
Article Figures & Data
Figures
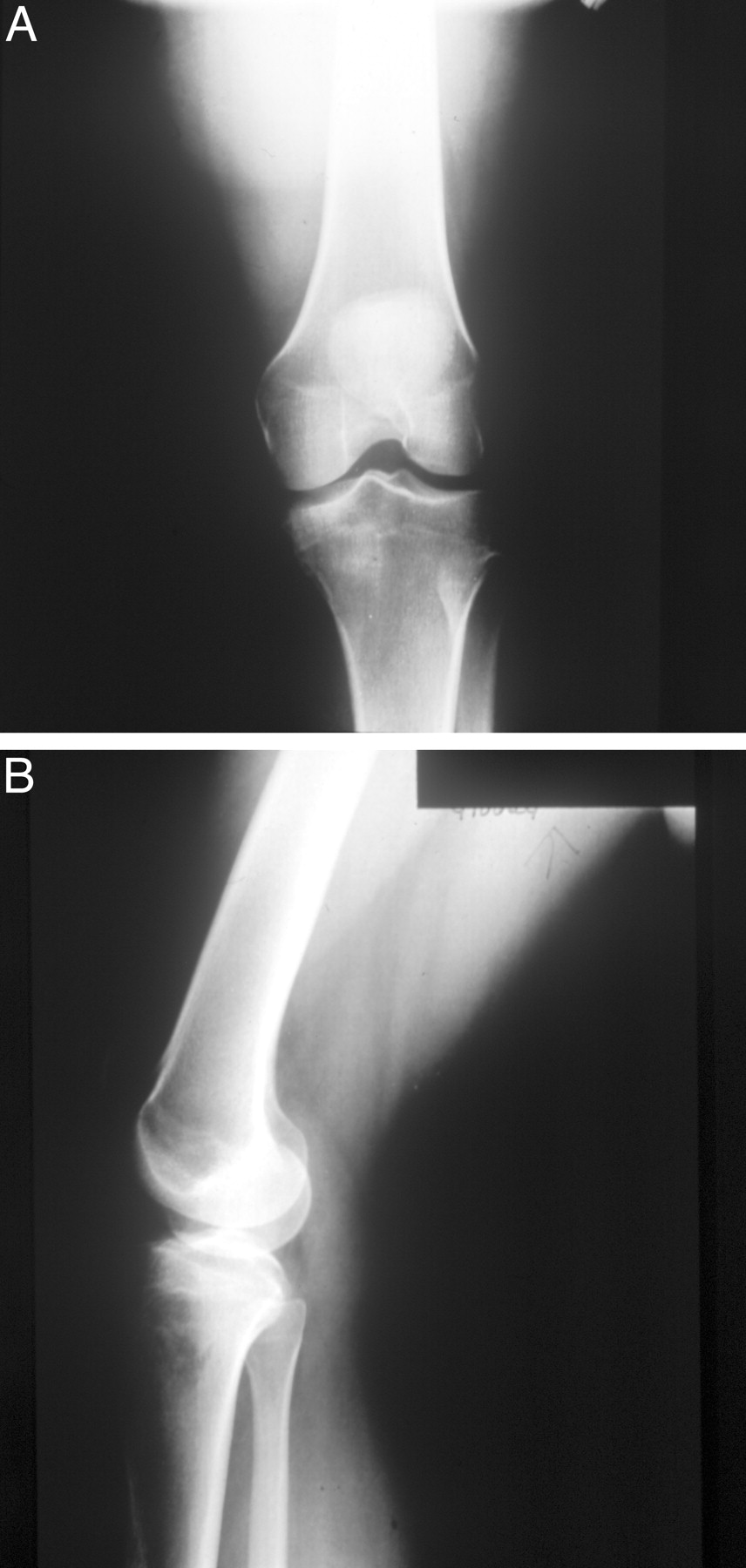
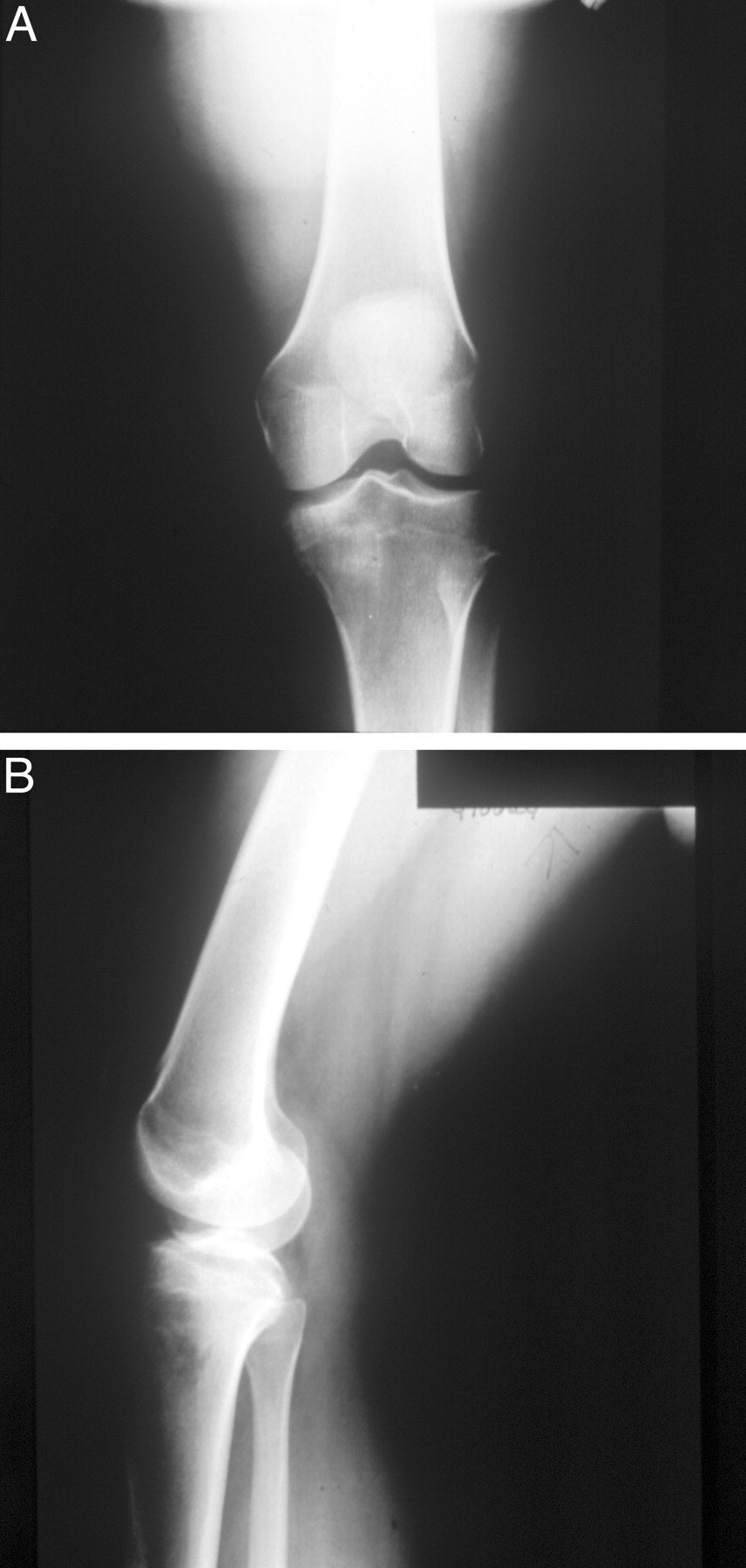
- Figure 1.
Plain knee radiographs of a 25-year-old recreational runner with chronic right knee pain. The radiographs reveal an abnormal bony architecture with a mottled lucency and cortical irregularity affecting the medial tibial plateau.
