The frequency of walking short trips improved significantly more in the pedometer group relative to the comparison group. The results of this pilot study highlight the need for further research on the use of pedometers as a motivational tool in the context of medical encounters with inactive patients.
Physical inactivity is widely recognized as a major threat to public health.1 In the United States, physical inactivity combined with a poor diet accounts for an estimated 16% of the actual causes of death and approximately 24.4 billion dollars per year in health care expenditures alone.2,3 In contrast, a physically active lifestyle has been associated with health benefits that include improved control of hypertension, diabetes, obesity, hyperlipidemia, and reduced overall morbidity and mortality.1,4–6 An objective of Healthy People 2010 is that adults engage in at least 30 minutes of moderate physical activity on most, preferably all, days of the week.7 More than 60% of US adults, however, do not achieve this amount and are, by definition, insufficiently active.1
The average US citizen visits a physician 3 times per year, more than half of these are to see a primary care physician.8 Over 25% of visits to physicians involve patients with 6 or more annual encounters, and the average age of patients is on the rise.9 Elderly patients and those who make multiple medical visits may require the extra care because of the sequelae of inactive lifestyles. Family physicians, by virtue of their role in preventive health and their increasing encounters with inactive patients, are poised to be on the forefront of the medical community’s response to physical inactivity.
Although it has long been advocated that physicians promote physical activity with their patients,10 few provide adequate exercise advice.11,12 Lack of time, inadequate reimbursement, and unfamiliarity with counseling techniques are among the most widely cited barriers.13 In addition, many physicians do not believe that physical activity counseling is effective, and recent reviews of clinical trials lend support to this skepticism.14–16 To be applicable to the current demands of family medicine, interventions must prove effective while remaining brief, simple, and inexpensive.
Walking is one of the most prevalent, advocated, and beneficial forms of leisure time physical activity.1,7,17 It is accessible and safe for most sedentary persons. Pedometers have been found to be a valid method for assessing walking.18,19 They capture changes in lifestyle ambulatory behaviors (eg, walking short trips and climbing stairs) that are not typically considered exercise, but in fact help to increase energy expenditure. Researchers have noted significant improvements in weight management, insulin sensitivity, blood pressure, and lipid profiles, as a result of participation in programs using pedometers.20–24 Although most research to date has involved physical activity assessment, pedometers may also motivate increased activity levels by increasing cognitive awareness1 and self-efficacy.18 Pedometers are beginning to show promise in the medical setting, where they have been recently studied for patients with the specific conditions of diabetes and osteoarthritis.20,21 To date, however, the efficacy of using pedometers in the context of family medicine encounters is unknown.
The purpose of this investigation was to examine whether pedometers could help patients increase their lifestyle ambulatory activity. To isolate the impact of the pedometer, a randomized comparison group received similar treatment (brief physician advice and telephone follow-up) without a pedometer. Given the pilot nature of this study, we were primarily interested in answering the following research questions. Would the intervention group use the pedometer over the course of the study? Would completers in the intervention group increase their steps over the course of study? Would the intervention group show a greater increase in walking relative to the comparison group? To assess lifestyle walking behavior, we piloted a 7-item Lifestyle Walking Questionnaire (LWQ) as a self-report measure. Secondarily, we measured stage-of-change and self-efficacy to assess how they co-vary alongside activity changes.
Methods
Design and Participants
This study was approved by the University of Minnesota’s Institutional Review Board and conducted at the University’s family medicine residency clinic in semi-urban Minneapolis. Over a 2-week period in the spring of 2003, all patients who presented to the clinic while the principal investigator and a research assistant were both available were considered as potential participants. Patients were recruited while waiting to be seen for their office visit. Inclusion criteria were ≥18 years old, ability to provide information over the phone, and conversational competence in English. Exclusion criteria were contraindications to increased walking (eg, pneumonia, acute knee pain, unstable angina), disordered eating, and pregnancy.
