
Article Figures & Data
Figures
- Figure 1.
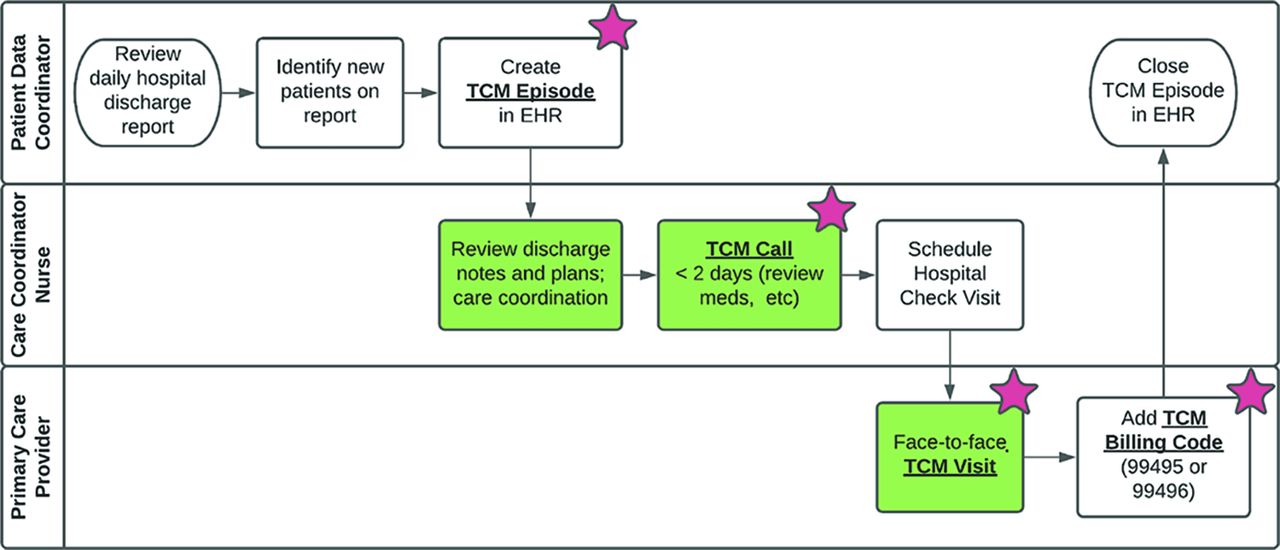
Transitional Care Management (TCM) workflow showing tasks completed by Patient Data Coordinator, Care Coordinator Nurse, and Primary Care Provider. Processes coded in green indicate the 3 steps required by Centers for Medicare and Medicaid Services (CMS) to support use of TCM billing codes. Red stars indicate key process indicators captured in the electronic health record and used in our TCM dashboards. An Episode is an electronic health record (EHR) tool for tracking TCM services related to a single discharge.
- Figure 2.
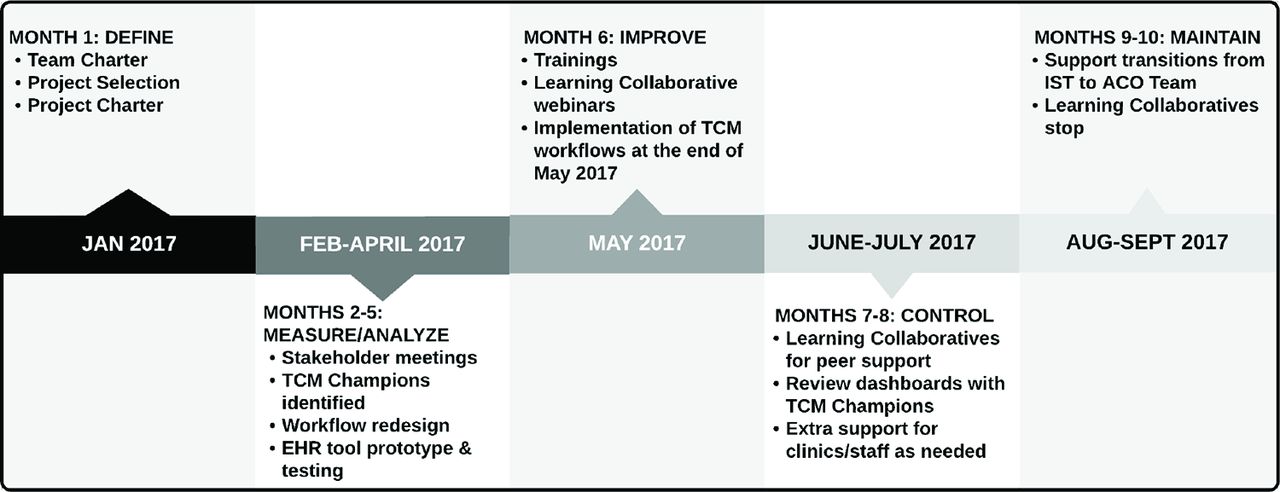
Timeline for Transitional Care Management (TCM) quality improvement project. Abbreviations: IST, Improvement support team; ACO, Accountable care organization; EHR, electronic health record.
