
Abstract
Background: National organizations have issued comprehensive cancer survivorship care guidelines to improve care of cancer survivors, many of whom receive care from primary care providers (PCPs).
Methods: We analyzed Porter Novelli’s 2019 fall DocStyles survey to assess use of cancer survivorship care guidelines, receipt of survivorship training, types of survivorship services provided, and confidence providing care among PCPs in the United States. We grouped PCPs by use of any guideline (“users”) versus no guideline use (“nonusers”). We calculated descriptive statistics and conducted multivariable logistic regression analyses to examine guideline use, having received training on providing survivorship care services, and confidence in providing care. Within the panel, sampling quotas were set so that 1000 primary care physicians, 250 OB/GYNs, 250 pediatricians, and 250 nurse practitioners/physician assistants were recruited.
Results: To reach selected quotas, 2696 health professionals were initially contacted to participate, resulting in a response rate of 64.9%. Sixty-two percent of PCPs reported using guidelines and 17% reported receiving survivorship care training. Use of any guidelines or receiving training was associated with reporting providing a range of survivorship services and confidence in providing care. After adjusting for demographic characteristics, guideline users were more likely than nonusers to report assessing genetic cancer risk (OR = 2.65 95% confidence interval (CI) (1.68, 4.17)), screening for cancer recurrence (OR = 2.32 95% CI (1.70, 3.18)) or a new cancer (OR = 1.63, 95% CI (1.20, 2.22)), and treating depression (OR = 1.64, 95% CI (1.20, 2.25)). Receipt of training was also positively associated with providing genetic risk assessment, surveillance for recurrence, as well as assessing late/long-term effects, and treating pain, fatigue, and sexual side effects.
Conclusion: Survivorship care guidelines and training support PCPs in providing a range of survivorship care services.
- Cancer
- Cancer Survivors
- Clinical Guidelines
- Disease Management
- Logistic Regression
- Primary Health Care
- Survivorship
Introduction
Advances in early detection and cancer treatment have resulted in more people becoming long-term cancer survivors, with 5-year relative survival for cancer in the US currently at 66%.1 The aging of the US population will likely lead to more people being diagnosed with cancer, and may also contribute to the growing number of cancer survivors over the next several decades.2 Many cancer survivors face late and long-term effects from their cancer and its treatment, and some struggle with anxiety, depression, and pain as a result of their illness and treatment.3,4
Although some cancer survivors routinely see oncologists for follow up care, many survivors rely on their primary care providers (PCPs) to deliver post-treatment care.5,6 Many PCPs lack formal training in cancer survivorship or feel ill-equipped to provide many elements of survivorship care, leaving gaps in care for some cancer survivors.7⇓⇓–10 A number of studies have revealed that PCPs have low to moderate confidence in their ability to provide basic survivorship services such as surveillance for cancer recurrence or assessing late and long-term effects from treatment, and delivery of guideline-concordant survivorship care for surveillance of recurrence is variable.7⇓⇓⇓–11
To improve cancer survivorship care, several national cancer organizations, such as the American Society of Clinical Oncology (ASCO), the National Comprehensive Cancer Network (NCCN), and the American Cancer Society (ACS), have issued comprehensive cancer survivorship care guidelines.12⇓⇓⇓–16 These guidelines address topics related to surveillance for recurrence, management of late and long-term treatment effects, and other common concerns, such as health promotion. The purpose of survivorship care guidelines is to provide evidence-based care to survivors to ultimately improve their quality of life and reduce risk of recurrence and a second primary cancer. Other organizations, although not issuing comprehensive cancer survivorship care guidelines, have addressed surveillance for cancer recurrence or late treatment effects among people who have been diagnosed with cancer in the past.17⇓⇓⇓⇓⇓⇓–24
PCPs are the primary audience for some survivorship guidelines, such as those issued by the American Cancer Society.25 Although efforts have been made to promote comprehensive survivorship care guidelines among health care providers, little is known about whether PCPs are aware of these guidelines.25
To further explore this topic, we analyzed questions on Porter Novelli’s DocStyles survey that assess PCP delivery of and confidence in their knowledge of survivorship care. We looked at these topics by types of cancer survivorship care services provided to cancer survivors, use of surveillance and comprehensive survivorship care guidelines from national cancer care and health care organizations, and receipt of survivorship care training.
