
Abstract
Context: Access to high quality primary care was identified by Healthy People 2010 as one of the mechanisms through which racial and ethnic disparities in health might be reduced. Despite the well-established connections between good primary care and health, the scientific evidence on whether good primary care can reduce racial disparities in health is sparse.
Objective: To examine whether better primary care experience can attenuate racial and ethnic disparities in self-reported health status.
Data Sources: The 1996 to 1997 and 1998 to 1999 data from the Community Tracking Study (CTS) sponsored by the Robert Wood Johnson Foundation.
Study Design: Cross-sectional, bivariate, and multivariate analyses of inter-relationships between self-rated general and mental health status, access to and interpersonal relationship with primary care provider, and vulnerability measured by race and poverty status.
Results: We found that higher quality primary care levels are associated with reduced racial and ethnic disparities in health status, as measured by self-rated general and mental health. This relationship is particularly pronounced for the racial and ethnic minorities living at or below poverty level. Based on the data from 1996 to 1999, the study also confirmed the presence of significant and persistent health differences across racial and ethnic groups.
Conclusion: Promoting primary care may be a viable approach toward reducing racial and ethnic disparities in self-reported health status.
Despite notable progress in the overall health of the nation, there are continuing disparities in the burden of illness and death experienced by blacks, Hispanics, Native Americans and Alaskans, and Pacific Islanders compared with the United States population as a whole and to the white population in particular.1 In response to the growing evidence of persistent inequalities in health, Healthy People 2010 proposed elimination of health disparities as one of its major goals and outlined potential mechanisms that can help eliminate those disparities.2,3
One of these mechanisms is improved access to high-quality primary care. This recommendation was supported by the substantial research evidence identifying that poor access to and inferior quality of primary care could lead to reductions in the amount of preventive care,4 more fragmented and uncoordinated management of medical problems,5,6 and poorer health outcomes.7–9 Although the positive relationship between good primary care experience and better health outcomes has been well-established at both individual and ecological levels, few published studies exist concerning whether primary care can reduce racial and ethnic health disparities. The logic of the connection between disparity, primary care, and self-rated health is that disparity, by affecting socioeconomic and psychosocial factors, may also exacerbate some risk factors for health. Because primary care is positively related to health, it might ameliorate some of the negative health impact of disparity.
The main objective for this study was to examine the role of primary care experience in reducing racial and ethnic disparities in health status. Using 1996 to 1997 and 1998 to 1999 national data from the Community Tracking Study, this study examined two domains of primary care, accessibility and interpersonal relationship, in terms of their influences on racial/ethnic disparities in general and mental health status. The second objective for the study was to analyze the differential effect of primary care on racial and ethnic disparities by various vulnerability groups identified by the convergence of race and poverty status characteristics. Combining race and socioeconomic status into a single measure of vulnerability recognizes both the independent and congruent influence of race and socioeconomic status on health.
Findings of the study have significant policy implications by identifying whether appropriate interventions targeted at strengthening primary care and improving access to primary care are indeed effective means of reducing racial disparities in health. The evidence based on national data, and on actual individual experiences with primary care, provides more definitive conclusions about the role of primary care in reducing health disparities. In addition, examination of the relationship between vulnerability status, operationalized by racial/ethnic group membership and poverty, and health status will provide better guidance to policy makers in developing programs or interventions that address the broader risk spectrum.
Methods
Data
Four years of data, 1996 through 1999, were drawn from the Community Tracking Study (CTS) household survey, a major initiative of the Robert Wood Johnson Foundation. As a national study of the rapidly changing health care market, CTS is designed to develop an information base to track and analyze changes in health systems and to study how health system change affects health care and health outcomes.