- Figure 3.
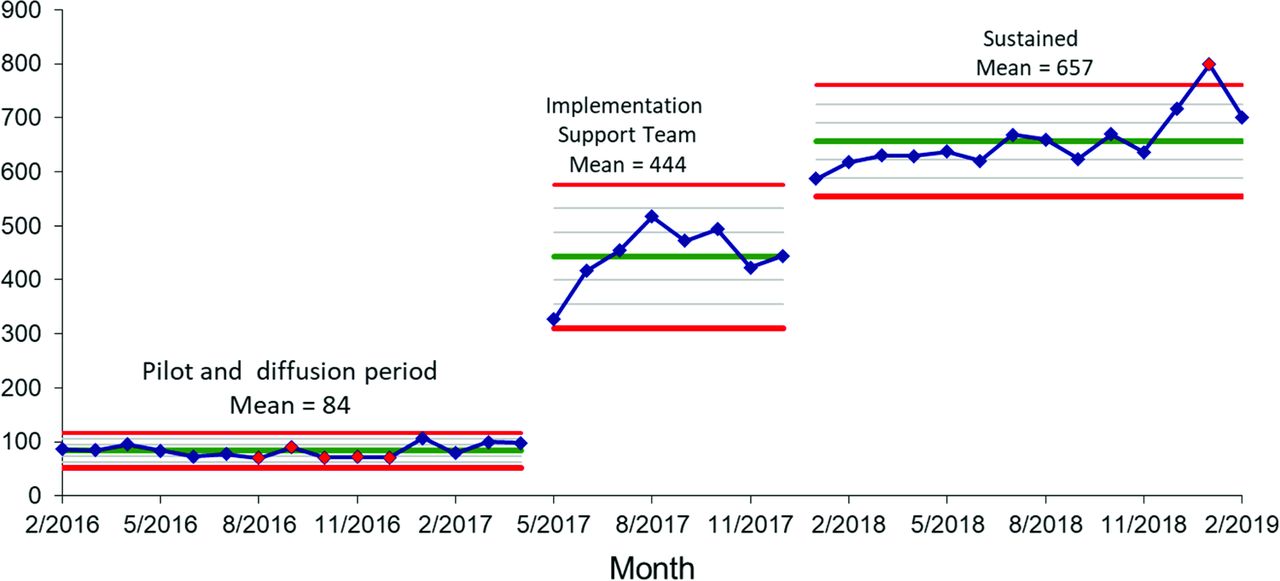
Transitional Care Management (TCM) Episodes – Monthly number of TCM Episodes documented in the electronic health record (EHR) sustained an increased from 84 to 657 (780% increase) following 4 months of Implementation Support Team (IST) engagement (P < .01).
