
Abstract
Background: Recent attention and focus on, antiracism training in health care has potential to accelerate our path to social justice and achieve health equity on a national scale. However, theoretical frameworks and empirical data have yet to emerge that explain the uptake of antiracism trainings and their efficacy.
Objective: This goal of this study was to test hypotheses regarding uptake of antiracism training in Family Medicine departments using Diffusion of Innovation Theory.
Methods: In 2021, we incorporated 10 survey items in the Council of Academic Family Medicine Educational Research Alliance's national omnibus survey for Department of Family Medicine Chairs (n = 104). We used DOI (Diffusion of Innovation) attributes (ie, relative advantage, compatibility, complexity, trialability, and observability) as a guiding framework to assess perceived innovation of antiracism training. We also evaluated the mode of training (eg, didactic, experiential) and whether any subsequent policy or practice-level antiracist actions occurred. We used c2 tests to examine associations between DOI attributes and antiracist actions; and logistic regression to determine odds of association.
Results: Ninety-two percent of respondents indicated antiracism training was happening in their department. Relative advantage, compatibility and observability were positively associated with antiracist actions, P < .05. Perceived relative advantage was associated with implementation of antiracist action (OR 1.94, 1.27-2.99). Complexity and trialability were not statistically significantly associated with action.
Conclusion: Our findings provide evidence of DOIs influence on antiracism uptake in Departments of Family Medicine. We believe our findings can facilitate the future implementation of antiracism training activities and actionable antiracist policies and practices.
- Chi-Square Test
- Diffusion of Innovation
- Family Medicine
- Health Equity
- Health Policy
- Logistic Models
- Social Justice
- Surveys and Questionnaires
Background
Antiracism refers to thoughts or practices that seek to confront, eradicate, and end racism.1 The practice of institutional antiracism requires institutions to dismantle structural racism and shift power through mechanisms, that is, funding, policies, processes, leadership, and culture—so that individuals who have been historically marginalized and minoritized have equitable access to opportunities supporting health and advancement.2 For example, some academic health centers have implemented systematic strategies to remove bias in processes for faculty recruitment, retention, advancement and student matriculation.3 This is can also include antiracism training to identify, address and measure progress toward mitigation.4
Antiracism training gained increased popularity and attention with Ibram X. Kendi's 2019 book entitled “How to Be an Antiracist,”5 published during the recent period of civil unrest regarding racist practices. Increased attention on antiracism training may accelerate our path to social justice and achieving health equity on a national scale, particularly in primary care. In a recent scoping review of the literature, Hassen et al found a range of antiracism training activities across different health care settings and clinician groups. Only 14% of the trainings occurred in primary care settings and only 11% occurred in the US.6 Data are lacking about the barriers and facilitators to uptake of such training.
We used Rogers' Theory of Diffusion of Innovation (DOI) to test our hypotheses related to the uptake of antiracism training in Departments of Family Medicine (DFM). According to the theory, 5 user-perceived attributes influence uptake of an innovation (relative advantage, compatibility, complexity, trialability, and observability).7 To the extent that an innovation is seen as beneficial (relative advantage), value-aligned (compatibility), usable (low complexity), scalable (triability), and measurable (observability), it becomes adopted. We surveyed DFM Chairs to determine if DOI attributes were associated with likelihood of antiracism training and the implementation of DFM antiracist policies or practices. We hypothesized that higher scores on DOI attributes would be associated with greater uptake of training and implementation of policies or practices.
Methods
Study Design
We developed 10 questions included in a larger omnibus survey conducted by the Council of Academic Family Medicine Educational Research Alliance (CERA). The methodology for the CERA has been previously reported.9
Subjects
The survey was emailed to 192 DFM Chairs in the US using Survey Monkey software from August 6 to August 31, 2021. The project was approved by the American Academy of Family Physicians (AAFP) Institutional Review Board.
Survey Items
The survey included items related to Chair demographics and their program's characteristics. Chairs were asked to report whether they conducted any antiracism training in the past year and how it was conducted (didactic, experiential, or both).
DOI Attributes (Primary Independent Variables)
One question for each of the 5 DOI attributes (relative advantage, compatibility, complexity, triability, and observability) was used as a guiding framework (appendix).
DOI questions were scored using a 7-point Likert scale ranging from 1 to 7 with higher scores indicating higher proclivity for the attribute.