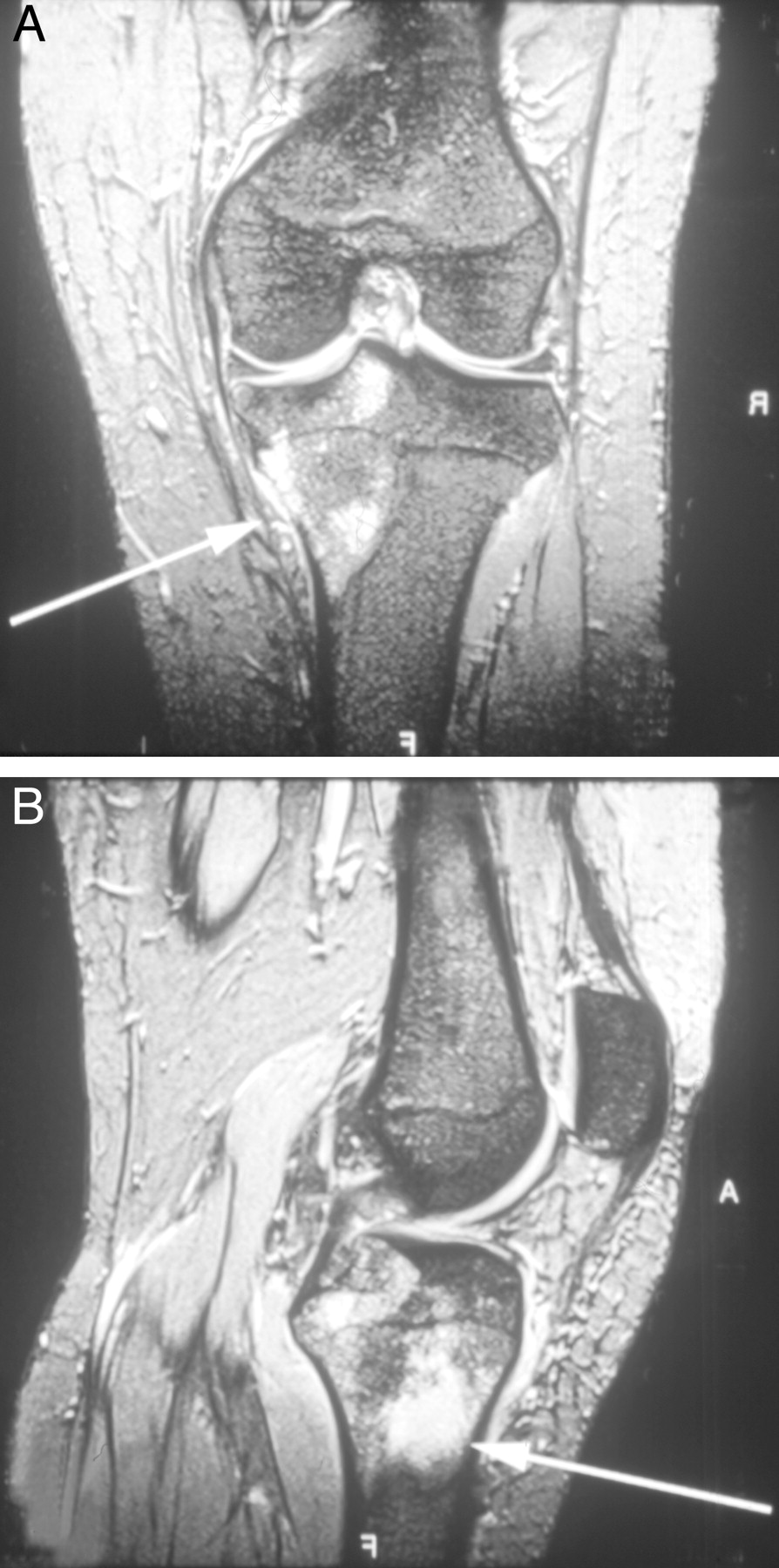
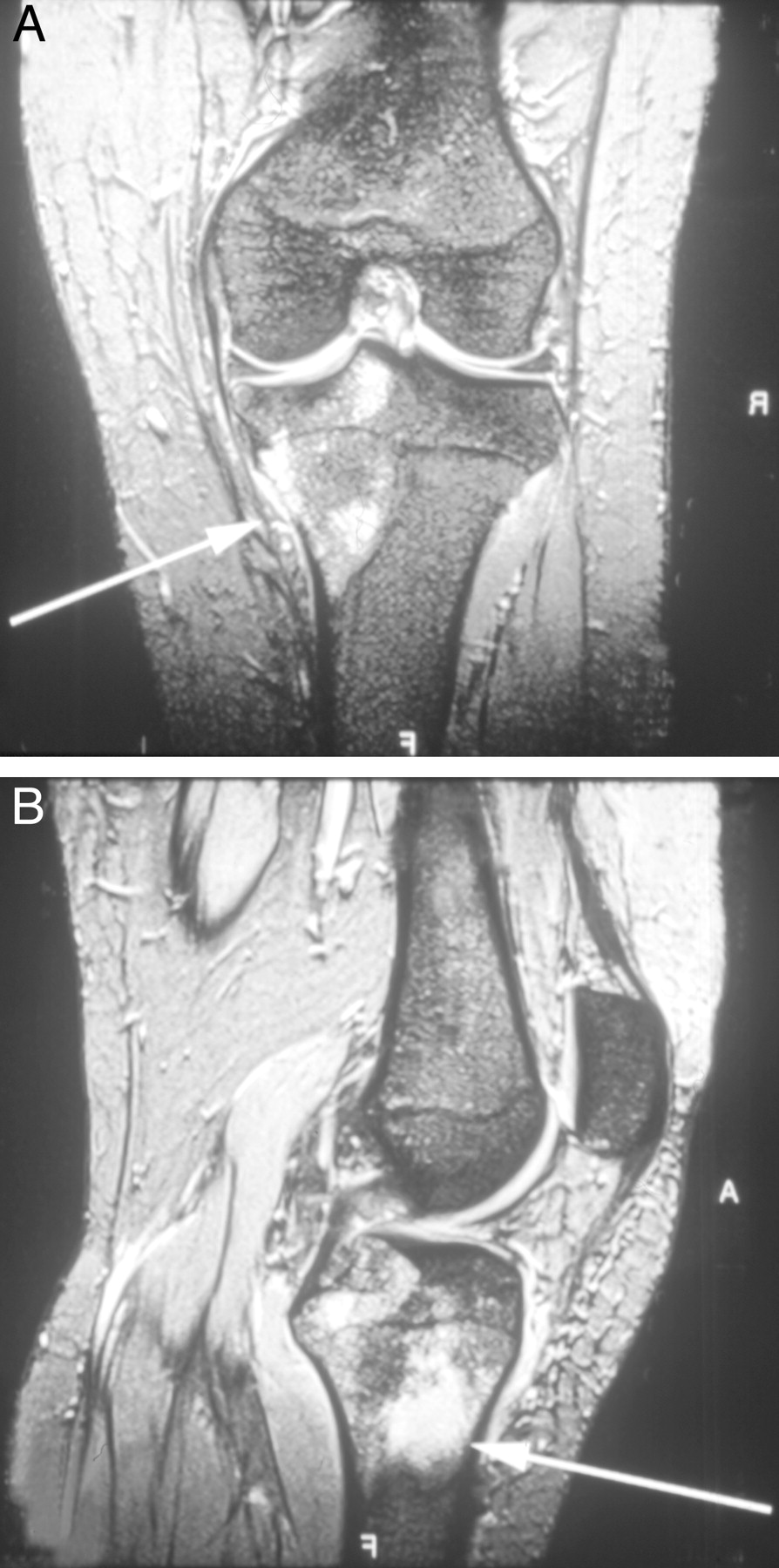
- Figure 2.
MR images of the patient’s right lower extremity show a large (5 cm) focus of pathologic marrow replacement at the medial tibial plateau with disruption of the posterior cortex and extension into the adjacent soft-tissue (arrows).