A randomized controlled design with precomparison and postcomparison was used. To minimize disruption to clinic flow and respect for patient privacy, patients that were unavailable in the waiting room or that expressed a disinterest in participation were not tracked. For those that were available and interested, a research assistant reviewed the study procedures and asked if they wished to participate. Patients who agreed then provided written informed consent and completed baseline questionnaires (see Dependent Measures). The research assistant then placed a previously randomized, sealed envelope on each patient’s medical chart that contained their group assignment. During the office visit, the physician verified patient eligibility based on inclusion/exclusion criteria. The physician, research assistant, or any other clinic personnel did not know group assignments. Demographic information was collected from medical charts during patients’ initial office visit. Enrollment was discontinued after 50 participants had been randomized to the pedometer group.
Intervention Procedures
All office visits were conducted in the usual manner, with the following exception: immediately before or after the office visit, the principal investigator (SDS) entered the room and made a brief scripted statement endorsing the benefits of increased physical activity. He then opened the patient’s sealed chart envelope and presented the appropriate treatment protocol based on group assignment. The physician message was designed to last approximately 1 minute as suggested by Stange and colleagues.16
Participants assigned to the intervention group were given a pedometer (with a demonstration of its use) and a one-page handout that summarized the benefits of physical activity, as well as a 9-week calendar to be used as a step log. Intervention participants were instructed to wear their pedometer each day (from the time they got up until the time they went to bed) and record their daily step totals in the log. Participants in the comparison group were given a similar one-page handout summarizing the benefits of physical activity and a calendar analogous to a step log. They were encouraged to use this calendar as a guide for recording physical activity, whatever they deemed appropriate. All participants were instructed to continue their usual levels of activity for the first week to obtain a baseline.
After the first week, all participants were contacted by telephone from a health educator (JJV). Those in the pedometer group were encouraged to try to increase their daily average pedometer steps by 400 each week. The number 400 was selected because prior testing revealed that activities of daily living required approximately 4000 steps per day. An additional 400 steps per day represented approximately a 10% increase above baseline, which was considered a meaningful and achievable goal. A predetermined activity prescription, such as 10,000 steps per day, was not recommended because it is unclear how many steps are actually needed to meet current physical activity guidelines,18 and even minimal improvements are known to benefit inactive persons.1 Participants in the comparison group were also encouraged to increase their physical activity level by 10% each week, but were not given a pedometer.
The health educator phoned participants during week 5 to encourage participation and after week 9 to collect data from the postintervention questionnaire, step logs (pedometer group only), and a brief qualitative exit survey. Near study end, participants were also sent a letter with all questionnaires enclosed so they would have the option of either mailing in their assessments or submitting them by phone.
Dependent Measures
The primary outcome for the pedometer group was ambulatory activity as measured by pedometer steps. Participants in the pedometer group were given a Yamax Digi-walker (model SW-200) pedometer and instructed to record daily step totals. The Digi-walker is generally considered among the most reliable and valid pedometers available.18,19 Step counts needed to be recorded for at least 3 days each week for averages to be considered reliable and two-thirds of days overall for adherence to the study protocol.
An additional dependent measure, both within and between groups, included ambulatory activity as assessed by the LWQ. The LWQ is a 7-item instrument (see Appendix) designed by the investigators to quantify walking behavior under common “lifestyle” circumstances (eg, short errands, using stairs, leisure walks). A pilot test of the LWQ (n = 37) indicated acceptable 4-week, test-retest reliability (mean 0.49, range for each item 0.11 to 0.80).
Other dependent measures included known behavioral mediators of physical activity, stage-of-change, and self-efficacy.25 Stage-of-change for walking was based on a behavioral criterion, operationally defined as walking at least 30 minutes per day (cumulative) on most days of the week. Specifically, walking stage-of-change was measured using a 5-choice response format. Participants selected the response that best represented their walking activity. Responses included:
I currently do not walk regularly, and I do not intend to do so within the next 6 months (precontemplation).