Methods
DocStyles is an annual web-based survey of US health professionals sponsored by Porter Novelli Public Services. Detailed methodology on DocStyles is listed at https://styles.porternovelli.com/DocStyles/. Briefly, DocStyles covers a variety of health topics, with a focus on the perspectives of PCPs and select other medical specialties. We analyzed the 2019 fall sample, which was administered by Sermo to their Global Medical panelists. Participants were health care providers who have practiced for at least 3 years, actively saw patients during that time, and worked in either an individual or group practice, or hospital setting. Within the panel, sampling quotas were set so that 1000 primary care physicians, 250 OB/GYNs, 250 pediatricians, and 250 nurse practitioners/physician assistants were recruited. To reach selected quotas, 2696 health professionals were initially contacted to participate, resulting in a response rate of 64.9%. Respondents could quit the survey at any time, and no personal identifiers were stored in the study database.
The 2019 fall survey included questions on use of cancer surveillance guidelines for cancer recurrence or management of adverse treatment effects by national medical organizations, use of comprehensive cancer survivorship care guidelines, specific guidelines used, types of care typically provided to post-treatment cancer patients, use of the survivor’s cancer survivorship care plan, confidence level regarding knowledge of cancer-related follow-up care, and receipt of training or instruction within the past 5 years regarding the late or long-term effects of cancer treatment. Participants were asked “The following organizations have issued recommendations for surveillance for recurrence of cancer. Please indicate which organizations you have used to find information on surveillance for recurrence” and “The following organizations have issued comprehensive cancer survivorship care guidelines or recommendations. Please indicate which organizations you have used to find information on cancer survivorship care.” Respondents could choose from a list of national cancer care or medical organizations who have developed either guidelines, practice briefs, or recommendations on these topic areas. To assess receipt of survivorship training, survey respondents were asked “In the past 5 years, have you received training or instruction regarding the late or long-term effects of cancer treatment that cancer survivors may experience over time?” To gather information on typical survivorship care provided, survey respondents were asked “What care do you typically provide to your post treatment cancer survivor patients?” with a list of the most common survivorship care services offered and multiple response options allowed. Use of the survivorship care plan was assessed by asking “How often do you refer to your patients’ survivorship care plans to guide their medical care?” with 5 response options provided, ranging on a Likert scale from 1 (never) to 5 (always), with a “not applicable” option provided. Providers participating in this survey were limited to family physicians, internists, obstetricians and gynecologists (OB/GYNs), physician assistants, and nurse practitioners. Given their low frequency of seeing cancer survivors, pediatricians did not complete the cancer survivorship questions. We also excluded respondents who reported that they did not see any cancer survivors in their practice (n = 79), resulting in a sample size of 1421 respondents.
We created 3 variables to categorize respondents based on: 1) use of any of the named sources for surveillance for recurrence; 2) use of comprehensive survivorship care guidelines; and 3) receipt of training on cancer survivorship. Respondents who indicated they did not use any of the named sources for surveillance for recurrence, comprehensive survivorship care guidelines, or who never received training were categorized as nonusers for each variable. In multivariable analyses, we created an additional variable that classified a respondent who reported using any source for surveillance for recurrence or comprehensive survivorship care as a guideline user, and anyone reporting not using any of the sources as a guideline nonuser.
We examined the percentage of providers who reported they typically provide the following survivorship care to post-treatment cancer survivors: surveillance for cancer recurrence, screening for a new cancer, evaluating late and long-term adverse treatment effects, counseling on smoking cessation, counseling on diet and physical activity, treating anxiety and depression, assessing genetic cancer risk or managing patients with genetic syndromes, treating pain from cancer treatment, treating fatigue, treating sexual dysfunction, or none of these services provided. We also examined confidence in knowledge of the following topics: surveillance for recurrent cancer, screening for other new primary cancers, evaluating patients for adverse late or long-term physical effects of cancer or its treatment, treating pain related to cancer treatment, treating depression and/or anxiety, treating fatigue, or treating sexual dysfunction. Each 1 was measured on a 4-point Likert scale, ranging from very confident, moderately confident, somewhat confident, and not at all confident, with an option to report “do not know” or “not applicable.” We dichotomized responses into very confident/moderately confident versus somewhat/not at all confident based on the distribution of responses.
Descriptive statistics were calculated for demographic characteristics of survey respondents, and use of either guidelines for surveillance for cancer recurrence or comprehensive survivorship care guidelines, and receipt of survivorship care training. We examined the types of survivorship care providers reported delivering and confidence in knowledge overall and by use of guidelines for cancer surveillance for recurrence, comprehensive survivorship care guidelines, or receipt of survivorship training. Due to the number of statistical comparisons, we adjusted the p values obtained from Chi-Square tests for the false discovery rate.26,27 We considered p values < 0.05 as statistically significant.