Adoption of Antiracist Policies or Practices (Primary Dependent Variable)
Chairs reported departmentally instituted antiracist policies or procedures as a result of the training using a dichotomous response option (yes/no).
Analyses
Data were analyzed using STATA 16 (Stata Corporation: College Station, TX). Descriptive analyses and χ2 tests were used to determine if the DOI attributes, Chair demographics, or program characteristics were associated with antiracism training or implementation of antiracist policies or practices (see Table 1). Subsequently, a multivariable logistic regression was employed to estimate how much the DOI attributes were associated with implementation of antiracist policies (see Table 2). A p-value of <0.05 level was used to determine statistical significance.
Department and Program Chair Characteristics
Results of the Logistic Regression Model: Odds of Implementing Antiracist Policies or Practices
Results
The response rate was 54.17% (104/192). Chairs were primarily male (66%), served as Chair for 6 years, and 88% ≥age 50 years. Their residency programs were primarily community-based (82%). Sixteen percent reported 31% or more of their faculty were underrepresented minorities in medicine (URiM).
Ninety-two percent had or planned antiracism training and members of their department or institution (40%) were most likely to lead the training. Sixty-four percent reported their department implemented antiracist policies or practices because of the training. Only 6% of Chairs reported no training and had no plans to do so.
Factors Associated with Implementation of Antiracist Policies or Practices
Departments that implemented antiracist policies or practices scored higher on the DOI agreement scales. For example, 64% of those that implemented practices agreed (somewhat agreed, agreed, or strongly agreed) the training results would be observable; compared with 24% of those that did not (see Figure 1).
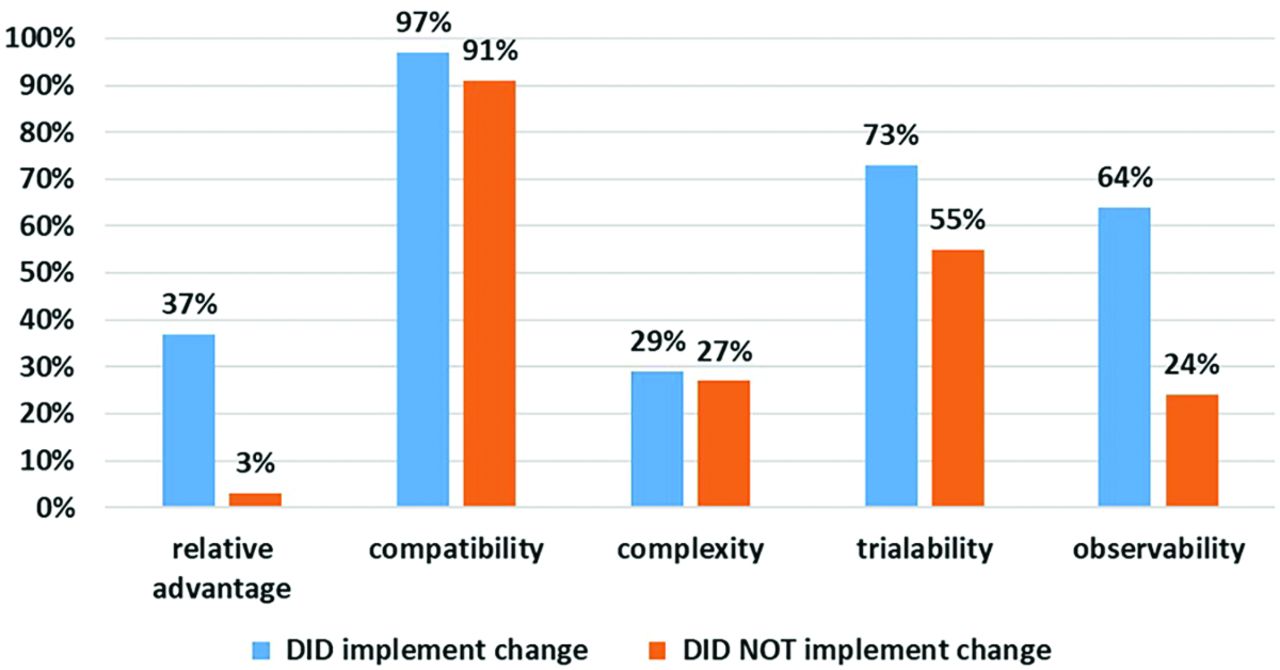
Total percentages of those that agreed (somewhat agreed, agreed, or strongly agreed) the respective attributes of innovation (relative advantage, compatibility, complexity, trialability, observability) were important for antiracism training. We grouped the results by those that reported they did implemented antiracist policies and or practices vs. those that did not.