I currently do not walk regularly, but I intend to do so within the next 6 months (contemplation).
I currently walk some, but I intend to start walking regularly within 30 days (preparation).
I have begun walking regularly within the last 6 months (action).
I walk regularly and have done so for at least the last 6 months (maintenance).
In addition, participants completed a 5-item measure of self-efficacy for regular walking. This instrument was adapted from a similar validated instrument designed to measure exercise self-efficacy.25 On a scale from 1 to 7, participants were asked to rate how confident they were that they could engage in regular walking when: tired, in a bad mood, limited on time, on vacation, and in bad weather. Scores for each item were summed to produce a walking self-efficacy index. Pilot testing of both the stage-of-change and self-efficacy instruments (n = 37) indicated good test-retest reliabilities (0.71 and 0.83, respectively).
Statistical Analyses
Analyses included comparing the change in scores between groups using an intent-to-treat principle (ie, baseline scores carried forward for participants unavailable at follow-up). An intent-to-treat analysis was not possible for step-counts on those that were unavailable by phone at week 2 as baseline steps would be unknown. Given the pilot nature of this study and the novelty of using pedometers in a family medicine setting, a treatment-received analysis (ie, completers only) was conducted within and between groups.26 Continuous variables were examined using t tests. Stage-of-change movement was examined using χ2 tests. All analytical procedures were computed using the statistical package for the social sciences (SPSS Inc., Chicago, IL) with a 0.05 α level as the criterion for statistical significance.
Results
Participants presented to the clinic for routine visits as described in Table 1. The pedometer (N = 50) and comparison group (N = 44) were similar at baseline in terms of gender, body mass index, and cardiovascular risk factors (Table 2). Age was the only exception because participants in the comparison group were significantly older than those in the intervention group (t = 2.30, P = .024). Previous research suggests that this difference is negligible in terms of physical activity levels.27
Primary Reason for Office Visit
Baseline and Poststudy Characteristics of All Randomized Participants*
Forty four participants (47%), 21 from the pedometer group and 23 from the comparison group, were included in the final analyses. Forty five participants did not provide follow-up data, and 5 participants from the pedometer group were excluded because of insufficient data (ie, did not record steps on at least two-thirds of all study days). Baseline comparisons between completers and noncompleters indicated that completers were significantly older (46.6 vs 36.0, t = −4.17, P < .001), reported climbing fewer stairflights per day (5.4 vs 7.6, t = 6.259, P = .014), and were more likely to be male (22 vs 9, χ2 = 9.44, P = .002).
The intent-to-treat analysis did not reveal any significant changes between the pedometer and comparison group (see Table 2). An intent-to-treat analysis was not possible for pedometer steps because week 1 (ie, baseline) step values were not available from 16 participants in the pedometer group who couldn’t be reached for the week 2 follow-up call. The treatment-received analysis revealed the following.
