
Abstract
Background: Transitional Care Management (TCM) is a reimbursable service designed to minimize hospital readmissions. We describe a multifaceted approach to increase TCM services among 107 primary care providers in a rural catchment area of 4250 square miles.
Objective: The primary objective was to increase use of TCM phone calls, office visits, and billing codes; the secondary objective was to decrease hospital readmissions.
Methods: We utilized a learning health system model, an improvement support team (IST), and a learning collaborative that included webinars and in-person support. The process emphasized user-centered system redesign, coaching, electronic health record (EHR) improvements, and real-time feedback. Analyses included statistical process control charts, box plots, analysis of variance, and t-tests.
Results: The IST engaged stakeholders to design and test TCM workflows and EHR prototypes. This resulted in rapid, iterative improvements and system-wide spread of new processes. In the month following implementation, TCM calls and visits quadrupled and increased during 18 subsequent months. Pragmatically, most discharged patients (95% in a subsample) did not receive both the TCM call and visit, serving as a comparison group. The Readmission rate for patients receiving complete TCM services was 5.0% (n = 101) versus 11.9% for comparators (n = 2103, P = .03). Billing codes increased initially, then returned to baseline.
Conclusions: Our approach led to rapid, sustained scaling of TCM calls and visits in a rural primary care group. Patients who received TCM calls and visits had significantly fewer readmissions. Training of new staff, including PCPs, is required for sustainability. Future research is warranted to increase adoption and evaluate additional outcomes including mortality rates, patient satisfaction, and health care economics.
- Analysis of Variance
- Electronic Health Records
- Information Systems
- Learning Health System
- Patient Readmission
- Quality Improvement
- Rural Health
- Transitional Care
- Workflow
Introduction
Problem Description
Hospital readmissions are common, leading to a significant burden for patients and health care systems. Transitional Care Management (TCM) is a care pathway to prevent readmission.1,2 Most payers, including Centers for Medicare and Medicaid Services (CMS), reimburse providers for TCM services at a higher rate than standard office visits to cover the additional care coordination. Providers may use a TCM billing code once during the 30 days following a hospital discharge. Within Dartmouth Health, there was previously no way for leadership to track which clinics were completing TCM activities. Furthermore, primary care provider (PCP) use of TCM billing codes was much lower than expected. Primary Care Service Line (PCSL) leaders targeted TCM for improvement based on expected benefits to patient (fewer readmissions) and organizational finances (fee-for-service revenue, savings in risk-based contracts).
Background
Rationale
Increased use of TCM utilization (phone calls and office visits) is likely to improve continuity of care post hospital discharge, thereby addressing risks for readmission early in the outpatient setting. Therefore, we expect to see use of TCM services inversely correlated with hospital readmission rates.
Readmissions and TCM
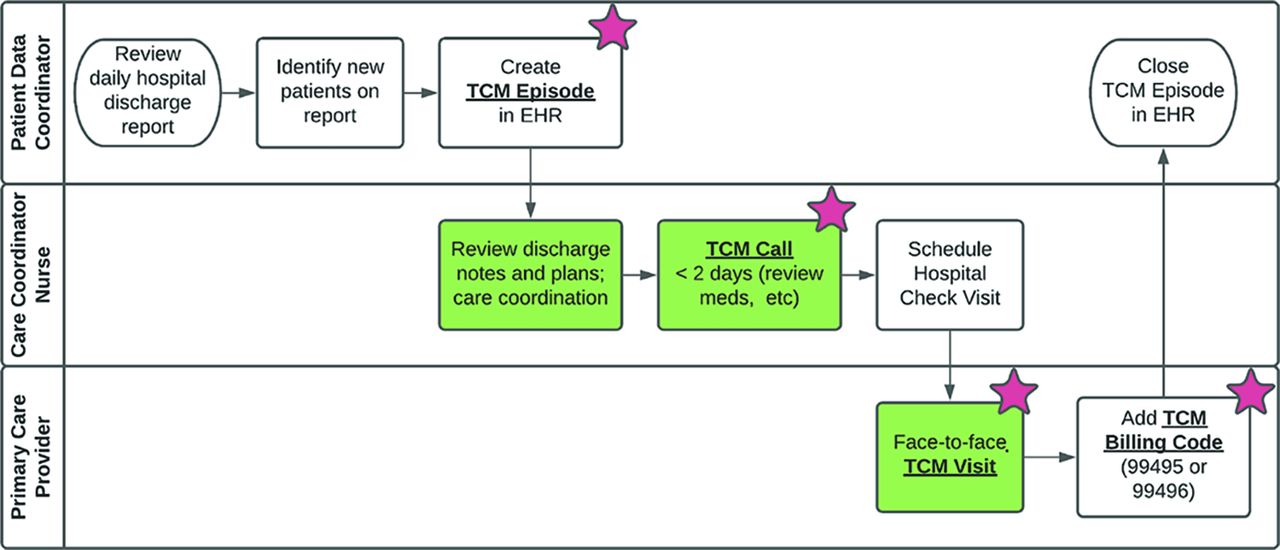
Approximately 20% of Medicare patients transitioning from hospital to outpatient care are readmitted within 30 days, costing ∼$17 billion annually.3 Health care systems have applied various models to decrease readmission, including TCM. CMS implemented TCM billing codes to incentivize the adoption, first in 2013 and with higher reimbursement in 2020.4 Billing requirements include 3 TCM components: (1) nonface-to-face services (e.g., record review, care coordination), (2) interactive contact (typically a phone call) within 2 business days of discharge, and (3) office or telehealth face-to-face visit within 7 days (high complexity) or 14 days (moderate complexity). (Figure 1).