We created separate multivariable logistic regression models to determine predictors of providing each type of survivorship care service (dependent variables). Independent variables in most of the final models included the following (after eliminating nonsignificant covariates using a backward elimination approach): gender, work setting, years in practice, financial status of most patients within the practice, provider type, number of cancer patients seen per week, receipt of survivorship care training, and use of either guidelines for surveillance for recurrence or comprehensive survivorship care. Potential confounders were retained in the final models if the odds ratios for either guideline use or survivorship care training were changed by more than 10% after their exclusion. Models were also assessed for goodness of fit using the Hosmer-Lemeshow test and for collinearity by examining the variance inflation factor in linear regression models. We repeated the multivariable logistic regression analysis with confidence in knowledge of survivorship care as the dependent variable for each service assessed. Data were analyzed using SAS 9.4 (SAS Corporation, Cary, NC).
Results
Survey respondents were majority male, most commonly aged 50 to 64 years, and 2-thirds reported being non-Hispanic white, with an additional 20% reporting they were Asian or Pacific Islander (Table 1). Most survey respondents saw between 1 to 15 cancer survivors per week and were either family physicians or internists. Most worked in an outpatient group practice and have practiced for less than 20 years. More than 78% of all survey respondents reported using any of the listed sources for surveillance of cancer recurrence, whereas 62% reported using comprehensive survivorship care guidelines, and 18% reported using neither type of guideline (“nonusers”; Table 1). A smaller percentage (17%) of survey respondents reported receiving training on survivorship care. PCPs who received survivorship training reported more frequent use of surveillance for recurrence (92% vs 76%) or comprehensive survivorship care guidelines (85% vs 57%) compared with PCPs without training. Only 4% of PCPs who received survivorship care training did not use any of the guidelines listed. PCPs who reported using comprehensive survivorship care guidelines also saw more cancer survivors on a weekly basis than other PCPs. Slightly fewer internists reported using surveillance for recurrence guidelines compared with other types of PCPs, and nonguideline use was higher among internists. Twenty-three percent of PCPs who always/often referred to survivorship care plans were nonusers of guidelines.
Characteristics of Providers and Use of Guidelines for Surveillance for Cancer Recurrence and Survivorship Care, 2019 Porter Novelli DocStyles Survey
