
Primary bone cancers are rare and affect fewer than 2500 people yearly in the United States.1 Osteosarcoma, the most common malignant primary bone tumor, has an annual incidence of 2 cases per million people.2 Advances in surgical and medical therapies have dramatically improved the prognosis of osteosarcoma during the last few decades.3 Early detection by primary care physicians remains a cornerstone of treatment, because locally advanced or metastatic disease has a substantially worse prognosis.4 This report describes a recreational athlete who complained of persistent knee pain and was subsequently diagnosed with high-grade tibial osteosarcoma.
Case Report
A 25-year-old recreational runner presented to her family physician for evaluation of chronic right knee pain. The discomfort had been present for 2 months and started after an episode of falling onto her knee. She had struck her flexed knee on cement while avoiding a dog and noted moderate anterior knee pain. She sustained a few superficial abrasions but did not hear a “pop” or recall swelling of the affected knee. She felt no regional weakness or numbness and did not seek care at the time. The pain subsided over the ensuing 3 weeks, and she resumed athletic activities. Five weeks before evaluation, she noticed increasing pain in the anterior right knee that awakened her from sleep and forced her to discontinue running. She noted no catching, locking, or instability of her knee. She denied any fevers, chills, night sweats, or weight loss. No similar symptoms were present in other joints. Her medical history was otherwise unremarkable, and her only medication was ibuprofen. She smoked half a pack of cigarettes daily, used no illicit substances, and had no relevant family history.
