
Abstract
In the evolving landscape of health care, marked by increasing physician distress, the role of family physicians in leadership positions emerges as crucial for driving systemic improvements. Drawing from 9 years of collective experience as chiefs of staff, this commentary outlines a framework for family physicians serving in the Chief of Staff, Medical Staff President role or other physician executive positions aimed at improving physician well-being. Recognizing the comprehensive scope of practice and team-based orientation of family medicine, we highlight the unique capabilities of family physicians to foster organizational changes that address the root causes of physician burnout. The proposed framework emphasizes the importance of effective communication channels to ensure the medical staff's voices are heard and valued. It advocates for physician-centered approaches to credentialing and privileging processes, equitable incident reporting systems, and supportive measures for physicians facing professional challenges. By implementing a wellness-oriented framework, healthcare organizations can safeguard the future of the medical profession and create a healthcare system that prioritizes the well-being of both patients and clinicians.
- Burnout
- Employee Health
- Family Medicine
- Family Physicians
- Health Services
- Leadership
- Medical Staff
- Patient Safety
- Physician Satisfaction
- Primary Health Care
Introduction
Given the rising challenges in health care, including high levels of physician distress exacerbated by the COVID-19 pandemic, it is important that leaders address the problems in the practice environment that contribute to these challenges. Family physicians’ systems approach to medicine, orientation toward service, comprehensive scope of practice, and team-based orientation facilitate an organizational perspective that makes them well-suited to pursue operational leadership roles that enable them to address these challenges.
Extensive research as well as systematic reviews and meta-analysis have demonstrated that occupational distress in physicians has important implications for the health care system, including impacts on quality of care, patient satisfaction, cost of care and access to medical care.1 Family medicine’s comprehensive scope of practice and team-based orientation facilitate an organizational perspective on solutions to occupational distress across all specialties. Studies demonstrating the efficacy of organizational interventions have published,2 and an increasing proportion of US hospitals and health care organizations are implementing organizational approaches.3–4
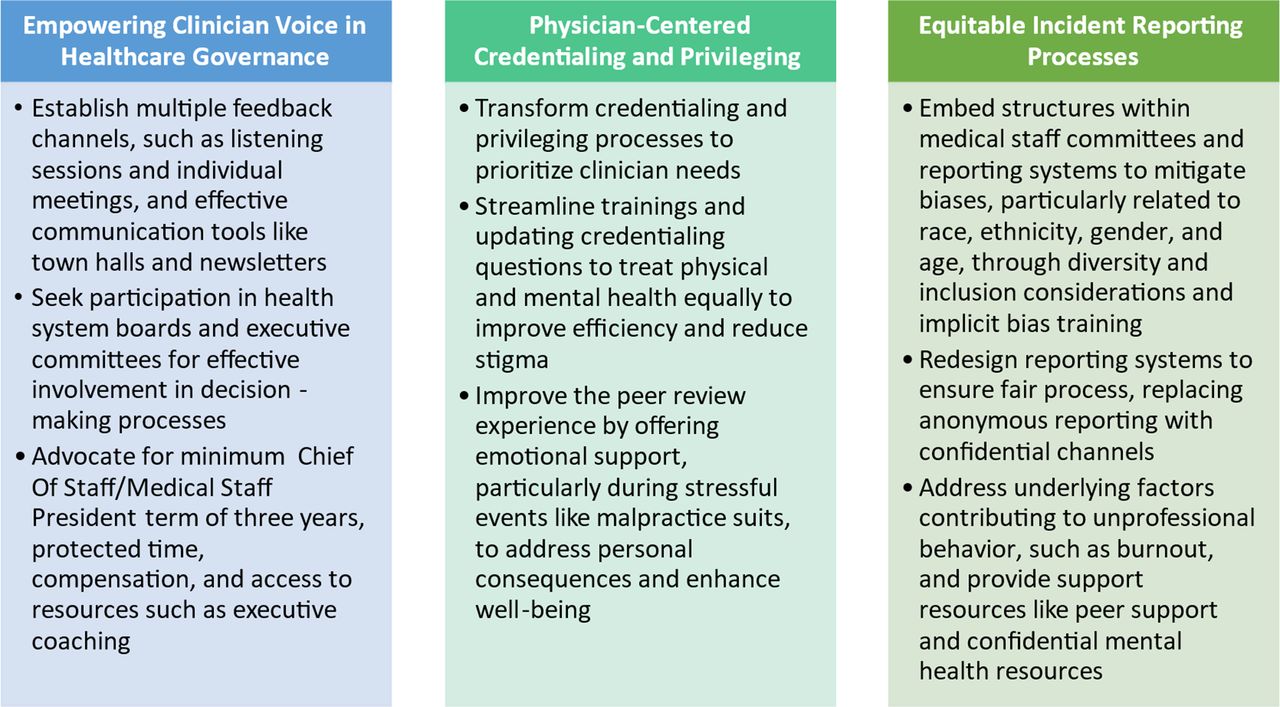
All organizational leaders have a role to play in driving system level change.5 Health care organizations naturally turn to physicians for leadership and credibility regarding clinical issues, often viewing them as the bridge between clinicians, operational staff and senior leadership. Given their expertise and insight into all aspects of the delivery system, family physicians are well equipped to serve in senior physician leadership roles. The Chief of Staff, also referred to as the Medical Staff President in some institutions (COS/MSP), is an established leadership position in large health care organizations and typically oversees a variety of functions including credentialing and privileging, updating the medical staff regarding hospital operational initiatives, fostering interdisciplinary professionalism and managing professionalism complaints, shaping organizational policies, and serving on leadership committees where strategic organizational decisions are made. Based on the authors’ 9 years of collective experience as Chiefs of Staff, we present a framework in Figure 1 for the COS/MSP to use these leverage points to mitigate occupational distress and promote professional fulfillment for physicians.

Opportunity domains for the chief of staff/medical staff president to advance clinician well-being.