Transitional Care Management (TCM) workflow showing tasks completed by Patient Data Coordinator, Care Coordinator Nurse, and Primary Care Provider. Processes coded in green indicate the 3 steps required by Centers for Medicare and Medicaid Services (CMS) to support use of TCM billing codes. Red stars indicate key process indicators captured in the electronic health record and used in our TCM dashboards. An Episode is an electronic health record (EHR) tool for tracking TCM services related to a single discharge.

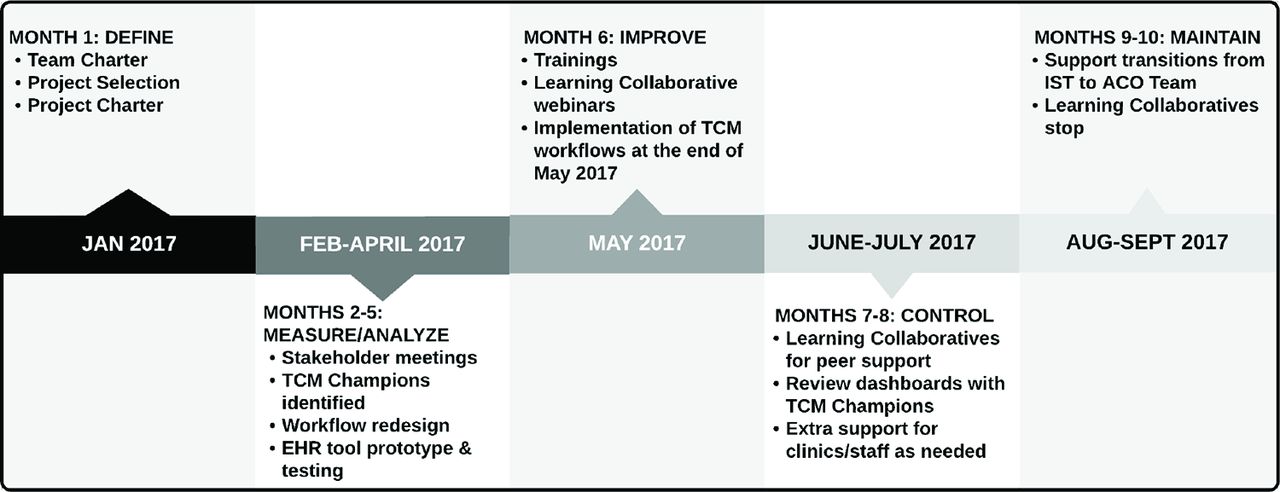
Timeline for Transitional Care Management (TCM) quality improvement project. Abbreviations: IST, Improvement support team; ACO, Accountable care organization; EHR, electronic health record.
A meta-analysis by Le Berre et al. found that services similar to TCM reduced all-cause mortality and hospital readmissions at 3, 6, 12, and 18 months after discharge.5 Across 90 randomized trials, TCM services decreased mortality and readmissions at 18 months by 7% and 21%, respectively, compared with usual care without TCM services. Despite clinical and financial imperatives, little is known about successful quality improvement (QI) approaches to developing TCM services. A review of the literature found numerous articles on the processes and outcomes of TCM but none addressing specific methods to increase the use of TCM.
Specific Aims
Our primary aim was to develop new workflows and electronic health record (EHR) tools that would increase TCM services. We had 3 specific aims: (1) to increase the use of TCM phone calls and TCM office visits, (2) to increase use of the TCM billing codes; and (3) to spread the use of TCM tools across all clinics within the PCSL. Our secondary aim was to lower hospital readmissions rates.
Methods
Clinical Context
Health Care System
We implemented TCM in Dartmouth Health, an integrated system with a catchment area of 4,250-square miles that is 95% rural. The system employs all the providers and staff who share a single EHR (Epic). The system has 4 geographic divisions, each composed of several multi-specialty clinics. In 2016, shortly before this project, the system created service lines to standardize care pathways and operations across divisions. The primary care service line (PCSL) included 107 adult primary care providers (PCPs) serving 165,382 unique patients (Table 1). This was the first PCSL standardization project across all 4 divisions.
Characteristics of Primary Care Service Line Divisions at Baseline (Fiscal Year 2018), Including Descriptors of Patients and Primary Care Providers (PCPs)
Divisions
Division A includes 3 primary care (PC) clinics located adjacent to the affiliated academic medical center (AMC). All PCPs teach, and many engage in research or QI activities. Divisions B, C, and D, located 1 to 2 hours south of the AMC, include 12 highly dispersed clinics functioning as a large, nonacademic, community group practice (CGP). Divisions B, C, and D are not affiliated with any local hospitals, and almost none of the PCPs teach or conduct research or QI work.