Her temperature was 99.1°F on initial examination, and she seemed healthy. Physical examination of her knee revealed no gross deformity, effusion, crepitus, or regional muscle wasting. She was tender over the medial proximal tibia and the anteromedial joint line of her right knee. The knee range-of-motion was 5° to 140°. Strength testing of the right lower extremity was normal, and she had normal peripheral pulses and sensation. Ligamentous and meniscal tests were normal. She walked with a normal gait, and the remainder of her physical examination was normal.
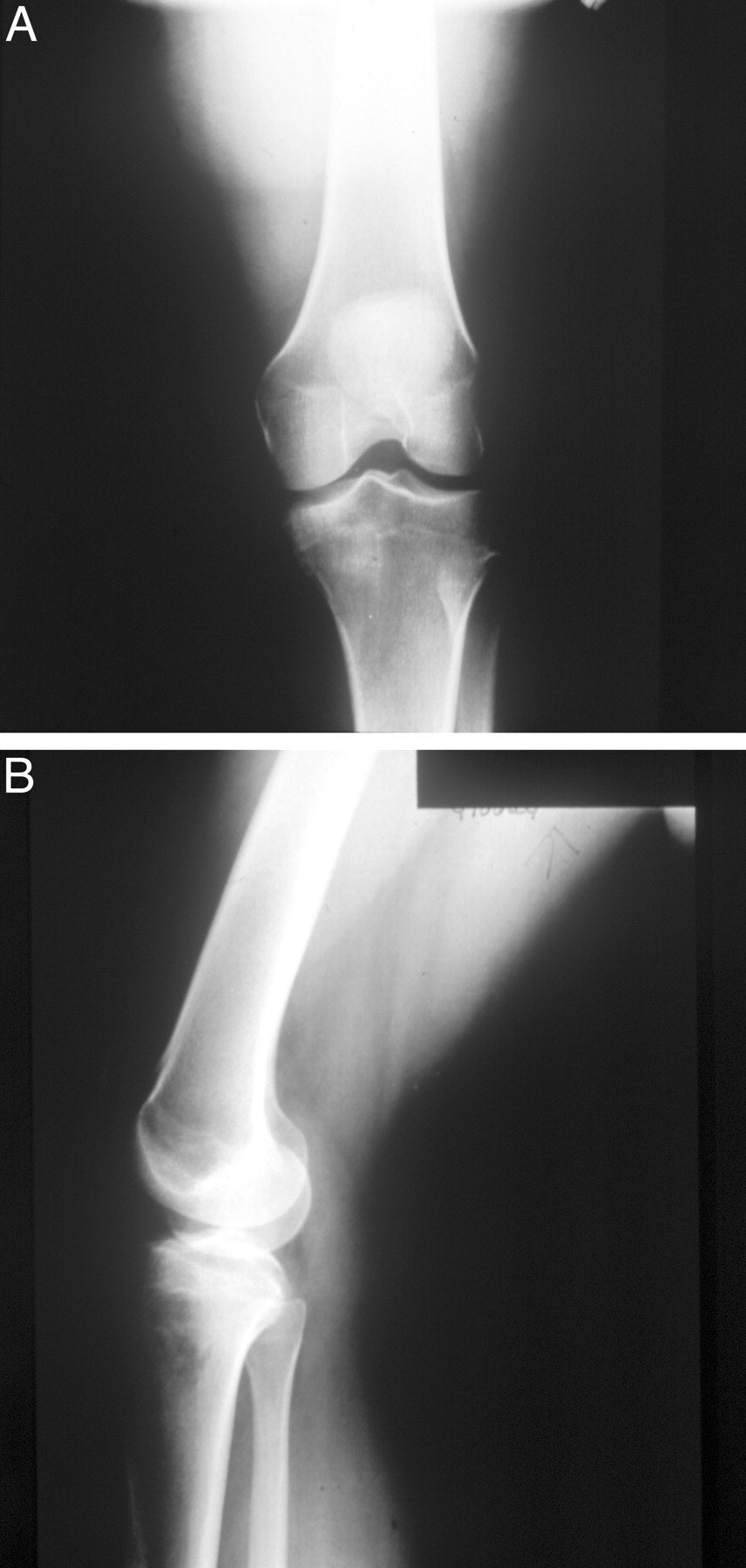
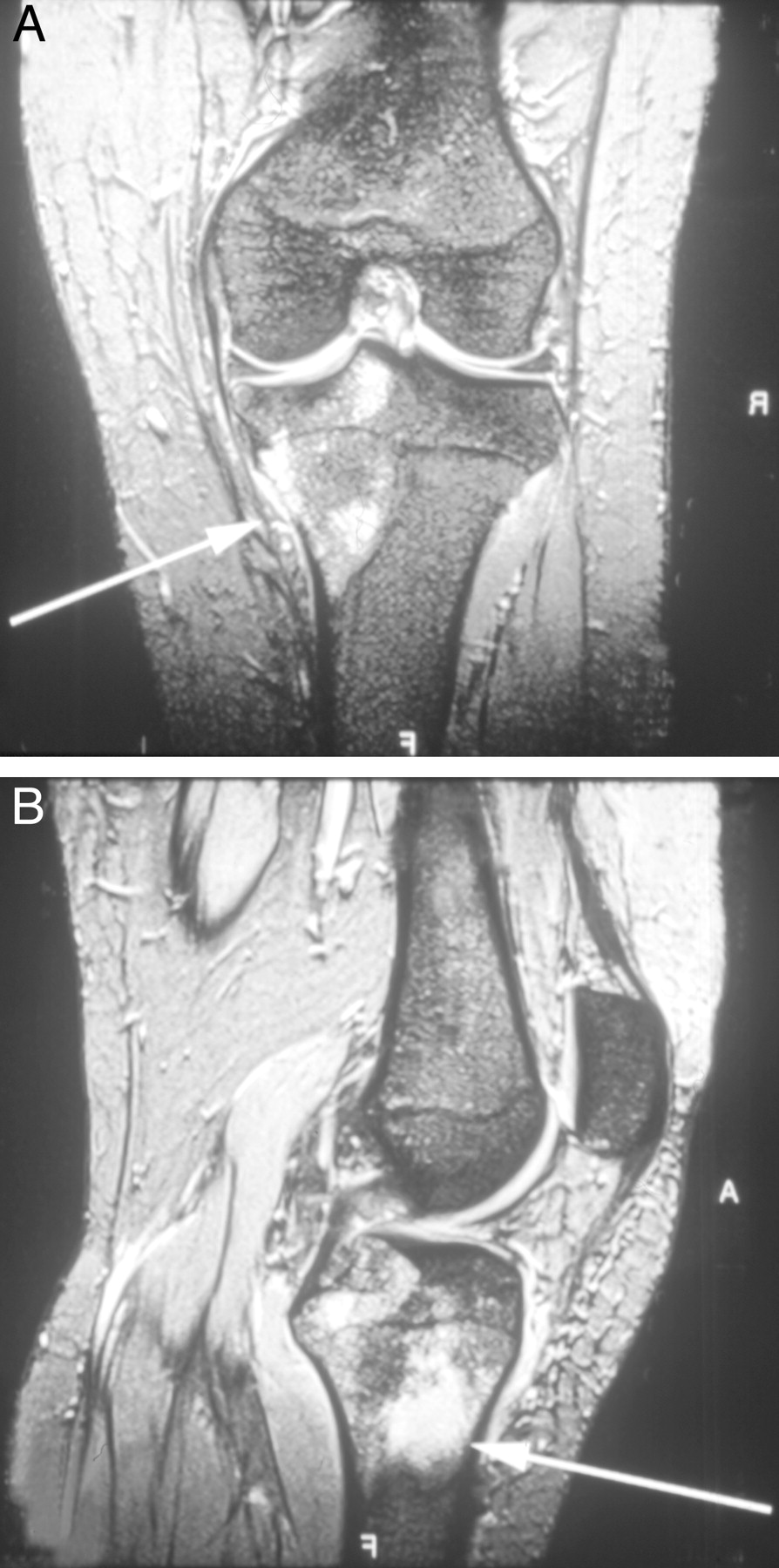
The patient’s atypical symptoms, including progressive discomfort and night pain in association with localized bony tenderness, prompted her family physician to obtain radiographs of her right knee. These radiographs revealed an abnormal bony architecture with a mottled lucency and cortical irregularity affecting the medial tibial plateau (Figure 