Empowering Clinician Voice in Health Care Governance
Physician executives, particularly the COS/MSP, serve as liaisons between operational leaders and the medical staff. Family physicians possess well-developed communication skills enabling them to foster relationships and to develop a deep understanding of the needs and concerns of the medical staff. We recommend the COS/MSP establish multiple feedback channels for medical staff to provide input, such as listening sessions and individual meetings with leaders and medical staff, to understand and address medical staff concerns. Providing multiple avenues to elicit medical staff feedback demonstrates respect and appreciation to the medical staff.
Effective communication channels, such as town halls and newsletters, keep medical staff informed of organizational priorities and facilitate alignment with patient care, quality, and sustainability. The COS/MSP should also regularly communicate appreciation and gratitude for the contributions of physicians to the organization. Although awards and recognition banquets are the most traditional form of such appreciation, other expressions recognizing the demands of clinical work and providing the resources and support for physicians to perform it effectively may be equally or more important. This includes attending to staffing, workflows, and the efficiency of the practice environment. Allocating dedicated space for breaks during the workday (eg, physician lounge, break rooms) is also important. Incorporation of free coffee, fruit, and healthy snacks are often greatly appreciated by clinicians on busy shifts with limited break time. Similarly, advocating for adequate space for lactation rooms in reasonable proximity to clinical care delivery areas should also be a priority to support physicians returning from parental leave.
Including the COS/MSP in the health system board and executive leadership team committee ensures the clinician voice is considered in the decision making processes. Regular meetings with senior leaders as well as a dedicated budget, and dedicated administrative support are vital components for the success of physician leaders in the COS/MSP key role. Considering the lengthy onboarding process typically required for a new COS/MSP to become fully acclimated, it is advisable to institute a minimum term of 3 years for the COS/MSP role. In addition, providing protected time, compensation, and access to resources such as executive coaching can further support COS/MSP effectiveness.
Physician-Centered Credentialing and Privileging
Oversight of the credentialing and privileging process is a core responsibility of the COS/MSP, guaranteeing that all health care professionals maintain competency and stay current in their fields. We suggest implementing several steps to transform the process into one that prioritizes the needs of clinicians. Streamlining annual training and replacing lengthy online modules with targeted briefs can improve efficiency and reduce burden. Training should be periodically refreshed and interactive to maintain physician engagement and interest. Credentialing questions about physical and mental health conditions can heighten or lessen stigma about help seeking, depending on how they are worded.6 These questions should be updated to treat physical and mental health issues similarly, avoiding outdated inquiries that violate American Disability Act regulations.7 Lastly, going through the peer review process (eg, being named in a malpractice suit or accused of unprofessional behavior) should consider very stressful events in the life of the physician. Emotional support should be provided to physicians going through this process. The frequency of malpractice suits and their negative associations with quality of life, career satisfaction, and overall well-being emphasize the need for organizations to not only provide legal guidance but also emotional support to mitigate the personal consequences of malpractice litigation for the physician.