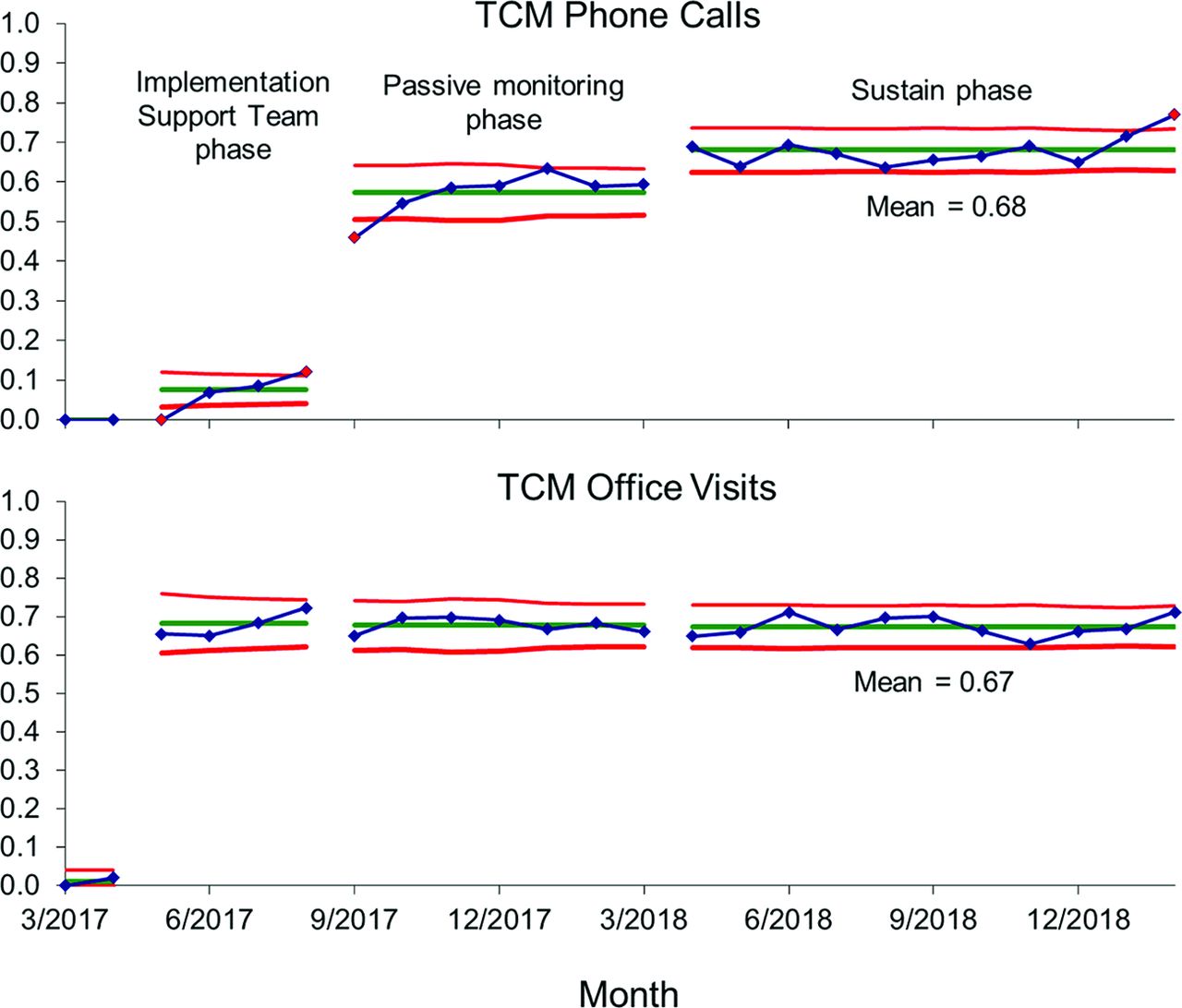
- Figure 4.
Monthly Transitional Care Management (TCM) services as a percent of TCM Episodes – Use of TCM Call and TCM Visit increased during the Implementation Support Team (IST) Learning Collaborative (May through September 2017). The gains continued to increase for phone calls even after the IST engagement ended. During the sustain phase, with no IST involvement, 68% of TCM Episodes had a follow-up Call within 2 business days, and 67% of TCM Episodes have had a Visit within 14 days of discharge.