Pedometer Steps
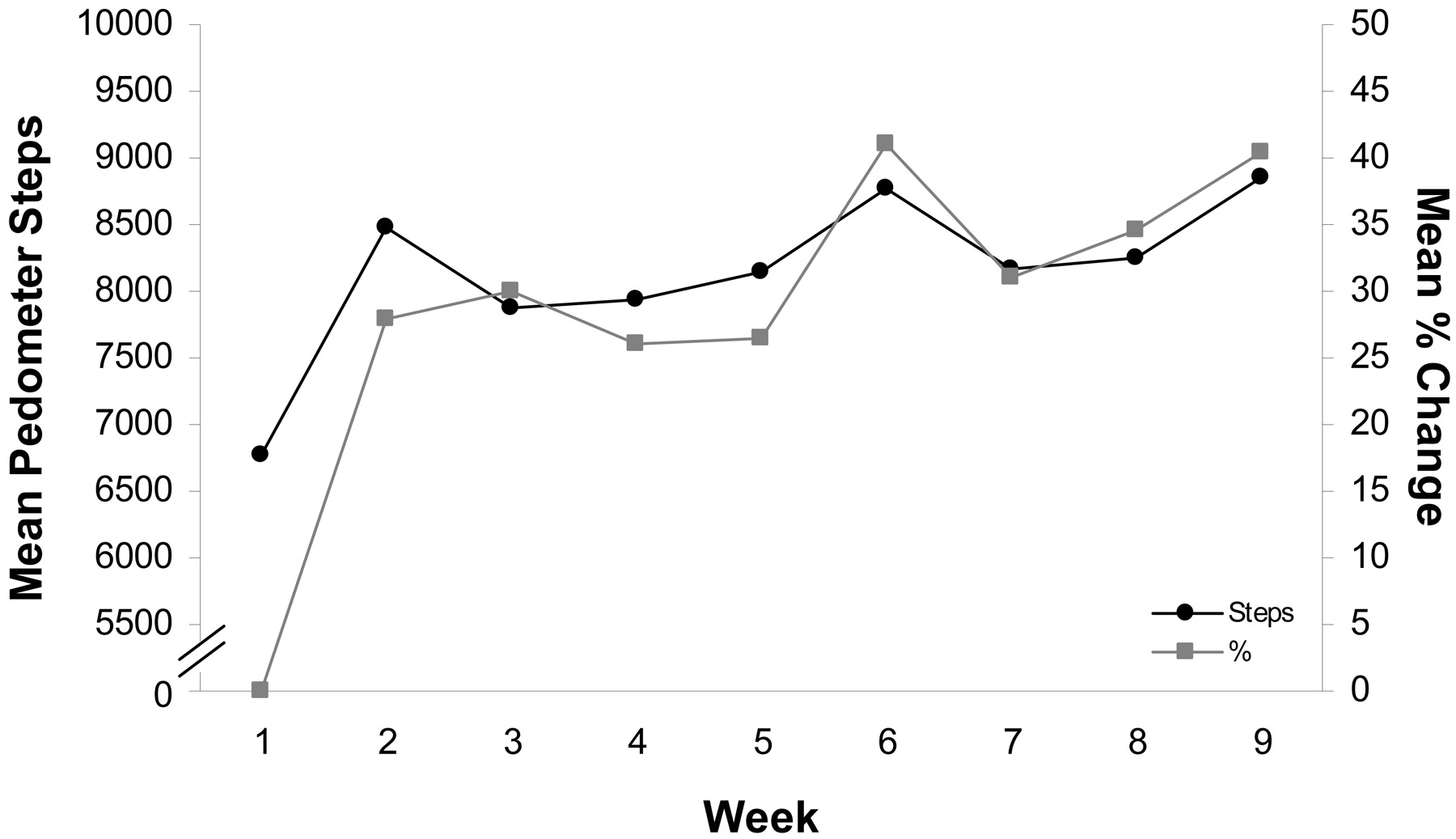
As outlined in Figure 1, pedometer steps significantly increased from a mean of 6779 ± 4079 steps per day during week 1 to 8855 ± 4690 steps per day by week 9 (t = 3.17, P = .005). Average improvement per person was 41%. Of the 17 participants in the pedometer group who were in the preaction stages at baseline (ie, precontemplation, contemplation, or preparation), mean daily steps increased by 26% between weeks 2 and 9. By comparison, the 4 participants in the pedometer group who were in the action or maintenance stages at baseline increased their mean daily steps by 59% during the same time frame.