Prior TCM Efforts
There was substantial variation in TCM workflows, staff roles, and EHR tools. Division A had piloted some TCM QI work in 1 clinic. Independently, division D had piloted a separate TCM project in 1 clinic. All 4 divisions had done prior projects getting lists of patients discharged from local hospitals and did so reliably using a variety of workflows involving faxes, electronic notifications, and access to hospital EHRs.
Interventions
To develop and implement our TCM efforts, we adopted the learning health system (LHS) framework, introduced by the US National Academy of Medicine in 2011.6 Menear et al. found that exemplar LHS organizations are organized around 6 pillars: scientific, social, technological, policy, legal, and ethical “to enable cycles of continuous learning and improvement to be routinised and embedded across the system.”7 Our approach is mapped to Menear's 6 pillars (Table 2). In particular, we describe below the Improvement Support Team and the Learning Collaborative which support the Social Pillar.
Learning Health System (LHS) Pillars Using Menear Model With Components Developed for Transitional Care Management (TCM) Quality Improvement Project in a Rural Primary Care System
During a 42-Month follow-up of Accountable Care Organization (ACO)-Enrolled Patients, Admissions with Subsequent TCM Services (n =101) Had a 5% Readmission Rate, Compared with an 11.9% Readmissions Rate for Admissions That Did Not Receive Subsequent Transitional Care Management (TCM) Services (n = 2103), Representing a 58% Decrease in the Readmission Rate (P = 0.03).
Improvement Support Team (IST) Activities
The IST met initially in January of 2017 (Figure 2). The team included experts representing the LHS pillars: a PC physician informatics leader; a Lean 6-Sigma blackbelt analyst; and 3 nurses with experiences as a care coordinator (CC), an educator, and a project manager. We later added a Physician Assistant who had led a TCM pilot project and a care manager from our Accountable Care Organization (ACO). We included a member from each division. The team met in person, weekly, for 7 hours. During the first month, they met with organizational leaders to develop team and project charters. We excluded hospitals as stakeholders because our prior projects had already developed reliable mechanisms for identifying patients being discharged, and the scope of our project started with the PC workflows. Patients were excluded as stakeholders because the focus was on the clinic-facing processes.
The next 3 months involved meetings with clinic staff involved with TCM activities to standardize and improve workflows and EHR tools.8 The team used a hybrid Lean/Model for Improvement approach,9⇓⇓–12 including systems thinking, process flowcharts,13 and rapid redesign based on user testing of protypes.14⇓–16 The IST identified a “TCM Champion” from each division, usually a clinical operations manager. The IST met with Champions to understand the current state of TCM within each division and to propose a standard workflow that meets CMS requirements. The IST also met with billing coders, schedulers, EHR leaders, and data analysts.
The IST created standardized TCM job aids for Patient Data Coordinators (PDCs), Care Coordinator nurses (CCRNs), and PCPs. Job aids targeted 3 key TCM components:
TCM Episode: PDCs obtained daily hospital admission and discharge reports, by fax or web portal. PDCs then documented in our EHR the hospital name, admission and discharge dates, and reason for admission. This EHR documentation related to the discharge and follow-up care was called the “TCM Episode.”
TCM Call: The TCM Episode was routed via EHR messaging to the CCRN who documented 2 attempts to contact the patient within 2 business days of discharge. The date of the TCM call(s) was then documented in the TCM Episode form. The CCRN scheduled the patient for a TCM visit with a PCP within 14 days of discharge.
TCM Visit: A PCP completed the TCM visit, including appropriate documentation and billing code.
The TCM Episode, Call, and Visit were all linked in the EHR to establish that the TCM activities related to a specific discharge. Done correctly, every TCM Episode would have both: a linked TCM Call and a linked TCM Visit. All significant activities in the TCM Episode, Call, and Visit used discrete data capture for use in process measures dashboards.17 For our purposes, complete TCM was required to include all 3 components.
At month 6, we started Learning Collaborative (LC) webinars (described below) to train staff and continue getting user input.18 Several clinics started using the new TCM tools and began giving feedback. Other clinics needed another month to complete training. By month 7, all clinics were using the new TCM system. At month 8, the IST closed the project, handing ongoing work to the ACO operations team. The ACO team continued to enhance and track the use of the TCM tools.
Learning Collaborative (LC)
We utilized a modified Institute for Health Care Improvement (IHI) Breakthrough Series Collaborative approach to facilitate networked learning and sharing of best practices throughout the development and implementation periods.11 The LC included all members of the IST, TCM Champions, and practice managers from each division. LCs built front-line capability for improvement and implementation through shared experiential learning. Meetings via Webex virtual conferencing software ran weekly for 2 months before and during launch of the TCM tools, then decreased to biweekly for several months. A QI expert from facilitated the LC. The sessions provided QI skills instruction, sharing of ongoing experiences of teams and coaches in the project, and review of run chart dashboards.