CTS collected data on 60 randomly selected local health care markets (communities) to represent the US population. Within each community, households were randomly selected through a combination of random-digit dialing and a field sample to include and represent households with no telephones or with intermittent telephone service. Information was obtained on all adults in the household and one randomly selected child within each family in the household. All families within a household were interviewed separately in English or Spanish (for respondents not fluent in English). The overall response rate was 65%, an average rate for this type of survey. Stratification by region and systematic sampling by state ensured that the full diversity of health delivery systems across the nation, as well as diversity with respect to historical evolution and community “culture,” is reflected in the study population. More detailed discussions of the response rate, design and scope of CTS have been published elsewhere10,11 and can also be obtained through the web site of the Robert Wood Johnson Foundation (http://www.rwjf.org/nation/jnation.htm).
Several exclusion criteria were applied to yield the analytic sample used by this study. First, the sample was restricted to people whose last visit in the past 12 months was made to their usual source of care—the “place they usually go when they are sick or need advice about their health.” This restriction was made because the primary care experience questions were linked to the practitioner whom the individual last visited. Second, only persons identifying a primary care physician as a usual source of care were included in the study sample for the following reasons. Those identifying specialists were excluded because these persons are likely to be less healthy and therefore would bias the study outcome because of selection bias. Further, the processes of care experienced through a specialist can differ markedly from those experienced in a primary care setting. Observing the primary care effect on health disparities while including respondents with a specialist usual source of care may complicate interpretation. Preliminary analysis indicates that although 11.77% of those with primary care physicians as the usual source of care reported bad health, 17.67% of those with specialists as the usual source of care reported bad health (P < .01). Persons with primary care physicians as a usual source of care also had significantly better SF-12 Physical Health Component Score (36.75 vs 45.42; P < .01) and SF-12 Mental Health Component Score (39.28 vs 49.56; P < .01) than those with specialists as usual source of care. Specialists as a whole are known to perform less well on primary care attributes than do primary care physicians.12–14 The long-term nature of the patient-primary care physician relationship is qualitatively different from most relationships patients have with specialists, which tend to be time-limited and less intense. Although some specialists, such as obstetricians and gynecologists, are often seen by women as their usual primary care provider, the Tracking Survey dataset does not indicate the type of physician specialty once “specialist” is checked.
In addition, persons who identified a hospital emergency department as their usual source of care were excluded because they are less likely to have a regular provider for their needs, thus decreasing the likelihood of having continuity of care.15,16 The poorer continuity of care for primary care visits in emergency department may contribute to a more aggressive practice style, because of less familiarity with patients’ medical and health histories. Greater service intensity and poorer continuity of care in an emergency department setting also raise concern over the suitability of this setting as a primary care delivery site. Those identifying community health centers or hospital outpatient facilities as a usual source of care were retained because these settings have become more popular in recent years and have increasingly served as the primary care safety-net providers for the nation’s uninsured and underinsured.17–20
Measures
Primary Care
Our specification of the principal domains of primary care is consistent with the definition of primary care given in the 1994 Institute of Medicine (IOM) report, which states that primary care is … the provision of integrated, accessible health care services by clinicians who are accountable for addressing a large majority of personal health care needs, developing a sustained partnership with patients (which connotes the nature of the interpersonal relationship between patients and their health care practitioners), and practicing in the context of family and the community.21
IOM lists the attributes of primary care as accessibility, comprehensiveness, coordination, continuity, and accountability. A number of professional committees and experts have reaffirmed these important characteristics of primary care.12,22,23
For the purpose of this study, we identified questions within the CTS “access to care” component of the Household Survey that measure such principal primary care domains as accessibility and interpersonal relationship. Measures of other primary care domains were inadequate or unavailable from CTS and therefore not represented in the study. Access to care encompasses an array of factors often conceptualized as “potential” and “realized” access, where potential refers to those factors enabling proper receipt of care and realized access refers to actual receipt of services. Here, traditional measures of potential access are available in the CTS and are used in the analytic models. Specifically, we used three questions to address accessibility of primary care: appointment time, waiting time, and travel time. For interpersonal relationship, we identified four questions reflecting patient-physician interactions (ie, thoroughness of care, doctor’s listening, doctor’s explanation, and choice of doctor). Construct validity and selection of the indicators representing the two domains of primary care were performed by the means of principal component factor analysis in earlier studies by the same researchers.9
Overall scores for primary care accessibility and interpersonal relationship were created by summing all primary care indicators within each domain. The primary care accessibility characteristic was measured by a summary score ranging from 0 to 15 and included three items: appointment time, waiting time, and travel time. Appointment time measured how long it took for the respondent to get their last appointment in the following categories: same day, 1 to 7 days, 8 to 15 days, 16 to 30 days, 31+ days. Waiting time measured the time the respondent had to wait in the waiting room before seeing the doctor, measured in the following categories: 0 to 30 minutes, 31 to 60 minutes, 61 to 120 minutes, 121 to 180 minutes, 181+ minutes. Travel time captures the amount of time a respondent spent traveling to the most recent doctor’s appointment, measured in the following categories: 1 to 30 minutes, 31 to 60 minutes, 61 to 120 minutes, 121 to 180 minutes, 181+ minutes.