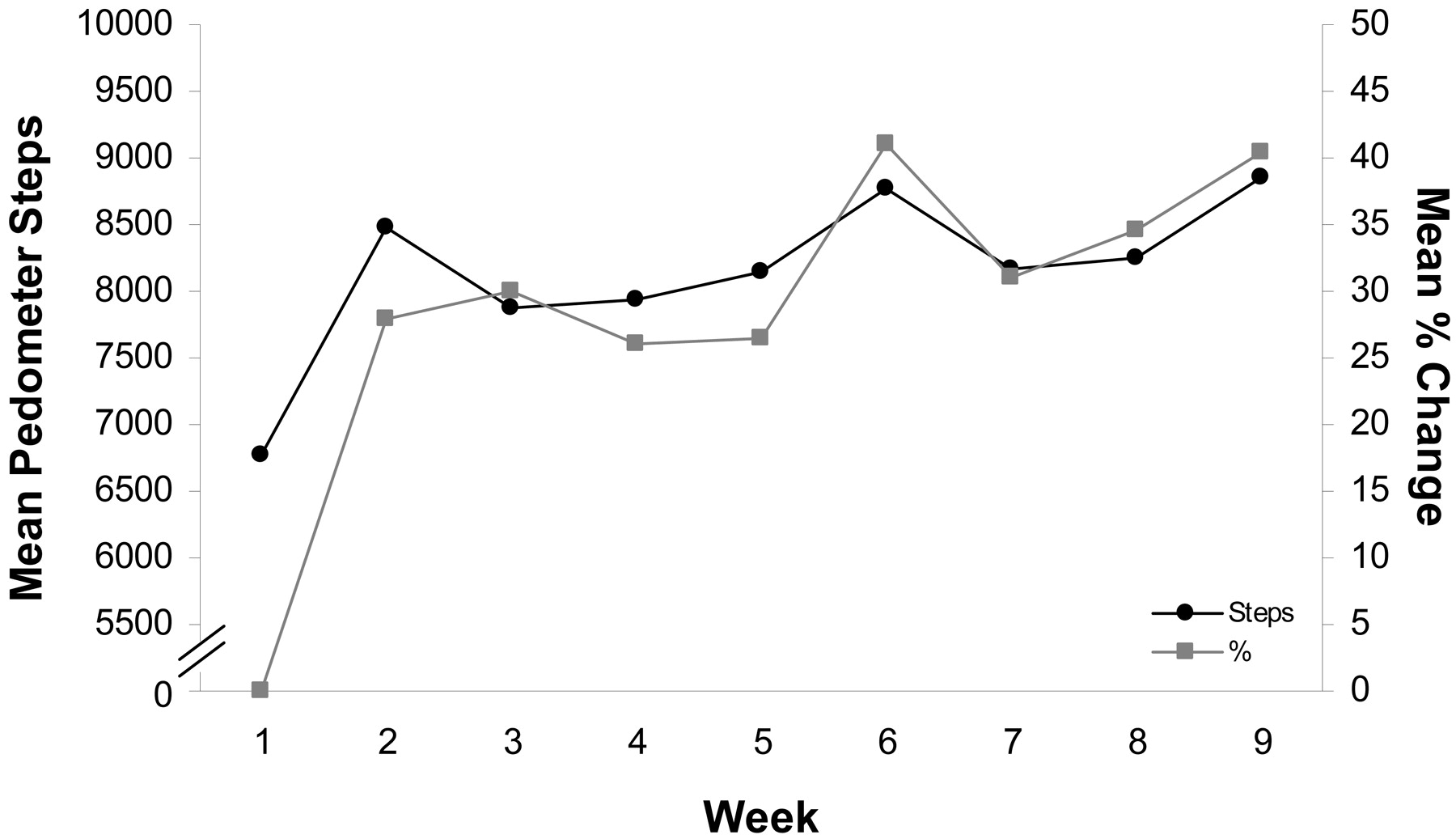
Mean (and percentage) of step improvement for the pedometer group.