Measures
Primary Aims
The measures for the primary aims included the 3 TCM components: (1) TCM Episodes documented in the EHR by the PDCs, (2) TCM Calls documented by CCRNs, and (3) TCM Visits documented by PCPs. We also tracked PCP use of TCM billing codes (99495 or 99496). These measures allowed us to track each TCM step, determine which clinics or staff were doing well, and use the dashboards to reinforce correct workflows during our LCs. Each measure is captured as a discrete event in the EHR database with 100% reliability. Validation work repeatedly confirmed that our extraction into our Excel dashboards was accurate and reliable.
Secondary Aim
To evaluate the impact of TCM on readmissions, we identified patients who were enrolled in an ACO and had been admitted to a hospital with lengths of stay (LOS) between 5 and 15 days. Within that population, we compared the number of readmissions for patients who had completed all 3 TCM services to those who had not. If any component (Episode, Call, or Visit) was missing, we considered TCM services to be incomplete. ACO patients were not randomized to receive TCM services, rather this was a pragmatic, empiric cohort.
Analysis
We used descriptive statistics to describe the clinical context. Inferential analyses set statistical significance α level at P < .05. We used Microsoft Excel 2016 (Redmond, WA) with SigmaZone SPC Excel plug-in (Orlando, FL) for statistical analyses. We used Westgard rules for detection of special cause variation in statistical process control (SPC) analyses.
Primary Aims
SPC analyses allowed us to evaluate primary aims rigorously with real-time, time-series data. We determined nonrandom (special cause) variations in performance of our implementation to inform ongoing improvement work. We used XmR analyses for continuous measures. For proportions (p) analyses, we used the number of TCM Episodes as the denominator for assessing completion rates of TCM Calls, Visits, and TCM billing codes. We used a paired t-test to compare mean TCM Episodes per month and analyses of variance to assess for significant differences in performance between divisions pre- and post-IST intervention.
Secondary Aim
Readmission rates were analyzed using descriptive statistics and Fisher's exact test (2 × 2) to compare rates for ACO patients who did or did not receive complete TCM services during the study period.
Ethical Considerations
The institution's Committee for the Protection of Human Subjects determined the project was a quality improvement activity not requiring Institutional Review Board review or approval as human subjects research.19
Results
Process and Outcome Measures
TCM Episode Documentation
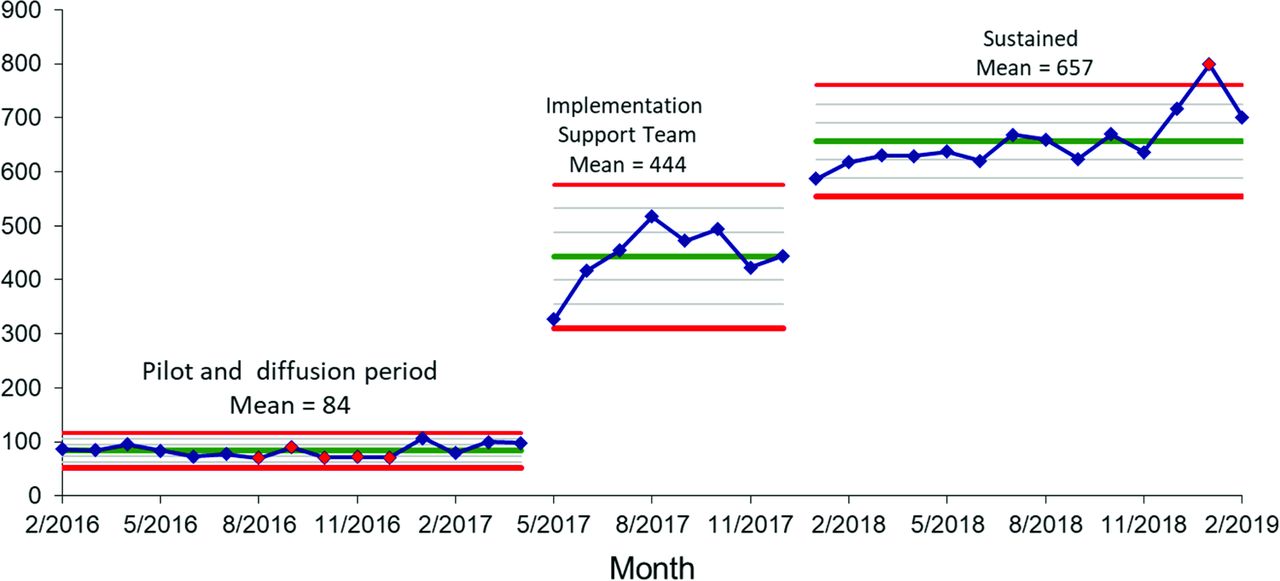
Before May 2017, TCM Episodes were documented in the EHR only sporadically and only in 2 divisions (A, D) despite a pilot period of more than 1 year. During the 5-month IST engagement period, system-wide average count of TCM Episodes per month increased by 529%, from a baseline of 84 to 444 (P < .01) (Figure 3). After the IST ended their support, average monthly Episode counts were sustained at 657, an increase of 780%.