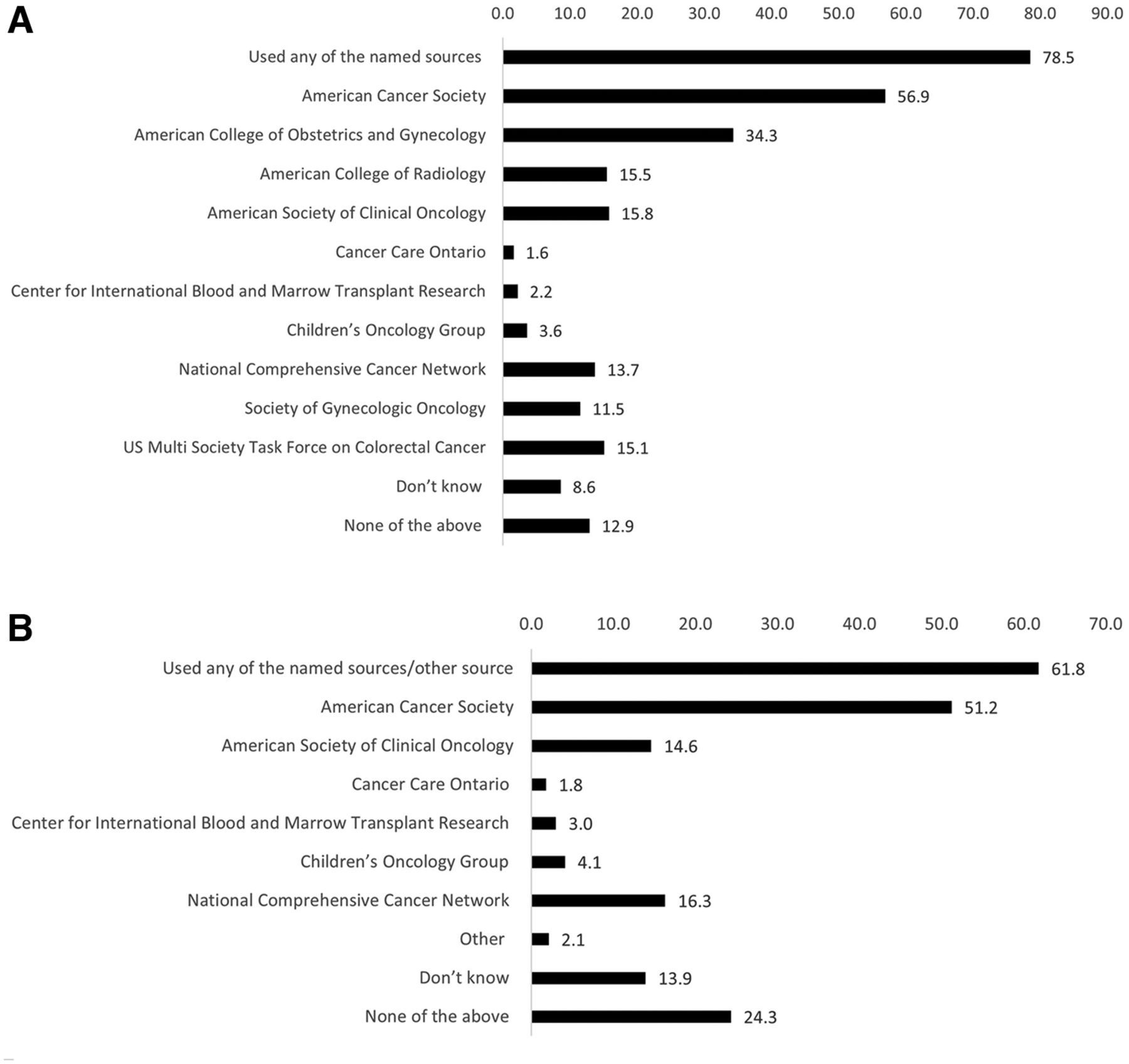
Overall, survey respondents most frequently reported using ACS guidelines for surveillance of recurrence (57%), followed by resources from the American College of Obstetrics and Gynecology (ACOG) at 34%, and less commonly, guidelines from the American College of Radiology and ASCO (Figure 1a). For use of comprehensive survivorship care guidelines, ACS was the most commonly reported source of information (51%), followed by NCCN (16%), and ASCO (15%, Figure 1b). Few PCPs reported using guidelines issued by Cancer Care Ontario, Children’s Oncology Group, or the Center for International Blood and Marrow Transplant Research.

(A) Use of guidelines that include recommendations for surveillance of cancer recurrence from national medical organizations, Porter Novelli DocStyles survey, 2019. (B) Use of comprehensive cancer survivorship care guidelines from national medical organizations, Porter Novelli DocStyles survey, 2019.
PCPs most frequently reported providing counseling on smoking cessation (66%), treating depression/anxiety (62%), or counseling on diet/physical activity (59%), followed by surveillance for cancer recurrence (57%, Table 2). Fewer PCPs overall reported treating sexual dysfunction among cancer survivors (40%) or assessing genetic risk (26%). Providers who ever referred to either surveillance for recurrence or comprehensive survivorship care guidelines more frequently reported providing these services to cancer survivors than providers who did not. PCPs who ever referred to surveillance for recurrence guidelines had substantially higher levels of surveillance for cancer recurrence (61%) compared with PCPs who did not use them (43%). They also more frequently assessed for genetic risk (29% vs 13%) or treated sexual dysfunction (43% vs 29%). Providing each specific survivorship care service was also higher among PCPs who reported using comprehensive survivorship care guidelines. These providers had significantly higher levels of surveillance for cancer recurrence (63% vs 47%), screening for a new cancer (55% vs 47%), and assessing late and long-term treatment effects (45% vs 33%), compared with providers who never used any of these specific guidelines on comprehensive survivorship care. Having received survivorship care training on late and long-term treatment effects was also associated with providing survivorship care services, with the exception of smoking cessation counseling and screening for new cancers. Notably, this group of PCPs more frequently assessed for late and long-term treatment effects (60% vs 36%), treated pain (58% vs 38%) and fatigue (55% vs 37%), and assessed genetic risk (38% vs 23%), compared with PCPs who reported not receiving training within the past 5 years.