1). Magnetic resonance imaging (MRI) showed a large (5 cm) focus of pathologic marrow replacement at the medial tibial plateau with disruption of the posterior cortex and extension into the adjacent soft-tissue (Figure 2). A radionuclide bone scan demonstrated increased activity in the medial proximal right tibia, but no other areas of abnormal uptake were noted. The patient’s family physician promptly discussed the case with an orthopedic oncologist who recommended and performed a biopsy of her right tibia that revealed a high-grade osteosarcoma.
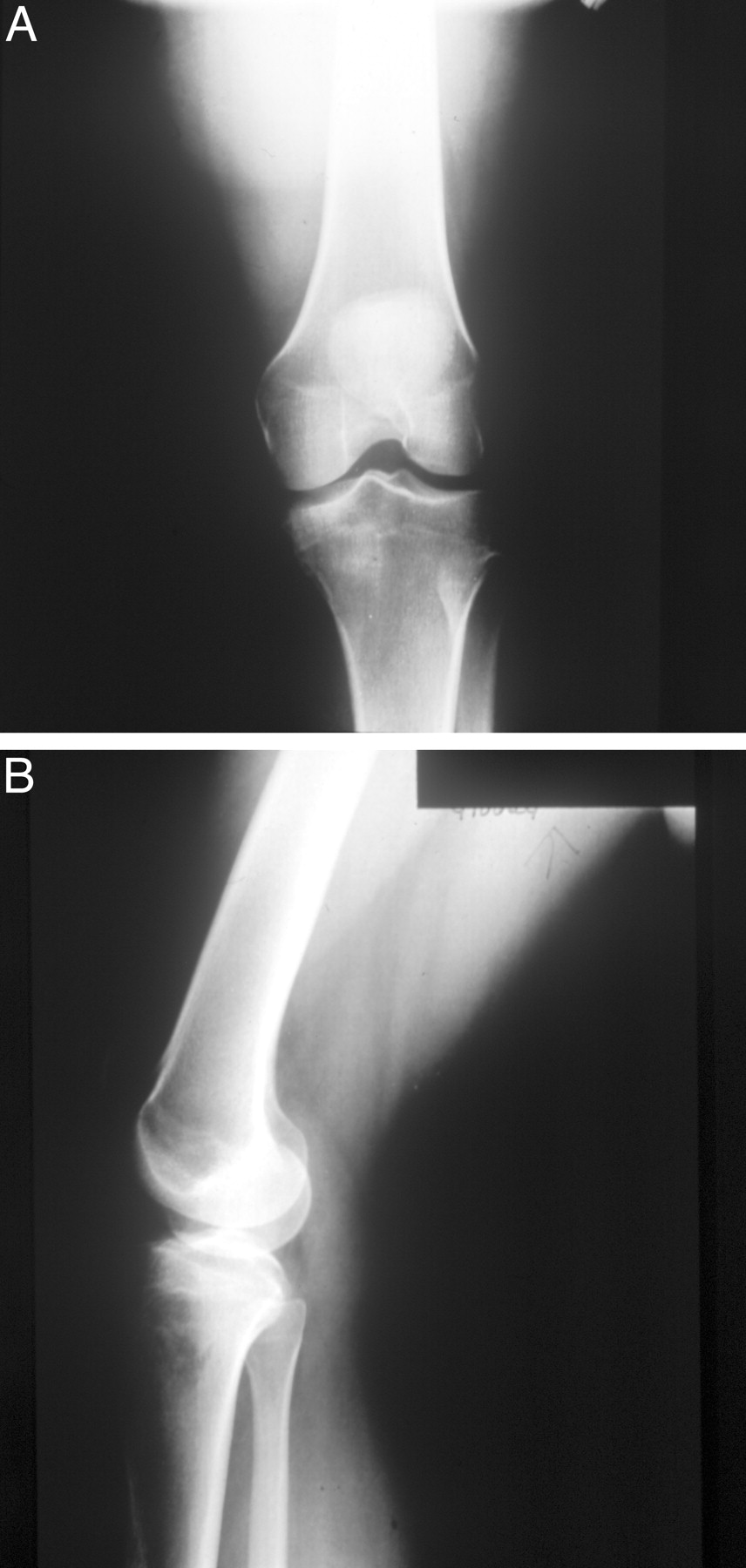
Plain knee radiographs of a 25-year-old recreational runner with chronic right knee pain. The radiographs reveal an abnormal bony architecture with a mottled lucency and cortical irregularity affecting the medial tibial plateau.
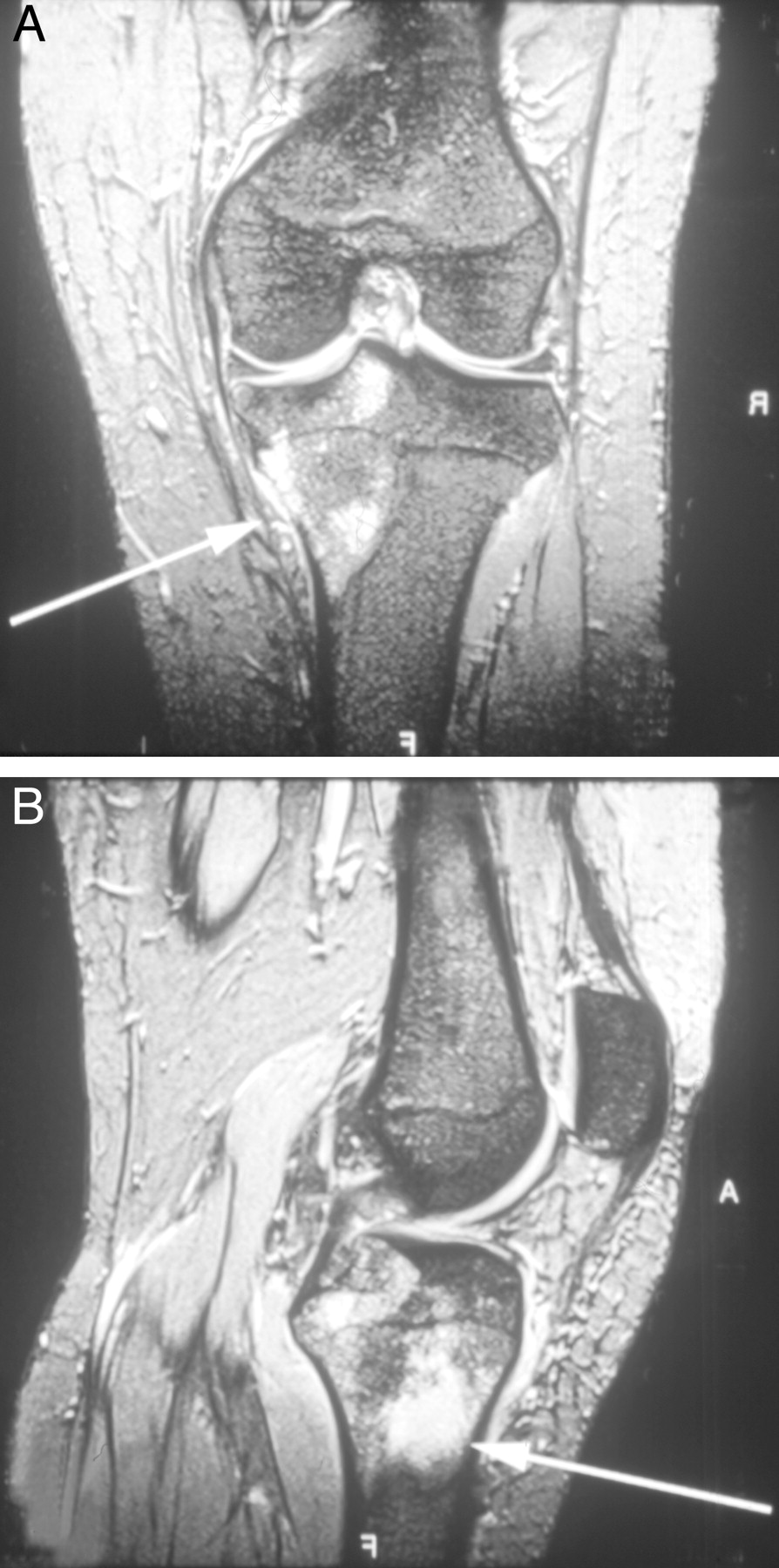
MR images of the patient’s right lower extremity show a large (5 cm) focus of pathologic marrow replacement at the medial tibial plateau with disruption of the posterior cortex and extension into the adjacent soft-tissue (arrows).
Under the direction of a medical oncologist working with the orthopedic and primary care teams, the patient received 3 cycles of preoperative chemotherapy with doxorubicin and cisplatin. Her orthopedic surgeon subsequently performed a wide tibial resection with endoprosthetic reconstruction. After a brief course of physical therapy, she received 2 postoperative cycles of chemotherapy with ifosfamide. She developed burning on the soles of her feet consistent with chemotherapy-induced neuropathy. She returned to her family physician to treat postoperative symptoms of depression and insomnia, but she had no other complications. Extensive testing revealed no recurrent disease 18 months after her initial presentation, and she became pregnant.