Transitional Care Management (TCM) Episodes – Monthly number of TCM Episodes documented in the electronic health record (EHR) sustained an increased from 84 to 657 (780% increase) following 4 months of Implementation Support Team (IST) engagement (P < .01).
Phone Calls and Office Visits
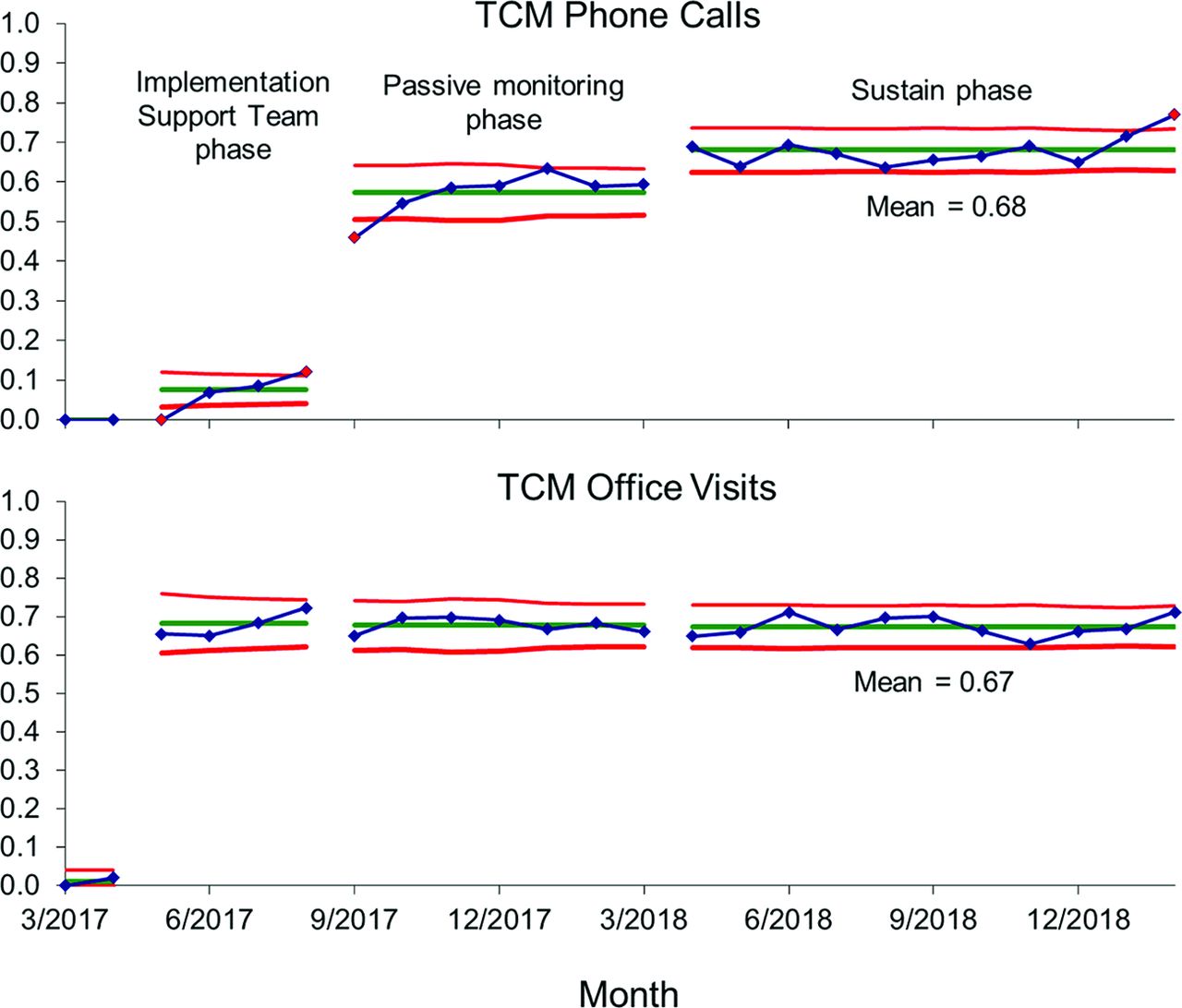
The percentage of all TCM Episodes (measured as aggregate rates of postdischarge phone calls) increased from 0% to 12% during the 4 months of IST involvement, continued to increase after the IST ended to a sustained rate of 65% (Figure 4), and maximized at 77% at the end of the study. The proportion of TCM Episodes with a postdischarge Visit increased rapidly from near 0% before the IST, reaching 70% across all divisions in the first months (Figure 4). After IST involvement ended, Visits were sustained at 68% of all TCM Episodes.

Monthly Transitional Care Management (TCM) services as a percent of TCM Episodes – Use of TCM Call and TCM Visit increased during the Implementation Support Team (IST) Learning Collaborative (May through September 2017). The gains continued to increase for phone calls even after the IST engagement ended. During the sustain phase, with no IST involvement, 68% of TCM Episodes had a follow-up Call within 2 business days, and 67% of TCM Episodes have had a Visit within 14 days of discharge.