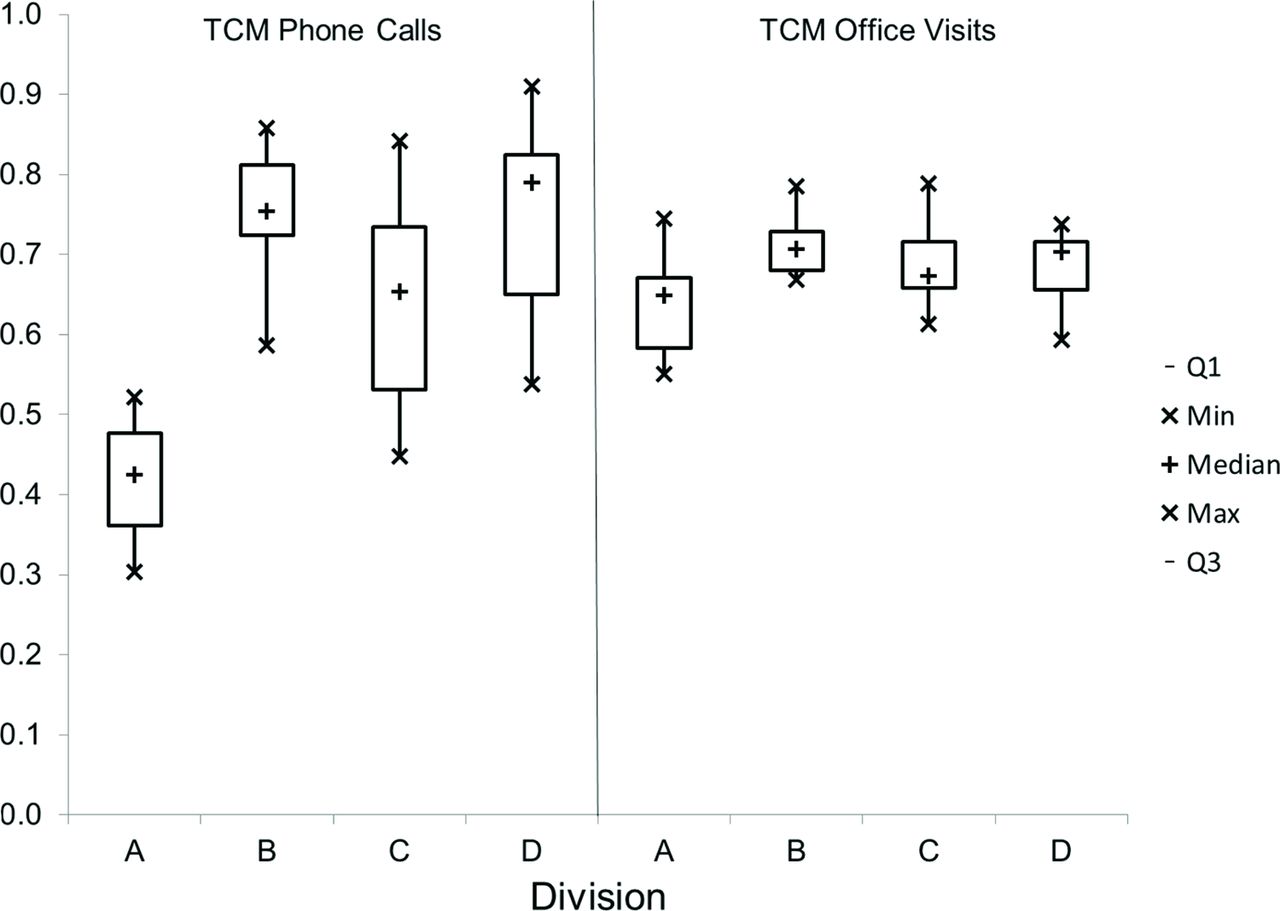
- Figure 5.