Types of Survivorship Care Provided by Survivorship Care Guideline Use and Training, 2019 Porter Novelli DocStyles Survey
Overall, the percentage of providers feeling very/moderately confident in knowledge of survivorship care ranged from 77% for treating depression to 58% for treating pain or assessing late and long-term treatment effects (Table 3). Use of any guidelines and having received training were associated with greater confidence in knowledge of survivorship care for nearly all topic areas. PCPs using surveillance for recurrence guidelines had higher confidence levels for surveillance for recurrence (68% vs 54%), treating pain (61% vs 48%), treating fatigue (63% vs 50%), and treating sexual dysfunction (63% vs 51%). Similarly, users of comprehensive survivorship care guidelines reported statistically significantly higher confidence in their knowledge of all types of survivorship care services, compared with nonusers of those guidelines. Differences were substantially higher for assessing late and long-term treatment effects (65% vs 47%), treating pain (65% vs 46%), and treating fatigue (67% vs 49%) compared with nonusers. PCPs who had received survivorship training reported very/moderate confidence levels for all services except screening for new cancers, compared with PCPs without training. The percentage of PCPs receiving training who reported very/moderate confidence levels ranged from 83% for treating depression to 67% for treating sexual dysfunction.
Confidence in Providing Survivorship Care by Survivorship Care Guideline Use and Training, 2019 Porter Novelli DocStyles Survey
In multivariable logistic regression analyses, reported use of any surveillance for recurrence or comprehensive survivorship care guideline was associated with providing each specific survivorship care service, with the exception of treating fatigue (Table 4). Notably, PCPs using any guideline were 2 times more likely to assess for genetic risk (OR = 2.65 95% CI (1.68, 4.17)) or screen for recurrence (OR = 2.32 95% CI (1.70, 3.18)) compared with nonusers. Having received training was associated with evaluating late and long-term treatment effects (OR = 2.30, 95% CI (1.69, 3.12)), and an approximately 2-fold increased odds for providing care for pain, fatigue, sexual dysfunction, and assessing genetic risk, and increased the odds 1.5 times for providing surveillance for recurrence.
Predictors of Providing Survivorship Care by Topic Area, 2019 Porter Novelli DocStyles Survey
In a separate set of multivariable analyses, PCPs who reported using any guideline were more likely to report being confident in knowledge of survivorship services, with the exception of treating sexual dysfunction (Table 5). The largest effects were for treating pain (OR = 2.18 95% CI (1.57, 3.03)), fatigue (OR = 2.14 95% CI (1.56, 2.95)) and screening for recurrence (OR = 2.11 95% CI (1.52, 2.92)). PCPs who receiving survivorship care training also were more likely to report being confident in knowledge of all types of survivorship care, although findings for treating depression and screening for new cancers were not statistically significant. Notably, PCPs with survivorship training were 2 times more likely to report being confident in assessing late and long-term treatment effects (OR = 2.32 95% CI (1.66, 3.26)).
Predictors of Confidence* in Providing Survivorship Care, 2019 Porter Novelli DocStyles Survey
Discussion
Use of either guidelines for surveillance of recurrence or comprehensive survivorship care were relatively high among PCPs, although few reported receiving training on late and long-term treatment effects of cancer within the past 5 years. Compared with nonusers of guidelines, use of either surveillance for recurrence or comprehensive survivorship care guidelines was associated with higher levels of providing survivorship care services across a range of topics, and PCPs using them reported higher levels of confidence in their knowledge of survivorship care. In addition, having received training was particularly associated with providing survivorship care services and confidence in knowledge of survivorship care. PCPs most often reported providing tobacco cessation and nutrition/physical activity counseling, treating depression, and conducting surveillance for recurrence among cancer survivors. These findings align with the role that PCPs may have in providing counseling and referrals to prevent other chronic health conditions, such as those related to obesity and lack of physical activity.28,29 However, gaps in survivorship care remain with many topic areas, with one-third to three-quarters of providers reporting they do not typically provide these services. Topics such as assessing genetic risk and late and long-term treatment effects, and treating sexual side effects, pain, and fatigue were least commonly reported services that were provided.
Our findings are somewhat similar to a study conducted in 2016 in Pennsylvania that found many PCPs were fairly confident in assessing adverse effects of cancer treatment, such as fatigue, depression, anxiety, and generalized pain, but having additional education and training helped with knowledge gaps.10 However, only approximately 17% of PCPs at the time that study was conducted were aware of the ACS breast cancer survivorship care guideline. We found that 51% of PCPs were aware of any ACS survivorship care guideline, and 28% reported familiarity with the ASCO/ACS breast cancer care guideline (data not shown). Given that 20% - 40% of PCPs did not feel very confident in their knowledge across topic areas, our findings point to the importance of training opportunities for PCPs on survivorship care. In addition, training for PCPs to assist with the maintenance of guidelines may be beneficial. Maintaining guidelines can be challenging for nonprofit organizations with limited resources and an ever-growing body of scientific literature to keep up with. In these situations, medical specialty organizations may consider using care guidelines of other organizations, or to partner with them to help with dissemination. Organizations that are familiar to and deemed trustworthy by PCPs may prefer to summarize existing care guidelines on their web sites and point clinicians to trustworthy resources.