Billing Codes
During a 2-month, pre-IST baseline period, TCM billing code were used at 47% of TCM Episodes in pilot sites in divisions A and D. During the 4 months following implementation, the system-wide rate of TCM code use was stable and averaged 41% of TCM Episodes. Between months 5 to 9 postimplementation, the system rate dropped to 31%, then held for the following year at a monthly average of 13%.
Differences Between Divisions
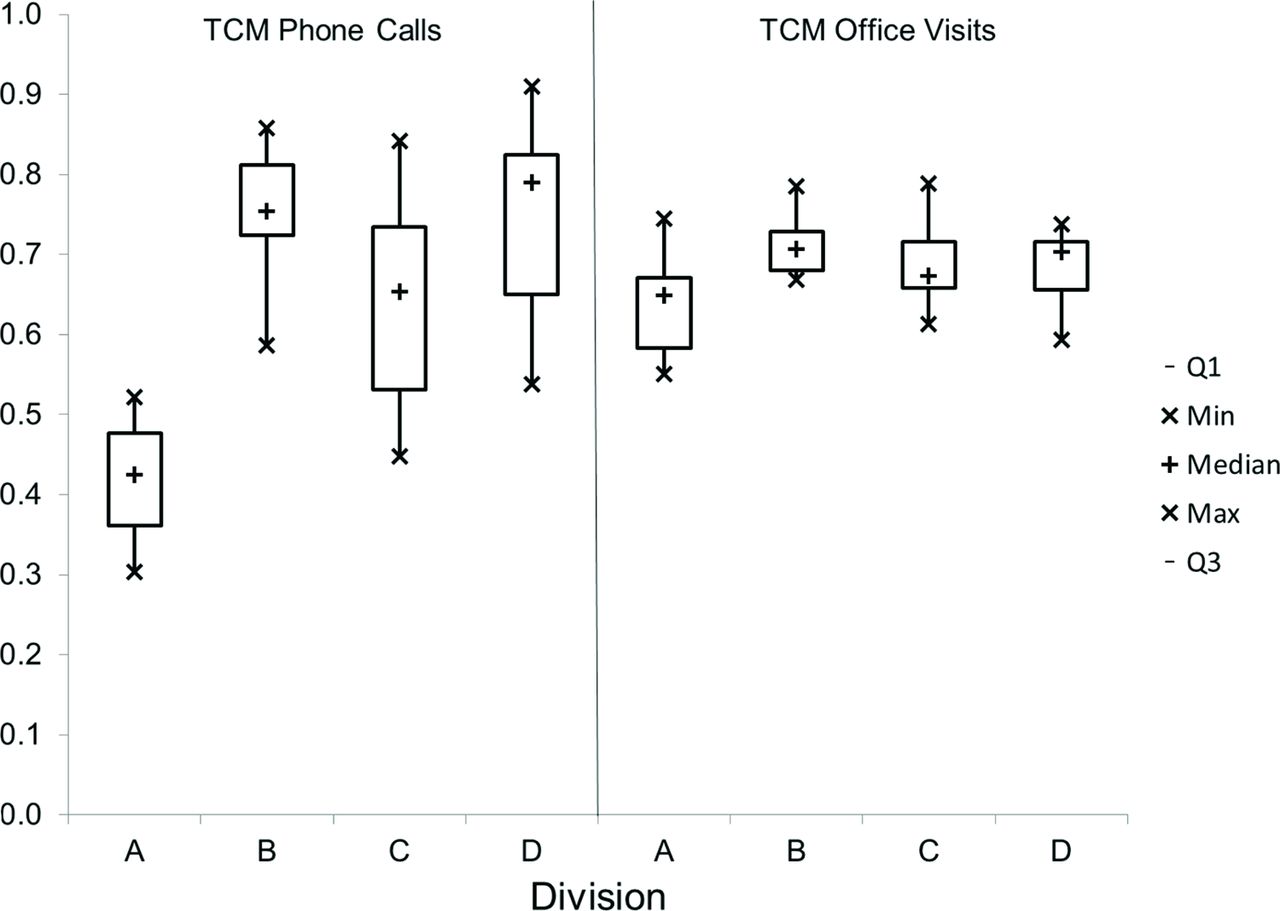
In division A, a smaller percent of TCM Episodes were converted to Calls (F = 50.7, P < .01) and to Visits (F = 7.4, P < .01) compared with the 3 other divisions further south (Figure 5). Use of TCM Billing Codes did not differ significantly between divisions.