The primary care interpersonal relationship domain was represented by such items as thoroughness of care, doctor’ listening, doctor’s explanation, and choice of doctor and was summarized in a score ranging from 0 to 20. For thoroughness of care, respondents were asked, “How would you rate the thoroughness and carefulness of care you received?” For doctor’s ability to listen, respondents were asked, “How would you rate how well your doctor listened to you?” Doctor’s ability to explain things was measured by asking respondents, “How would you rate how well your doctor explained things to you?” Respondents answered these questions using a 5-point Likert scale with “excellent,” “very good,” “good,” “fair,” and “poor” response categories. Finally, choice of doctors was captured through the question, “Are you satisfied with choice of primary care doctor?” Response categories included “very satisfied,” “somewhat satisfied,” “neither satisfied nor dissatisfied,” “somewhat dissatisfied,” and “very dissatisfied.”
Self-Rated Health
Two measures of self-rated health were used. As a measure of overall health, respondents’ self-perceived health status was used and coded as 1 for respondents reporting excellent, very good, or good health (herein referred to as good health), and 0 for those reporting fair or poor health (herein referred to as bad health). As a measure of mental health specifically, respondents’ self-perceived state of depression was used and coded as 1 for respondents reporting feeling depressed and 0 for those reporting feeling not depressed. Self-rated health has strong predictive validity for mortality, morbidity, and mental health, independent of other physiologic, behavioral, and psychosocial risk factors.24–27 Although CTS has other measures of health status (eg, SF-12 Physical Health Component Score, SF-12 Mental Health Component Score), these measures were fielded only to adults but are highly intercorrelated with self-perceived health status (0.65) and self-perceived state of depression (0.75).
Vulnerability
Vulnerability status is a self-constructed measure consisting of eight vulnerability status categories identified by a combination of either one of the four race categories (white, black, Hispanic, and other) and a poverty status category (above or below poverty).
Sociodemographic Covariates
Various sociodemographic characteristics known to influence health,28,29 such as sex, age, education, employment status, health insurance, smoking, and usual source of care type of place, were included as control variables into the full multivariate logistic regression model III.
Analysis
The analyses were weighted to represent the civilian noninstitutionalized population of the continental United States. The SUDAAN) software (Research Triangle Institute, Research Triangle Park, NC was used to take into account the complex CTS design, including the clustering of the sample in the 60 communities, the inclusion of multiple families within a household, the sampling of multiple adults within families, and the random selection of one child.30 The estimation procedure took into account the violation of independence among individuals in the same cluster and estimated the appropriate standard errors.
Cross-sectional bivariate analyses of 1996 to 1997 and 1998 to 1999 data were performed to estimate the extent of racial and ethnic disparities in self-rated general and mental health status. Proportions of persons reporting good versus bad health by four racial/ethnic categories (white, black, Hispanic, and other) were analyzed. As a second step, persons from each of the four racial/ethnic groups were stratified into two groups based on their belonging to either above or below poverty category. χ2 tests were performed to assess statistical significance of the associations between the two categorical variables. Furthermore, bivariate relationship between overall primary care scores for two domains, accessibility and interpersonal relationship, and self-assessed general and mental health status were estimated and assessed by t tests.