Creating An Equitable Incident Reporting Processes
Setting and ensuring standards of professional behavior is a key function of the medical staff, with the COS/MSP playing a pivotal role in promoting interdisciplinary professionalism and addressing complaints. Traditional social contracts that tolerated unprofessional behavior are outdated. While systems to report such behavior have been established, they have evolved in unintended ways, eroding fair process and leading to issues of bias and discrimination. These systems often fail to consider multiple perspectives and can result in anonymous accusations being interpreted as “truth” without a complete understanding of the events. These systems can also lead to covert racial and gender bias and discrimination. For example, we have heard from women and minority physicians that they received professionalism complaints for giving assertive instructions to team members during a surgical procedure or critical situation that likely would never have been reported had such instructions been given in an identical manner by a male or a nonminority physician. Reports on professional conduct and patient safety, particularly the voluntary nature of these systems, may be influenced by the reporter's implicit biases.8 Structures need to be embedded within medical staff committees, patient safety, and professionalism reporting systems to mitigate biases regarding race, ethnicity, gender, and age. This involves mindful consideration of diversity and inclusion in committee memberships, implicit bias training, and regular collection and reporting of disaggregated data on medical staff diversity throughout the organizational hierarchy, extending inclusion efforts to nonphysician health professionals and patient representatives.
There is also a need for many reporting systems to be redesigned to better adhere to their intent and ensure fair process. The construct of fair process emphasizes that it is important to both 1) achieve the right outcome, as well as 2) attend to the process by which that outcome was achieved. Achieving fair process involves expectation clarity, engagement, and explanation.9 Redesigning professionalism reporting systems to ensure fair process, including replacing anonymous reporting with confidential reporting, is crucial.
Recognizing that physicians experiencing burnout may be more prone to unprofessional behavior10⇓–12 also underscores the importance of addressing underlying factors and providing support as part of the professionalism reporting system. This does not excuse inappropriate behavior, but presents the opportunity to not only address it, but recognize underlying contributing factors which can be addressed it to help prevent future events. For example, when an individual without a history of professionalism complaints receives a new complaint, it is important to systematically assess whether a physician is in distress and, when appropriate, link them to resources such as peer support and confidential mental health and coaching. This approach facilitates the appropriate management of the event while concomitantly supporting a valued individual member of our medical staff.
Conclusion
In the face of mounting challenges for physicians, addressing occupational distress is crucial for the health care system's well-being. Occupational distress among physicians significantly influences health care systems, affecting quality of care, patient satisfaction, cost, and access to medical services. Physicians in executive leadership roles, such as the COS/MSP, play a pivotal role in bridging operational leaders and the medical staff. Family physicians, with their holistic approach to care and leadership, are uniquely positioned to serve in physician executive positions. Efforts by physician leaders can foster values alignment and partnership between the medical staff and the organization that helps enhance physicians’ ability to serve patients and the organization achieve its mission.
Notes
This article was externally peer reviewed.
Funding: Dr. Mahoney receives remuneration for her role as a Board Governor for The Doctors Company. This financial support acknowledges her contributions and responsibilities undertaken in this capacity. Dr. Shanafelt is co-inventor of the Well-Being Index Instruments and the Mayo Leader Impact Index. Mayo Clinic holds the copyright to these instruments and has licensed them for use. Mayo Clinic pays Dr. Shanafelt a portion of royalties received. As an expert in the field of clinician well-being, Dr. Shanafelt often presents grand rounds/keynote lectures and advises organizations on efforts to improve clinician well-being. He receives honoraria for some of these engagements.
Conflict of interest: The authors have no conflicting or completing interests.
To see this article online, please go to: http://jabfm.org/content/38/1/168.full.
- Received for publication March 31, 2024.
- Revision received May 31, 2024.
- Accepted for publication July 22, 2024.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.