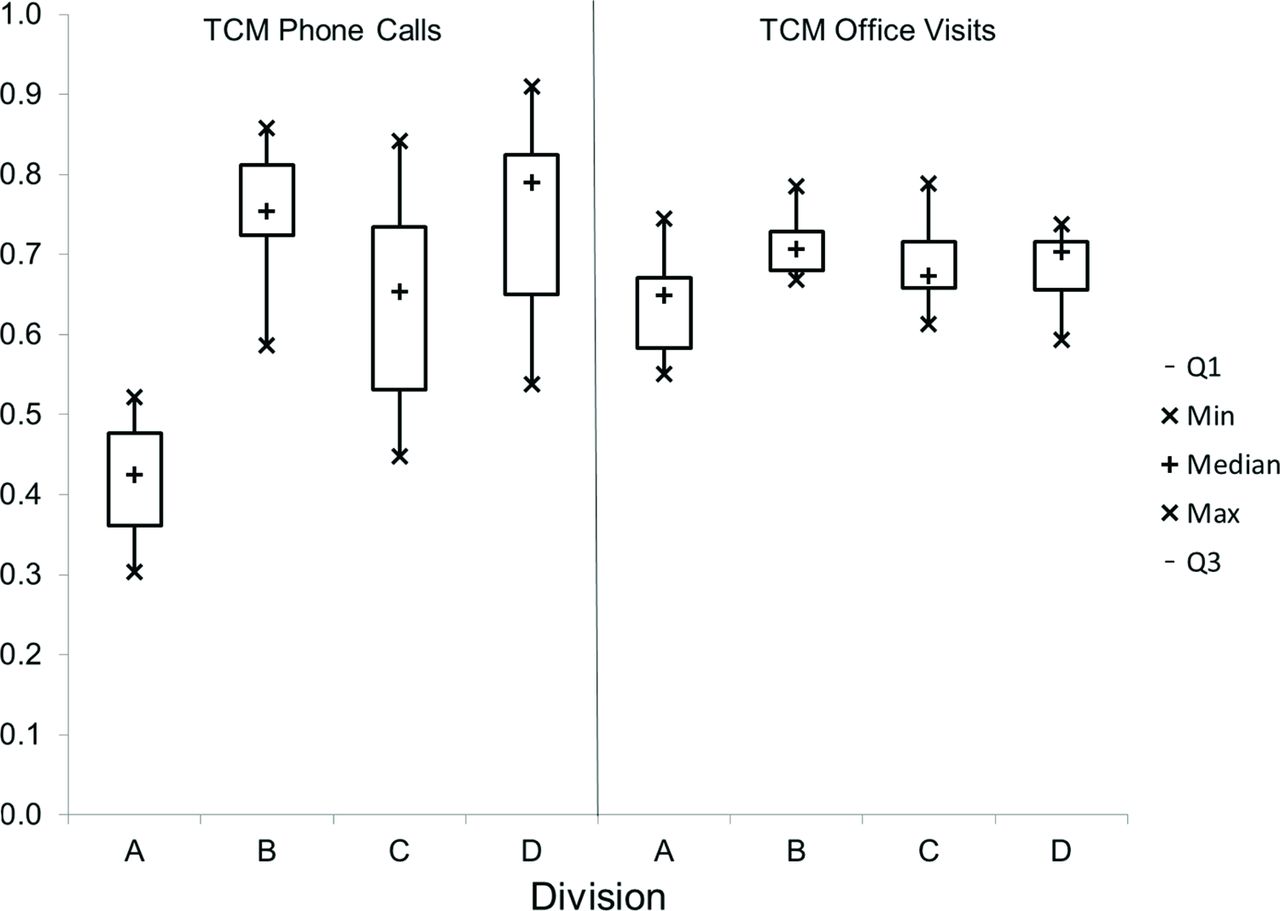
Rates of Transitional Care Management (TCM) Calls and TCM Visits as a percent of TCM Episodes. Division A had lower rates of TCM Calls (F = 50.7, P < .01) and TCM Visits (F = 7.4, P < .01) compared with the 3 other divisions. The use of TCM billing codes was not significantly different between divisions.
Impact of TCM on Hospital Readmissions
The ACO data included 2204 admissions with LOS between 5 and 15 days (Table 3). The readmission rate for patients receiving all 3 TCM services (Episode, Call, and Visit) was 5.0% (n = 101) versus a rate of 11.9% for patients who did not receive complete TCM services (n = 2103, P = .03).
Discussion
Summary
Primary Aims
The use of a multi-component implementation strategy consisting of an IST, LHS, and LC approach was effective at increasing documentation of TCM Episodes, Calls, and Visits very quickly. The use of the tools continued to increase across the system even after the IST engagement and LC ended. Use of TCM billing codes also increased with the launch of the TMC tools but was not sustained after the IST finished its work. Divisions B, C, and D demonstrated comparable improvement. Division A had a significantly lower rate of Calls and Visits than the other 3 divisions. In a subset analysis of ACO data from 2017 to 2020, of 2204 admissions, only 4.6% received all 3 components of TCM: Episode, Call, and Visit.
Secondary Aim
From the ACO data, complete TCM services (Episode, Call, and Visit) lead to a statistically significant 58% relative decrease in readmissions. Any 1 TCM component alone (Episode, Call, or Visit) did not decrease admissions, suggesting a synergistic effect: TCM seems to require all 3 components to be beneficial.
Interpretation
We used a RE-AIM framework to evaluate the implementation.20 A combination of QI, LC, and LHS elements, integrated thoughtfully, did facilitate a successful implementation.