To study whether primary care plays a mediating role in racial-ethnic disparities in health, three multivariate logistic regression models were estimated. The first model (model I) examined the simple relationship between self-rated general and mental health status as a dichotomous outcome variable, and the eight vulnerability status categories (white below poverty, Hispanic above and below poverty, black above and below poverty, and other above and below poverty) with “white-above poverty” as a reference group. The vulnerability status variables were coded as dummy variables.
The second model (model II) included the two domains of primary care in addition to the vulnerable groups from the first model. The third model (model III, a full model) includes both vulnerability and primary care variables, and also control variables, which include age, education, insurance coverage, smoking status, employment status, and USC type of place (age and employer type not included).
For the three logistic regression models, the odds ratios (OR) and their 95% confidence intervals (CI) are presented in Table 1 (for general health) and Table 2 (for mental health). All the three models were estimated for each of the two cross-sections, 1996 to 1997 and 1998 to 1999. An odds ratio greater than 1 indicates that, compared with the white-above-poverty reference group, the group under observation is associated with an increased odds of reporting bad health versus good health. An odds ratio less than 1 indicates a decreased odds of reporting bad health compared with the reference group (or an increased odds of reporting good health). The extent to which individual experiences of interpersonal relationships with a primary care provider and accessibility to a primary care provider are associated with racial/ethnic disparities, is assessed by the changes of the odds ratios for different vulnerability groups after primary care variables are included into the models.
Multivariate Analysis of Vulnerability, Primary Care Experiences, and Health (Odds Ratio (95% CI))
Multivariate Analysis of Vulnerability, Primary Care, and Mental Health Status (Odds Ratio (95% CI))
Results
Bivariate Analysis
Tables 3 and 4 summarize findings of bi-variate analyses between vulnerability, primary care attributes, and general and mental health status. These findings confirm the presence of significant racial/ethnic disparities in general and mental health status. In 1996 to 1997 fewer Hispanics (78.3%) and blacks (83.1%) compared with whites (89.2%) rated their general health as good, very good, or excellent. The mental health status ratings revealed similar findings, although more Hispanics (75.15%) than blacks (70.31%) rated their mental health as good, very good, or excellent. The degree of disparities in general and mental health status stayed without significant changes in both, 1996 to 1997 and 1998 to 1999.
Bivariate Analysis of Vulnerability, Primary Care, and General Health Status
Bivariate Analysis of Vulnerability, Primary Care Experiences, and Mental Health Status
When stratified by poverty status category, a greater gap between and within racial groups was found. In 1998 to 1999, for the whites, blacks, and Hispanics crossing the poverty line from above to below meant 13%, 11%, and 13% increases in the number of persons rating their general health as fair or poor. These figures did not considerably change in 1998 to 1999 and are comparable with mental health ratings, which confirms presence of persisting racial/ethnic health disparities.
The analysis of bivariate relationship between primary care experiences and health demonstrated significant association between good general health status and higher overall score for both domains of primary care: accessibility (13.25 vs 12.85) and interpersonal relationship (16.72 vs 15.74) (P < .001). Likewise, persons who rated their mental health status as good, very good, or excellent had higher scores, on average, for accessibility (13.13) and interpersonal relationship (16.74) (P < .001).
Multivariate Analysis
Table 1 presents multivariate odds ratios for self-rated general health status for the three multivariate logistic regression models described under Methods. In 1996 to 1997, unadjusted odds ratios (model I) are in line with the bivariate analysis findings, revealing enormous disparity between different vulnerability groups and white-above poverty population. The greatest disparity is seen for minority racial and ethnic groups living in poverty. Overall, the risk of poor general health is greater for the “in poverty” categories than for the “above-poverty”: Hispanics (OR 4.28 vs 2.10), blacks (OR 3.07 vs 1.51), and whites (OR 2.79 vs 1.0) (P < .001).