LWQ
At baseline, there were no significant differences between groups on any of the LWQ items (see Table 3). Within the comparison group, there was significant improvement between baseline and poststudy for reported blocks walked per day (t = 2.94, P = .008), stairs would climb versus elevator (t = 2.27, P = .033), days per week walking ≥30 minutes (t = 4.27, P < .001), and walking for fun/leisure (t = 2.15, P = .043). Within the pedometer group, there was significant improvement between baseline and poststudy for blocks walked per day (t = 3.30, P = .004), blocks would walk versus ride (t = 2.31, P = .031), stairs would climb versus elevator (t = 3.07, P = .006), days per week walking ≥30 minutes (t = 2.96, P = .008), walking short trips (t = 4.54, P < 0.001), and walking for fun/leisure (t = 2.61, P = .017).
Change in LWQ Items and Walking Self-Efficacy among Completers
The pedometer group reported a significant increase in walking for short trips relative to the comparison group (t = 2.53, P = .015). The pedometer group also showed a nonsignificant trend of greater improvement on 5 of the remaining 6 LWQ items. A large difference (d = 0.87) between the groups would have been needed to achieve a power of 0.80.
Walking Stage-of-Change
Walking stage-of-change progression is summarized for both groups in Table 4. Both groups advanced in their stage assignments, but there was no significant difference between groups on the number of participants who progressed ≥1 stage over the course of the study.
Walking Stage-of-Change Movement among Completers
Walking Self-Efficacy
Walking self-efficacy increased slightly in the comparison group and decreased slightly in the pedometer group. The changes were not significant (see Table 3).
Discussion
This pilot study was designed to test the efficacy of a physician delivered intervention using a pedometer to improve physical activity levels in patients seen for routine visits to a family medicine clinic. It was hypothesized that pedometers may serve as a motivating tool to inactive patients and thus enhance physician-based counseling. The intervention was designed to be applicable within the time constraints of modern medical practice.
Given the novelty of using pedometers in the context of primary care medicine, we were first interested in learning whether participants would be adherent with their use. Forty two percent of patients randomized to the pedometer group were adherent over the 9-week study period. In addition, we wanted to know whether those that completed the study would increase their step-counts. Completers in the pedometer group increased their steps by an average of 41% by study end. Step counts increased by an average of 2089 per day, which corresponds to approximately 20 minutes of increased walking.
To delineate the effect of the pedometer over the other interventions, a comparison group received similar treatment but was not given a pedometer and thus lacked the ability to objectively record their daily steps. The 2 groups were compared using the LWQ, along with stage-of-change and self-efficacy scales. Participants in both the pedometer and comparison groups increased several aspects of their walking behavior over the course of this 9-week study. By study end, 8 participants from each group reported walking at a level that met or exceeded the physical activity objective of Healthy People 2010.7 Although the pedometer group showed greater improvement on 6 of the 7 LWQ items, this was not statistically significant. Stage-of-change improvement was similar between groups. Self-efficacy decreased by a nonsignificant amount in the pedometer group relative to the control group. Although self-efficacy has been listed as a determinant of physical activity, it may have decreased in the pedometer group because recording daily steps may give participants more precise awareness of their physical activity barriers.28
Increased walking may be an especially important component of a healthy lifestyle because it is perhaps the safest and most accessible form of activity. Pedometers reflect cumulative bouts of activity, and thus are responsive to even small increases in walking.29 Activities as short as 8 to 10 minutes, although perhaps not typically perceived as exercise, are cumulatively beneficial toward improving health.7 Small improvements may subsequently “open the door” to more vigorous activity among inactive patients. The average body mass index for the patients in this study was in the obese range, suggesting that pedometers may be a useful tool when counseling those in need of increasing their physical activity levels for the purpose of weight management.