Based on our findings, some care topics continue to remain challenging for PCPs to deal with, such as assessing for genetic risk, treating pain, and addressing sexual problems. A team-based care approach may be 1 strategy to ensure cancer survivors receive optimal care, given the burden placed on PCPs to deal with a variety of issues with their patients.30,31 Although PCPs may need to recognize and screen for specific conditions, a team-based approach can help with optimally treating patients by referring them to other health care professionals on the team, including team members with specialized training on specific topic areas. For example, a PCP could assess for psychosocial distress using a standardized tool, and then refer patients to an appropriate mental health professional, similar to the practice in many oncology settings.32,33 As well, patient navigators or community health workers (CHWs) can help patients make follow up appointments, obtain transportation, and overcome other barriers to care.34,35 Other team-based approaches that integrate PCPs into the oncology care team using scalable, less resource intensive methods may be another promising approach.36
Health information technology might help support PCPs in providing survivorship care.37⇓⇓–40 Well-designed clinical decision support tools integrated into electronic health records (EHR) could provide a summary to PCPs of the patient’s cancer diagnosis, and alert PCPs on recommendations for survivorship care based on current guidelines.37,39,40 Information technology and EHR resources can significantly reduce the time and manual effort needed to create or update survivorship care plans.41 Pulling data from EHRs to create more tailored plans may also increase patient adherence to behavior change interventions.42 User-friendly patient portals could also be harnessed to deliver interventions.43
These findings may also inform future roles for public health in survivorship care. For a number of years, the Centers for Disease Control and Prevention (CDC)’s National Comprehensive Cancer Control Program (NCCCP) has worked with national partners and funded jurisdictional cancer control programs to form partnerships, develop cancer control plans, prioritize survivorship as a program priority, and implement interventions.44 This work may be most salient in geographic areas where there are a greater number of people who are medically underserved. In these areas, PCPs may often be the main point of contact for survivors, rather than an oncologist. Specific areas the NCCCP has shown may be helpful are equipping PCPs with advanced skills in managing cancer survivors in their caseloads through participation in Project ECHO and other types of learning collaboratives,34 and increasing knowledge through an online e-learning series on cancer survivorship care topics.45
This study had several notable limitations and strengths. We are unable to generalize the study findings to all practicing PCPs in the United States, given that we used a panel survey based on a convenience sample. In addition, PCPs self-reported the types of survivorship care services they provided, which could be overreported due to social desirability bias. Due to survey space limitations, not all medical organizations that may be issuing surveillance guidelines for cancer recurrence or that address limited topics may have been included. We also could not assess how often specific survivorship care services were offered to patients, or whether survivorship care services were provided to all cancer survivors or only a subset of them. In addition, the survey only asked PCPs about their current practice area, but not prior practice experiences, where they may have obtained different trainings or been exposed to advanced models of survivorship care. In addition, future qualitative studies could build on our findings and further explore the depth of survivorship care provided and how specific tools might support PCPs in delivering care. However, a strength of this study is the sample size of PCPs included, which allowed us to examine specific survivorship care services being provided and confidence in knowledge of various aspects of survivorship care. We extend previous findings of other studies by providing a contemporary look at survivorship care among PCPs and use of specific care guidelines.
Conclusion
Our findings reaffirm and extend the knowledge that survivorship care guidelines and training are associated with PCPs providing a range of survivorship care services, including more complex topics like long-term and late treatment effects, and assessing genetic risk. Although many PCPs report typically delivering survivorship care and feeling confident in their knowledge of topic areas, substantial percentages of PCPs reported they did not. Care guidelines and trainings that are maintained and accessible to providers may help PCPs deliver high quality survivorship care services.
Acknowledgments
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Notes
This article was externally peer reviewed.
Conflict of interest: We have no conflicts of interest to declare.
Funding: We have no funding sources to report. This work was completed as part of routine United States federal government employee duties.
Acknowledgments: The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
To see this article online, please go to: http://jabfm.org/content/36/5/789.full.
- Received for publication January 30, 2023.
- Revision received April 21, 2023.
- Accepted for publication May 1, 2023.




{kind=link}