After primary care domains of accessibility and interpersonal relationship were added into the model (model II), the odds ratios decreased and remained significant for all vulnerability groups, indicating decreased risk of poor health and, therefore, decreased disparities in health status. The odds ratios below 1.0 for accessibility (0.85, P < .001) and interpersonal relationship (0.93, P < .001) indicate negative and statistically significant association between poor health and better primary care. In particular, the odds ratio of 0.85 for accessibility domain means that persons with better primary care access have 15% less chance to be in poor physical health compared with those who had problems accessing their primary care provider.
In the third model, after controlling for other socioeconomic and demographic determinants of health, odds ratios decreased further from 2.89 to 1.61 (P < .001) for black-poverty category, and from 3.09 to 1.58 (P < .001) for Hispanic-poverty group. Association between primary care domains and health in this model remained negative and highly significant (0.92, P < .001), indicating that persons with a better primary care score on average have 8% lower chance to rate their health as fair or poor.
Multivariate analysis for 1998 to 1999 data gave analogous findings indicating persistent racial and ethnic disparities in health status and endorsing the role of primary care as a mediating factor in closing the gap between different racial and socioeconomic groups.
Discussion
The most important contribution of this study is in providing the scientific evidence based on a nationally representative sample that better primary care may reduce racial and ethnic disparities in health status. This study builds on previous research evidence, which pointed to the powerful connections between primary care and health status, further demonstrating that among persons with a primary care physician as a usual source of care, those who experienced better primary care reported better general and mental health status. In this study, better accessibility and interpersonal relationship with primary care provider accounted for a reduction of a risk of poor general health from 3.07 to 2.89 and of poor mental health from 2.8 to 2.71 (P < .001) for blacks in poverty (P < .001). For Hispanics living in poverty, the risk reduction was from 4.28 to 3.09 (P < .001) in general health. These figures indicate closing the health gap between racial/ethnic minorities living in poverty and white population in above poverty category.
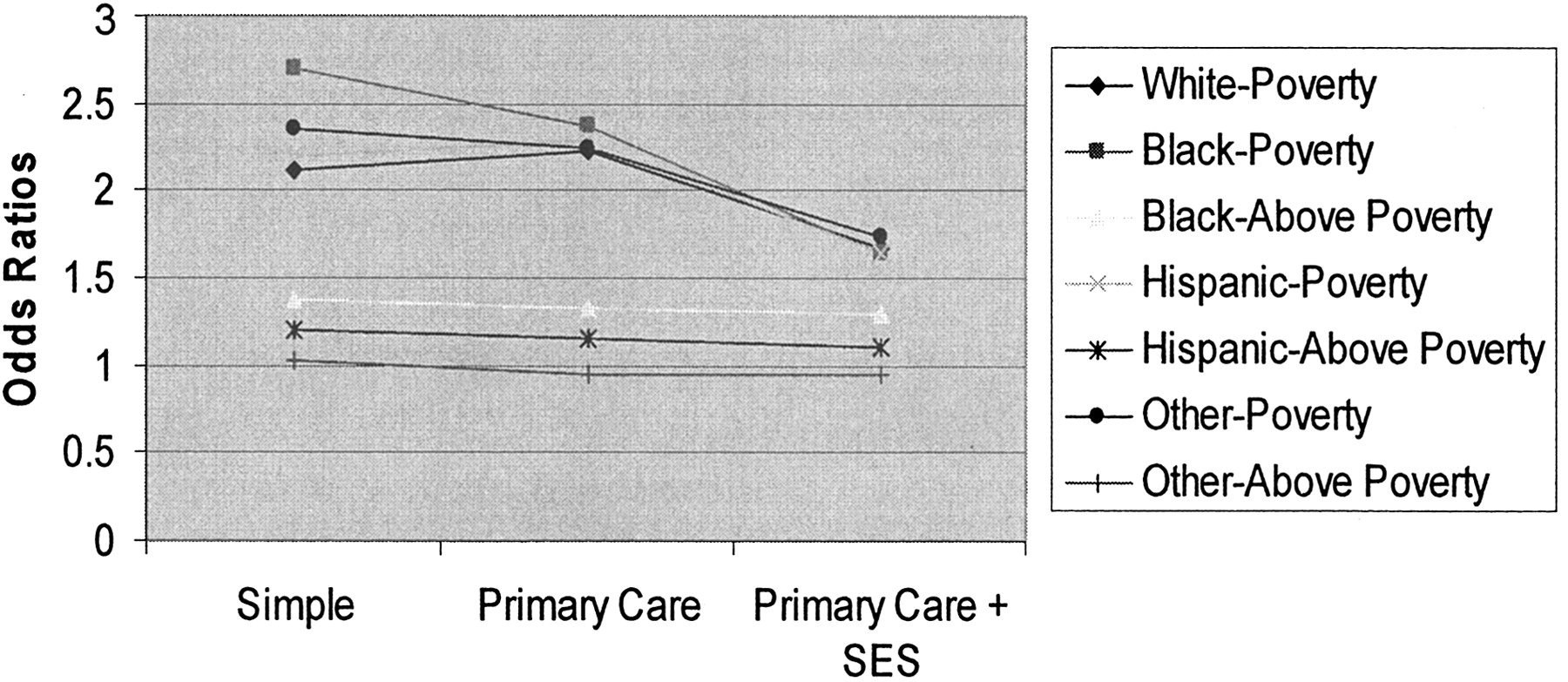
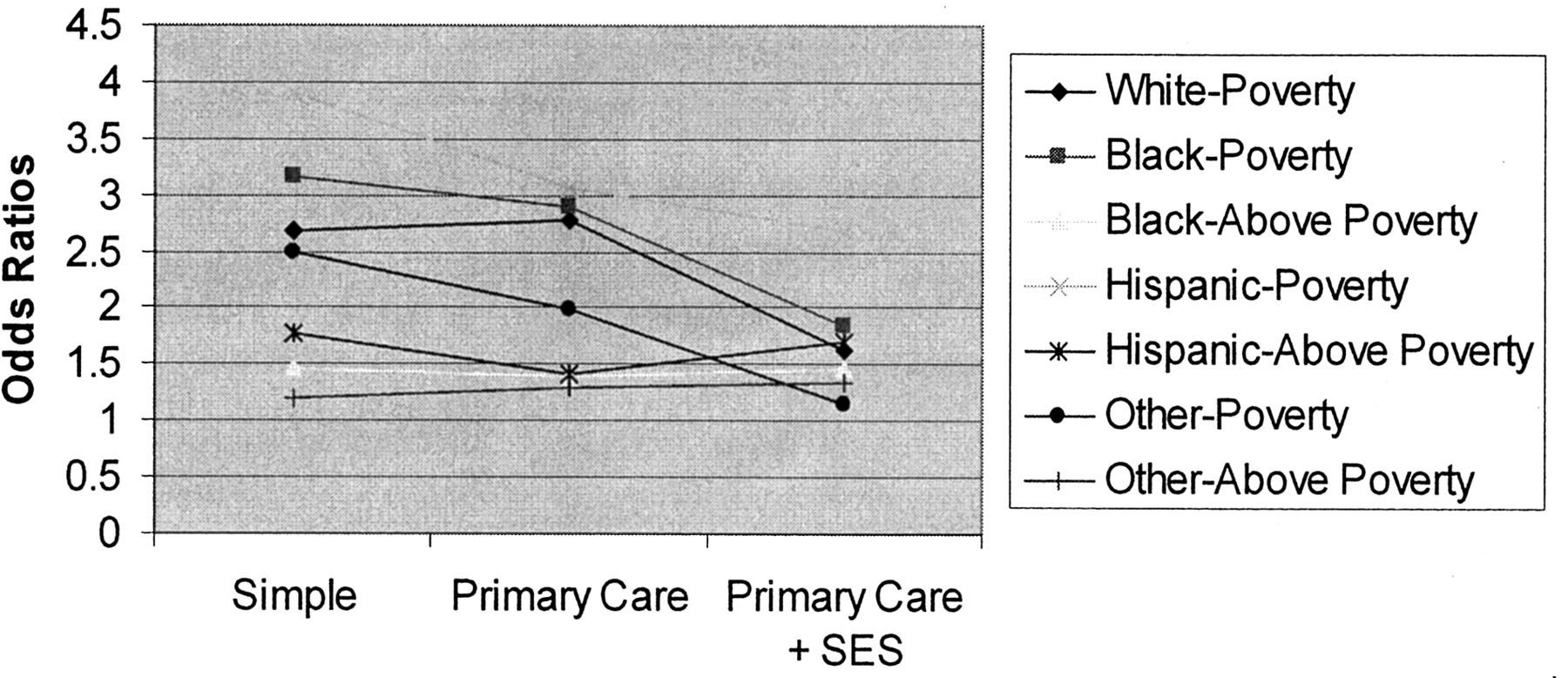
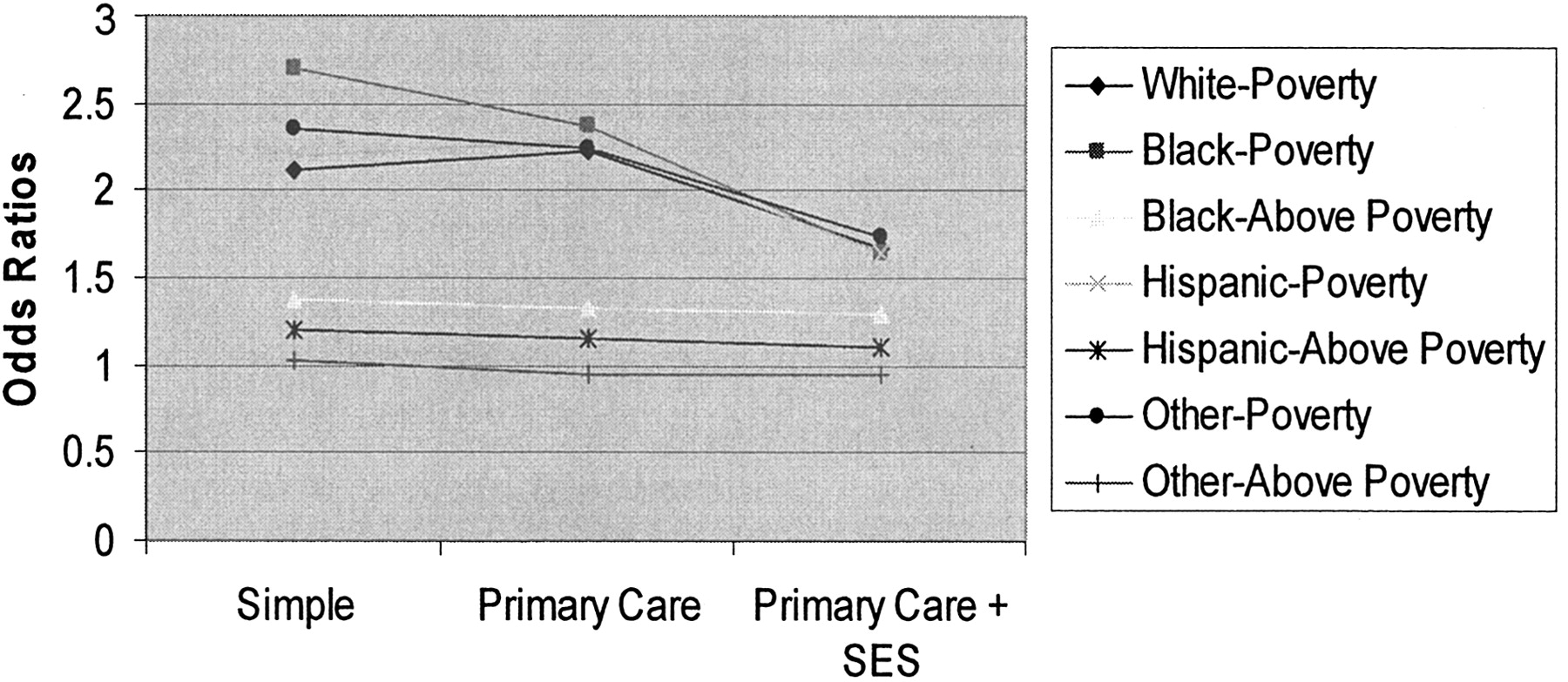
The decrease in the odds ratios and therefore in the risk of poor health, was also evident among Hispanics and blacks living above poverty level. As seen in Figures 1 and 2, which show the general trajectory of poor health risk reduction by primary care, the risk reduction effect is clustered within poverty status—with almost complete elimination of racial/ethnic disparities within the same poverty status category. Controlling for socioeconomic and demographic variables has further decreased the risk of poor health, bringing both in-poverty and above-poverty racial/ethnic groups closer to each other and also to the white-above poverty population group. This is particularly evident in the mental health outcome, where disparities are smaller to begin with.