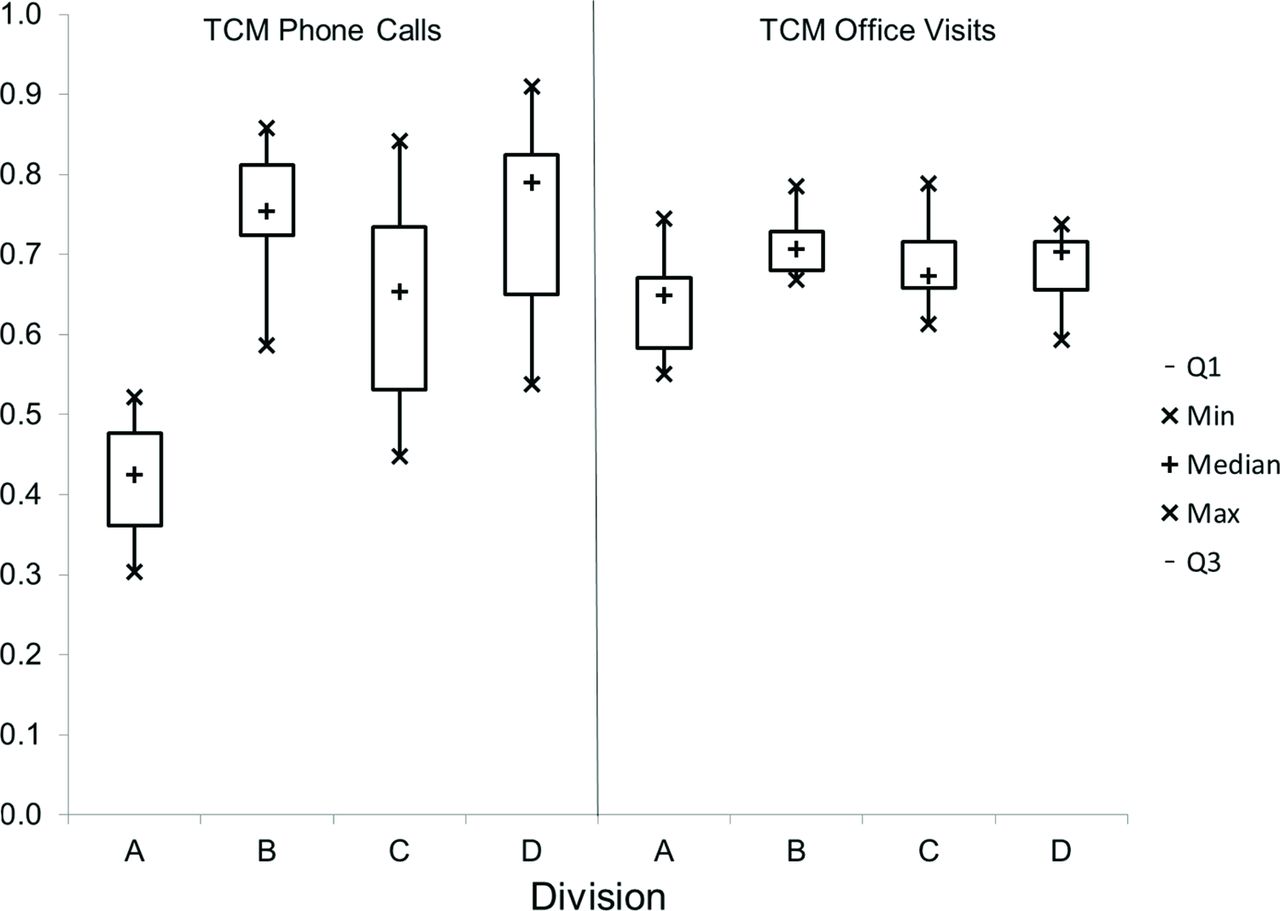
Rates of Transitional Care Management (TCM) Calls and TCM Visits as a percent of TCM Episodes. Division A had lower rates of TCM Calls (F = 50.7, P < .01) and TCM Visits (F = 7.4, P < .01) compared with the 3 other divisions. The use of TCM billing codes was not significantly different between divisions.




Tables
- Table 1.