Discussion
Although osteosarcoma is relatively uncommon, it accounts for a significant minority of newly diagnosed cancers among children and adolescents. It is the third leading cause of cancer-related death within this population.1,4 Osteosarcoma has a peak incidence in the second decade of life during growth spurts.5 A slight gender predilection is noted, and men are more 1.5 times likely than women to develop osteosarcoma.2,6 Osteosarcoma typically presents at the metaphyseal region of long bones, particularly the distal femur, proximal tibia, and proximal humerus.3,7 The majority of osteosarcoma tumors begin as primary lesions, although some arise from a prior malignancy.8 The natural history and progression of osteosarcoma is variable. Typically, fewer than 60% of high-grade tumors undergo spontaneous necrosis by outgrowing their blood supplies.9 Most cases consist of localized extremity tumors at the time of diagnosis. Fewer than 20% of patients present with identified metastatic disease, although most have subclinical micrometastatic disease.5,8
Diagnosing an osteosarcoma can be challenging for both primary care physicians and specialists, because the symptoms can frequently be subtle or misleading. Regional pain, decreased range of motion, or a palpable mass are the most common presenting complaints.4,7 Some patients have few symptoms except for mild, intermittent discomfort that has waxed and waned for several months. Night pain, fevers, and weight loss are uncommon.3 In one study, 47% of the patients with osteosarcoma related the onset of pain to regional trauma occurring shortly before the onset of symptoms.2 Because osteosarcoma typically affects young, healthy persons, the likelihood of reporting symptoms of a coincident activity-related disorder is relatively high. Consequently, a patient with an osteosarcoma may describe symptoms consistent with a muscle strain, tendinitis, or other benign condition. Thus, primary care physicians need to maintain a high index of suspicion when talking to active persons with localized extremity pain.
Like the symptoms of osteosarcoma, physical examination findings are nonspecific and inconsistent. As a result, fewer than one third of patients with osteosarcoma initially receive the correct diagnosis.2 Localized tenderness is the most common physical finding. Additional important clinical features of osteosarcoma include fever, a palpable mass, painful or restricted range of motion of the affected extremity, limping, or regional muscle atrophy. Local or distant lymphadenopathy is an uncommon finding.2,10
Accurately diagnosing knee osteosarcoma at an early stage is often difficult, for the differential diagnoses of anterior or medial knee pain are broad and osteosarcoma is uncommon. Tables 1 and 2 list the common differential diagnoses of localized anterior or medial knee pain, the typical clinical findings, and the recommended diagnostic tests to evaluate the various conditions. Several different bone tumors may affect the knee joint. Table 3 lists the most common benign and malignant bone tumors, including their peak ages of onset, typical locations, clinical findings, and prognoses. An important point to note is that osteosarcoma is uncommon in patients older than 20 years old, making this tumor very unusual for a 25-year-old person.
Differential Diagnosis of Localized Anterior Knee Pain
Differential Diagnosis of Localized Medial Knee Pain
Differential Diagnosis of Benign and Malignant Bone Tumors
Evaluating a suspected osteosarcoma may require a primary care physician to consider several diagnostic studies. Serologic tests are typically not helpful, but alkaline phosphatase or lactate dehydrogenase may be elevated in 30% to 40% of patients with osteosarcoma.10 The patient discussed in this case report had symptoms consistent with anterior knee pain syndrome, which is the most common knee disorder in this age group and does not typically require radiographs. However, plain radiographs of the entire affected bone should be the initial study of choice if warning symptoms occur (fevers, night sweats, night pain, or unexplained weight loss) in association with knee pain.4 Indeed, promptly obtaining radiographs pointed the family physician toward the correct diagnosis in this case. Radiographs have the advantage of being convenient, inexpensive, and reproducible. Radiographs will be abnormal in the majority of cases, with osteosarcoma appearing as a lytic and/or sclerotic lesion in a long bone metaphysis.3,7 Radiographs are often good predictors of histologic diagnosis but frequently underestimate the tumor extent.11
Triple-phase bone scintigraphy is a useful adjunct for evaluation of a suspected osteosarcoma.9 Bone scans are helpful in gauging the extent of the primary tumor and are more sensitive than plain radiographs for the detection of bony metastases.5 Scintigraphy has the advantage of allowing visualization of the entire skeleton, but bone scans may miss “skip lesions” in the affected bone (additional medullary disease within the same bone as the primary tumor but not in direct continuity).3 Thallium scintigraphy has been be used to predict the tumor’s response to neoadjuvant chemotherapy, and a tumor necrosis of less than 90% indicates a poor response.11 Bone scans are also used to monitor for disease recurrence.