Health status odds ratios by 3 models (simple, with primary care, and with primary care and socioeconomic status).
Mental health status odds ratios by 3 models (simple, with primary care, and with primary care and socioeconomic status).
The finding that some of the racial disparities in health may be amenable to primary care services calls for nationwide efforts to increase accessibility and quality of primary care, especially for the low-income racial and ethnic minority populations. Because this study sample included only those with usual source of care and because minority race has been linked to a lower likelihood of having a regular source of care, the first step should be to ensure that everyone has access to a primary care provider as a usual source of care.
This study has a number of other important findings. First, the national cross-sectional estimates for the two time periods, 1996 to 1997 and 1998 to 1999, confirmed the presence of persistent racial/ethnic disparities in general and mental health status in the noninstitutionalized population of the United States. Second, this study found gradient relationship between vulnerability status and health. In particular, minority groups living in poverty experience the greatest risk of poor health compared with their “above-poverty” minority counterparts and even more so than white population above the poverty line.
Despite the large nationally representative data sets, this study has a number of potential limitations. First, although the associations we report are strong, they are based on cross-sectional data that preclude determining causal relations between primary care and racial/ethnic disparities. This study, at best, documents the strength of the association between primary care quality and health and between primary care and disparity reduction. It does not parse out whether primary care attributes decrease disparities and does not specify the directionality of the primary care and health relationship. It is possible that those in worse health experience or report poor primary care quality. In separate analyses, not included here, models with vulnerability group-primary care attributes interactions were run to determine whether these factors had a joint, independent effect on health. With the exception of the primary care accessibility-other race category interaction (OR, 0.89; CI, 0.80, 0.99), where accessibility is positively associated with better health among members of the other race category, no other interaction effects were observed and therefore none is included in the analytic models. Further longitudinal studies are needed to ascertain the significant role of primary care in reducing the racial and socioeconomic disparities in health.
Second, the assessment of primary care is based entirely on self-report of receipt of primary care, and we do not know precisely to what extent the observed differences in patients’ assessments of primary care reflect true differences in quality of care. However, we have analyzed other national data sets, such as the Medical Expenditure Panel Survey, that used measures of primary care based on self-report and found significant associations between high quality primary care and better health. Further, this study examines only a subset of the primary care construct. It is possible that the two domains measured here can be the most or least important dimensions in the primary care and health pathway. Some other important domains of primary care, such as comprehensiveness, coordination, and longitudinality, are not captured in the CTS survey.
Finally, although we were able to include Hispanic ethnicity as a variable in our analysis, we were unable to capture other race categories. Existing research evidence suggests that other groups, including Hispanics, Native Americans, and Asian Americans, are also affected.31–34
- Received for publication July 7, 2004.
- Revision received July 7, 2004.




{kind=link}
{kind=link}