Tables
Condition Typical Findings Diagnostic Testing Bipartite or multipartite patella Usually asymptomatic Radiographs, including contralateral for comparison Infrapatellar fat pad syndrome (Hoffa syndrome) Tenderness below inferior patellar pole, worse with resisted knee extension Rarely indicated Osgood-Schlatter disease Localized tibial tubercle tenderness in an adolescent or young adult Radiographs, compare with contralateral knee Patellar fracture Localized patellar tenderness or swelling over the anterior knee Radiographs, including contralateral to rule out multipartite patella Patellar subluxation/dislocation Apprehension with lateral patellar pressure, abnormal medial/lateral patellar glide Radiographs if conservative therapy fails or patella is nonreducible Patellar tendonitis (jumper’s knee) Localized patellar tendon tenderness, worse with resisted knee extension Rarely, consider MRI for chronic symptoms Patellofemoral pain syndrome (Anterior knee pain syndrome) Tenderness over patellar body or facets; abnormal patellar tracking, medial/lateral glide, or tilt; increased Q-angle* Radiographs uncommon; consider if conservative therapy fails Prepatellar bursitis (housemaid’s knee) Tenderness, erythema, or superficial swelling over patella Rarely indicated Sinding-Larsen-Johansson disease Localized inferior patellar pole tenderness in an adolescent or young adult Radiographs, compare with contralateral knee Tumor Insidious pain, swelling, or mass over anterior knee; night pain or systemic symptoms Radiographs; consider MRI or bone scan if radiographs are negative and clinical suspicion is high * Q-angle: An approximate measure of patellofemoral alignment. The angle is formed by the intersection of a line from the anterior superior iliac spine to the center of the patella and a line from the tibial tubercle to the center of the patella. A normal q-angle is less than 10° in men and 15° in women.
Condition Typical Findings Diagnostic Testing Hamstring tendonitis Localized tenderness or swelling over medial hamstring tendon insertion Rarely indicated Medial collateral ligament tear Laxity or regional pain with valgus stress testing; effusion rare Radiographs or MRI Medial plica syndrome Tenderness near medial patellar retinaculum that worsens with knee flexion Radiographs if symptoms are atypical or persistent Meniscal tear Tenderness over medial joint line; positive McMurray test*; effusion possible >12 hours after injury MRI or arthroscopy Osteoarthritis Regional medial knee or joint line tenderness; effusion and decreased range-of-motion possible Radiographs Osteochondritis dissecans Decreased range of motion or mild weakness; joint line tenderness or effusion possible; occasional catching or locking Radiographs; consider arthroscopy, MRI or CT Pes anserine bursitis Tenderness 2 to 4 cm below medial knee joint line Rarely indicated Tibial plateau fracture Localized or diffuse superior tibial tenderness; effusion possible Radiographs; consider MRI or CT Tibial stress fracture Localized or diffuse superior tibial pain Radiographs; consider MRI or bone scan if radiographs are negative Tumor Insidious pain, swelling, or mass over medial knee; night pain or systemic symptoms may occur Radiographs; consider MRI or bone scan if radiographs are negative and high clinical suspicion * McMurray test: (1) Position patient supine and flex affected knee. (2) Steady the knee with one hand and grasp the ipsilateral heel with the other. (3) Palpate the medial and lateral joint lines. (4) Rotate the ipsilateral foot externally to test the medial meniscus and internally to test the lateral meniscus. (5) A snap felt over the joint line while extending the knee signifies a positive test.
Disease Peak Age (years) Typical Location Findings Prognosis Chondroblastoma 10–20 Long bone epiphyses Regional muscle atrophy and localized tenderness; radiographic appearance of a cyst containing calcium deposits Good Chondroma >20 Central diaphyses Usually asymptomatic;radiographs show stippled calcification Good Chondromyxoid fibroma <30 Distal long bones Sharply circumscribed, lytic lesion on radiographs Good Chondrosarcoma 30–50 Flat bones, long bone diaphyses Lobular radiographic appearance with punctate calcification Fair with surgical resection but resistant to chemotherapy Ewing’s Sarcoma 10–18 Long bone diaphyses and flat bones Localized pain or swelling; `onion peel` periosteal reaction on radiographs Good if nonmetastatic, poor if metastatic Giant cell tumor <2, >24 Epiphyses Lytic appearance on radiographs Good; tendency to recur Osteochondroma 5–15 Distal femur, proximal tibia Painless, hard palpable mass; most common benign bone tumor Good; 10% with multiple lesions develop a malignancy Osteoid osteoma 5–20 Femur, tibia Nocturnal pain relieved by aspirin Good Osteosarcoma 10–18 Long bone metaphyses Localized pain or swelling; sclerotic or lytic destruction on radiographs Good if nonmetastatic; poor if metastatic




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.