Magnetic resonance imaging (MRI) and computed tomography (CT) are superior to plain radiography for evaluation of osteosarcoma.3 Both MRI and CT can determine the presence of regional soft-tissue invasion and assist with planning a limb-salvage procedure.11,12 MRI is highly sensitive for identifying osteosarcoma and has largely replaced CT for this purpose.8 MRI can also determine the extent of disease, involvement of surrounding neurovascular structures, and presence of skip lesions.3,13 CT is a superior way to evaluate the cortical integrity of the affected bone and can delineate the tumor extent.5 The majority of osteosarcoma metastases occur in the lungs, and CT is the study of choice to identify pulmonary metastases that are undetectable on 20% of chest radiographs.3,10
A bone biopsy is a critical step in the diagnosis and management of osteosarcoma.13,14 A biopsy under CT or fluoroscopic guidance can distinguish osteosarcoma from other neoplasia or benign conditions with 90% accuracy.13 Biopsy technique is critical, and a trained tumor surgeon who is careful not to compromise the area of subsequent surgical resection should perform the biopsy.10 Improperly performed biopsies may be a cause of misdiagnosis or inappropriate therapy.5
Treatment should be initiated shortly after the biopsy and staging studies have confirmed the diagnosis and extent of osteosarcoma.10 Chemotherapy is essential for most patients with osteosarcoma, because hematogenous spread of micrometastases occurs very early in the disease process.4,14 The long-term survival rates of patients with osteosarcoma have dramatically improved during the last few decades, primarily as a result of enhanced chemotherapeutic regimens.2,7,15,16 Before the routine use of multiagent chemotherapy, 5-year osteosarcoma survival rates were less than 15%.3,6 The survival rate has recently escalated to 60% to 80% with the combination of chemotherapy and surgery.3,4,14,17 That the long-term survival rates for osteosarcoma have dramatically improved with modern treatment regimens should be emphasized by primary care physicians when counseling patients about osteosarcoma prognosis.
Modern chemotherapeutic regimens are given both before surgery (neoadjuvant) and after (adjuvant). A variety of researchers have confirmed that neoadjuvant chemotherapy significantly improves osteosarcoma survival, especially among children and adolescents.3,8,15,18 The fibrosis and tumor shrinkage that occurs after neoadjuvant chemotherapy may also facilitate surgical removal of the primary tumor.3 In addition, neoadjuvant therapy provides time to prepare custom prostheses for limb-salvage procedures, treat micrometastases empirically, and minimize pulmonary metastases.5,18,19
Doxorubicin, cisplatin, ifosfamide, etoposide, and high-dose methotrexate are the most commonly used chemotherapeutic agents.3 Patients are typically treated with multiagent regimens, although regimens of fewer drugs may be equally efficacious and better tolerated.17,20,21 The degree of necrosis after neoadjuvant chemotherapy is the most important prognostic factor for osteosarcoma and may be used to tailor the adjuvant regimen.7,17,19,22 Chemotherapy presents many potential risks, and some researchers believe that multiagent, aggressive chemotherapeutic regimens increase toxicity without improving survival.18,20,21 Potential chemotherapeutic side effects include cardiomyopathy, emesis, alopecia, peripheral neuropathy, ototoxicity, neutropenia, leukopenia, and nephrotoxicity. In addition, a second malignancy, such as leukemia, may occur as a long-term complication of systemic chemotherapy.8
Despite the importance of chemotherapy in the modern treatment of osteosarcoma, surgical removal of the primary tumor and all visible metastases remains essential to minimize the risk of recurrence.4,10,15,18 Surgery by itself, however, is inadequate for most patients because of micrometastases or unrecognized skip lesions, and more than 80% of patients treated solely with surgery will develop recurrent disease.3,15,19