Characteristics of Primary Care Service Line Divisions at Baseline (Fiscal Year 2018), Including Descriptors of Patients and Primary Care Providers (PCPs)
Division Division A Division B Division C Division D Empanelled Patients 3,0813 2,2727 5,7424 5,4418 Age Mean 46 37 37 40 Age SD 24 24 22 22 Female 57% 54% 55% 54% Private Insurance 65% 73% 74% 75% Medicare 23% 20% 16% 17% Medicaid 7% 5% 7% 6% PCPs (n) 28 19 24 36 Physicians 68% 74% 71% 75% Advanced Practice Providers 32% 26% 29% 25% Family Medicine 59% 63% 33% 72% Internal Medicine 41% 37% 67% 28% PCPs per 1000 Patients 0.91 0.84 0.42 0.66 Abbreviations: SD, standard deviation.
- Table 2.
Learning Health System (LHS) Pillars Using Menear Model With Components Developed for Transitional Care Management (TCM) Quality Improvement Project in a Rural Primary Care System
LHS Pillar Elements TCM Project Activities Scientific • Scientific expertise
• Academic or research institutes, centers, and groups
• Research training programs and knowledge-sharing activities
• Research funding agencies and programs• Use of best practice guidelines for – TCM clinical activities
– Technology
– QI, implementation, and dissemination methods
– Learning Collaboratives
– Training tools
• Use of subject matter experts from The Dartmouth Institute for Health Policy and Clinical Practice
• Dissemination of findings at local QI meetings and national publicationSocial • Multi-stakeholder networks and learning communities
• Service or partnership agreements
• Stakeholder engagement mechanisms (e.g., committees, advisory groups)• Development of the Improvement Support Team (see Methods section)
• In-person and virtual Learning Collaborative (see Methods section)Technological • Expertise in information technology and data science
• Information technology systems
• Health technologies or devices
• Data infrastructures (e.g., electronic health records, clinical or administrative databases, clinical registry)
• Communication technologies and platforms
• Web or mobile applications
• Data warehouses and marts
• Interoperability frameworks• Use of single EHR across all clinical sites
• Uniform data entry for all key process indicators
• Real-time data capture in clinic
• EHR clinical decision support alerts to support key processes
• Daily data extract from EHR into QI database
• Data visualization using statistical process control (SPC) charts
• Ability to filter SPC charts at multiple scales: provider, clinic, region, or system
• Interoperability frameworksPolicy • Governance and accountability structures and systems
• LHS policies
• LHS performance frameworks and incentive systems
• Funding mechanisms for LHS operations and sustainability• Creation of the Primary Care Service Line allowed for system-wide alignment and project prioritization.
• Development, chartering, and funding of the Improvement Support Team
• Organization involvement in risk-based contracts including Accountable Care Organizations drives need for reduced readmissions
• PCP payment based on relative value unit payments is an incentive for TMC work
• CMS payments for TMC and penalties for readmissionsLegal • Privacy legislation
• Laws governing healthcare institutions, organisations and professionals
• Other laws, regulations and rules relevant to LHS activities• Privacy legislation related to data use in healthcare (HIPAA, etc)
• Healthcare system contracts with payers.Ethical • Ethics expertise
• Ethical review boards and committees
• Ethics guidelines, frameworks and rules• Institutional Review Board determined that the TCM project was not human subjects research, making sharing of data much easier
• Decision to make TCM services available to all patients regardless of location, medical conditions, insurance status, or other factors - Table 3.
During a 42-Month follow-up of Accountable Care Organization (ACO)-Enrolled Patients, Admissions with Subsequent TCM Services (n =101) Had a 5% Readmission Rate, Compared with an 11.9% Readmissions Rate for Admissions That Did Not Receive Subsequent Transitional Care Management (TCM) Services (n = 2103), Representing a 58% Decrease in the Readmission Rate (P = 0.03).
No TCM Services TCM Services Relative Decrease in Readmission Rates Division Readmissions / Admission (n) Readmission Rate Readmissions / Admission (n) Readmission Rate A 41/317 12.9% 0/4 0.0% 100% B 43/445 9.7% 1/28 3.6% 63% C 95/739 12.9% 3/43 7.0% 46% D 71/602 11.8% 1/26 3.8% 67% System-wide 250/2103 11.9% 5/101 5.0% 58%




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}