There were several limitations to this study, the most significant being the low completion rate. This was not particularly surprising given the recruitment procedures whereby patients presented for routine indications and had no special motivation to participate in or complete a research study. It was also comparable to similar “real-world” interventions involving physical activity promotion.30 In an attempt to minimize disruption of clinic flow, the number of patients approached was not tracked. Given this, another limitation is potential selection bias. The control group received treatment that was geared to replicate the treatment of the pedometer group, but certainly differed in that their instructions were more general and there were no steps to record. The time of year may have also enhanced participation because spring has been associated with approximately a 15% to 20% increase in activity levels.31 Although the intervention was generally practical within the confines of modern medical practice, phone support from health educators may not be feasible for many clinics.
Physical inactivity has clearly become an epidemic in the United States.1,2 Family physicians are consistently faced with patients suffering the health consequences of their inactive lifestyles. Physician-based physical activity counseling has historically been limited by a perceived lack of effectiveness and concerns that it is too time-consuming.13 Given the time and financial constraints of modern medical practice, the medical community needs to be creative in developing feasible and effective approaches. Most of the intervention procedures in this study would be feasible in modern primary care settings. Participants were patients that presented for routine visits to a family medicine clinic. The intervention was brief, requiring the principal investigator to merely review a one-page handout and, for those in the pedometer group, demonstrate its use. Pedometers are an economically viable intervention (∼$20) and give providers a simple discussion point that may empower them to engage in more in-depth physical activity counseling. Although definitive conclusions regarding effectiveness cannot be drawn from this pilot study because of the limitations discussed above, the results lend promise to the future study of pedometers as a tool to increase activity levels in certain clinic patients.
Future research should attempt to broaden the scope of using pedometers and physician counseling across larger populations. More sensitive and objective primary outcomes (eg, blinded pedometer steps) would enhance the validity of this research. Similar interventions are presently being studied in some diabetic programs20 and may also prove useful for patients with depression and/or anxiety, metabolic syndrome, and obesity. Given that physical activity promotion programs are on the rise in larger urban work sites,7 there may be some benefit to performing a similar study in rural settings. Longer follow-up is also needed to investigate how pedometers may affect the maintenance of increased physical activity.
Appendix
Lifestyle Walking Questionnaire (LWQ)
How many blocks do you walk on a typical day (12 blocks = 1 mile)? (test-retest = 0.80)
How many blocks do you normally walk before choosing to ride in a car or bus? (test-retest = 0.11)
How many flights of stairs do you climb on a typical day (1 flight = 10 steps)? (test-retest = 0.35)
How many flight of stairs do you normally climb before choosing the elevator? (test-retest = 0.32)
How many days per week do you walk for at least 30 minutes total outside the house (not including your job)? (test-retest = 0.59)
How often do you walk when you are running short trips (such as going to the grocery store, shops, post office, school, visiting friends, etc.)? (test-retest = 0.71)
1 = never
2 = ∼1/month
3 = ∼1/week
4 = ∼3/week
5 = ∼1/day
6 = ≥3/day
How often do you walk for fun and leisure (such as walking the dog, hiking a trail, walking with friends/family or alone, etc.)? (test-retest = 0.58)
1 = never
2 = ∼1/month
3 = ∼1/week
4 = ∼3/week
5 = ∼1/day
6 = ≥3/day
Acknowledgments
We thank the HealthPartners Center for Health Promotion for donating the pedometers used in this research. In addition, we gratefully acknowledge the assistance of Nico Pronk, PhD, and Arthur Leon, MD, MS, for their advice and review of study procedures.
Notes
Conflict of interest: none declared.
- Received for publication May 9, 2005.
- Revision received May 9, 2005.
References




{kind=link}
Jump to section
Related Articles
Cited By...
- STRIVE pilot trial: a protocol for a multicentre pragmatic internal pilot randomised controlled trial of Structured TRaining to Improve fitness in a Virtual Environment (STRIVE) before surgery
- PREPARE trial: a protocol for a multicentre randomised trial of frailty-focused preoperative exercise to decrease postoperative complication rates and disability scores
- Prescribing exercise to help your patients lose weight
- Physicians promoting physical activity using pedometers and community partnerships: a real world trial