Osteosarcoma of the extremity has traditionally been treated with limb amputation.10 Recently, wide-local resection combined with limb salvage has become a preferable alternative to amputation for most patients.6,23–25 Limb-salvage reconstruction uses metallic implants (endoprostheses), autografts, or cadaveric allografts to replace the excised bones or joints.3 No evidence suggests a significant difference in the long-term survival rate between limb amputation and limb-salvage surgery for extremity osteosarcoma.23,26,27 Advantages of limb-salvage surgery include improved psychological, cosmetic, and functional outcomes with similar disease-free intervals compared with amputation.26,27 Disadvantages of limb-salvage surgery include higher rates of reoperation and the potential need for subsequent amputations.23 Allografts used in the procedure may also present risks of infection or transmission of viral diseases.28
Radiotherapy is of limited value in treating osteosarcoma, but radiation therapy may be helpful for palliation of nonresectable tumors.3,4,16 Intraoperative radiation therapy in conjunction with surgical excision has also been used for locally advanced tumors.28 Current research has not confirmed the value of prophylactic lung radiation for pulmonary metastatic disease.16,22
When counseling patients with osteosarcoma, primary care physicians need to be cognizant of osteosarcoma prognosis. As noted, the long-term survival of patients with osteosarcoma has dramatically improved, but several factors may influence the overall prognosis. An important factor affecting prognosis is the presence of metastases. Of patients with clinically detectable metastases, only 20% to 40% will successfully be cured, versus 60% to 80% without metastases.10 Because patients with metastatic disease at diagnosis have significantly worse prognoses than those with localized osteosarcoma, primary care physicians can significantly improve patient outcomes by quickly diagnosing and referring patients with osteosarcoma.3,4 Additional factors associated with a worse prognosis include an axial primary tumor location, bony metastases, increased lactate dehydrogenase levels, and a larger tumor volume.3,19,26 Patients with a greater degree of tumor necrosis after neoadjuvant chemotherapy or those with osteosarcoma of the tibia or fibula have more favorable long-term prognoses.3,7,17,19
With current medical and surgical therapy, the long-term survival for patients with osteosarcoma has dramatically improved, but 30% to 40% of patients will develop recurrent disease.10 Local recurrences affect only 5% to 10% of patients, and the majority of recurrences arise in the lungs.3,6,22,25 Additional surgery or chemotherapy can be considered for patients with recurrent disease, but most will develop additional disease. Ultimately, cure rates of only 10% to 20% should be expected for recurrent osteosarcoma, and distant metastases are the most common cause of eventual death.3,10,25 Patients without evidence of recurrence within the first 3 years after diagnosis are likely to be cured.15
Patients with successfully treated osteosarcoma should be monitored for at least 5 years by their primary care physicians or surgeons. Chest CT scans every 4 to 6 months and bone scans every 12 months for the first 2 years are recommended to detect recurrent disease.5 Psychosocial supports are often needed during the course of therapy. Coordinating care among medical staff, social workers, psychologists, and family members may improve the patient’s ultimate functional status.10
Conclusion
Osteosarcoma is the most common malignant primary bone tumor and has a peak incidence in the second decade of life. A high-degree of clinical suspicion by primary care physicians is essential to diagnose this uncommon cancer. Although many researchers have demonstrated that physically active persons have lower rates of serious illness and mortality compared with sedentary populations, any person with an atypical clinical musculoskeletal presentation must be suspected of having a serious underlying disease regardless of his or her overall health status. Localized tenderness, a palpable mass, restricted range of motion, limping, and muscle atrophy are the most common clinical findings. Plain radiography, MRI, CT, bone scanning, and surgical biopsy are helpful to evaluate osteosarcoma. Treatment involves surgical excision of local and metastatic disease combined with multiagent chemotherapy. With prompt recognition and early therapy, many persons with osteosarcoma have very favorable prognoses.
- Received for publication December 20, 2002.
- Revision received December 20, 2002.
References




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.