Reach
The use of TCM Champions and LC webinars were effective at spreading the TCM tools across the system. While LC participation was not a measure in this QI project, anecdotal evidence suggests that the sessions were useful. Limited in-person coaching, targeting lagging clinics or providers, was an additional way of reaching staff. By the end of the project, all clinics had engaged in the project and were using the new TCM tools.
Effectiveness
The QI, LC, and LHS components resulted in significant increase in TCM Episodes, Calls, and Visits but not TCM billing codes. A subset analysis of ACO data demonstrated a statistically significant 58% decrease in readmission rates. Furthermore, there seems to be an important synergy between tracking the Episodes, completing the Call, and conducting the Visit. Decreased readmission rates seem to depend on all 3 components.
Adoption
The IST was an effective quality improvement and dissemination engine. The IST was given protected time to work together, had access to senior leaders to facilitate overcoming obstacles, and consisted of talented individuals with complimentary skills. Use of the TCM tools showed stable or increased adoption after the end of the IST across the entire organization, although adoption was lower in division A.
Implementation
The designed workflows matched the CMS requirements for TCM and fulfilled the operational requirements identified by the TCM Champions. The LC delivered uniform training to all divisions, and ongoing webinars reinforced standardization. The LHS key processes indicators, tracked in the EHR and on our dashboard, allowed us to identify and correct workflows to improve fidelity. Overall, we feel that the intervention was implemented very close to its design. The study was not designed to determine which elements of the intervention (IST, LC, LHS) were the most valuable for fidelity. Completing all 3 TCM components (Episode, Call, and Visit) for each patient remains difficult, with an overall completion rate of less than 5% in our ACO sample, over 3 years following the IST project. Although many patients do not need or decline TCM services (usually patients following up with a surgeon or medical specialist), our low completion rate has become an area for ongoing improvement work.
Maintenance
At the end of the IST project, clinical operations teams incorporated TCM training into staff training. Leadership oversight transferred from the PCSL to our ACO management team, and they continued to improve and monitor the tools for several years. Turnover in the data analytics team resulted in the dashboard no longer being maintained after several years. New providers were not trained on TCM billing once the project ended, so more than 50% of current PCPs are not familiar with the project. Lack of sustained PCP training may partially explain the low use of TCM billing codes.
Limitations
As a QI project, we did not measure the IST, LC, and LHS as processes themselves to better understand the impact. We also did not study the impact of specific components, so we cannot gauge how much benefit users derived from different EHR tools, the LC, or the data dashboards. It is possible that a more streamlined process and fewer tools in the EHR could have resulted in similar outcomes.
We had claims data for tracking readmissions for only a small percent of our patients. Changes in policy under the 2021 CURES Act, requiring hospitals to share information electronically with fewer barriers may overcome issues of missing data going forward. Patients in our ACO population were not randomized, and only a small percent received complete TCM services. The impact of our pragmatic cohort is unclear: the 4.6% of patients receiving TCM may be perceived by staff as needing care coordination based on high readmission risk, or these patients could be the most engaged in their own care and be less likely to be readmitted.
The project was too brief to determine if we reduced mortality, and we did not have data to measure the total cost of care. These are key metrics at the population level that would be great to study. We did not evaluate the patient or clinic staff experience with the provision of TCM services, but we are doing so in subsequent work. The project was launched when the PCSL was new. During the project and shortly after it ended, there was turnover in several key leadership positions, and both the IST and the PCSL were dissolved. This organizational churn limited the impact on TCM services.
Conclusions
We demonstrated the effectiveness of a multi-component, QI approach—consisting of an interdisciplinary improvement support team, a virtual learning collaborative, and a learning health system approach—on increasing the use of TCM services across a rural Primary Care Service Line. Limited data from our ACO patients shows that patients receiving both a TCM Call and TCM Visit have a readmission rate 58% lower than patients who did not receive both services. Future research should focus on (1) determining relative impact specific TCM elements (e.g., reviewing records, phone call, medication review, office visit) and risk of readmission and (2) barriers to using TCM billing codes, including workflow, EHR design, and provider behaviors.
We believe that these results may be replicable at other organizations for several reasons: the tools all used functionality that is readily available in most EHRs; the IST followed standard QI processes for workflow optimization and standardization; and the LC and LHS are models that has already proven to be useful across many organizations. The use of similar methods could accelerate TCM adoption at other institutions.
Acknowledgments
Thanks to Lora Council for leadership in the Primary Care Service Line, Steve Sarette and Mike Grube for data analytics, Patricia Laliberte for project management, Elizabeth Morrill for operational leadership, Peter DiMilia for editing and statistics excellence, the Dartmouth Health staff and providers dedicated to improving clinical care, and the Dartmouth Collaboratory for Implementation Science for methodological assistance.
Notes
This article was externally peer reviewed.
Conflicting interests: None.
Funding: A portion of this project was supported through the HRSA Geriatric Workforce Enhancement Program (DSM, JR) and the Collaboratory for Implementation Science at Dartmouth (BJO).
To see this article online, please go to: http://jabfm.org/content/35/3/537.full.
- Received for publication November 23, 2019.
- Revision received November 24, 2021.
- Revision received December 8, 2021.
- Accepted for publication December 10, 2021.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}