Relative advantage, compatibility and observability were positively associated with making changes as result of the antiracism training, P < .05 (see Figure 2).
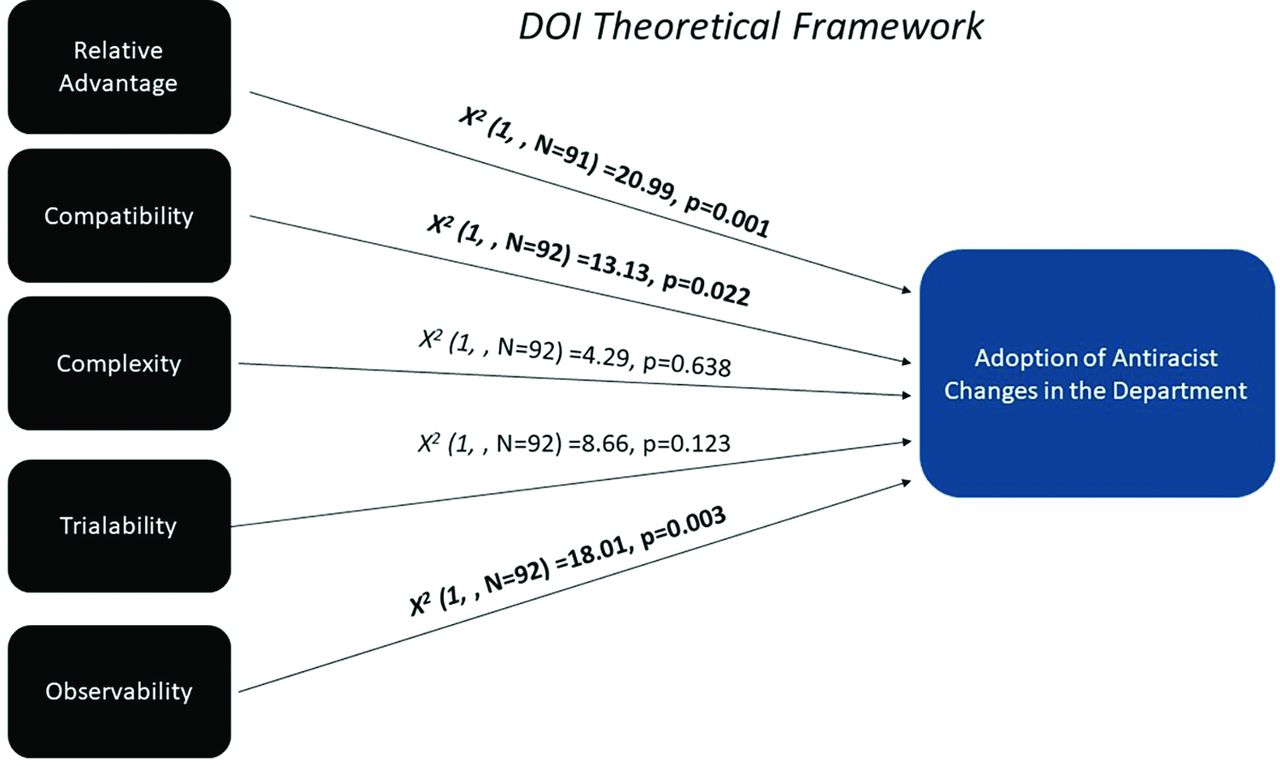
χ2 analyses showing that relative advantage, compatibility and observability were positively associated with making changes as result of the antiracism training.
In our multivariable logistic regression model, higher scores on relative advantage, compatibility, and observability were associated with increased odds of implementing antiracist actions in the department (see Table 2).
Discussion
This study provides partial confirmation that DOI predicted uptake of antiracism training, policies, or practices. Higher scores on perceived relative advantage, compatibility and observability predicted implementation of antiracist policies or practices. Of note, not all the DOI attributes are necessary to sustain an innovation.10 Almost all DFM provided some antiracism training, with most providing a combination of didactic and experiential learning experiences. Multimodal learning has been linked to greater knowledge retention among health care professionals.11,12
It has been over 20 years since Dr. Camara P. Jones called for a national conversation about the impact of racism on public health.13 The call has recently been answered via declaration of racism as a public health crisis from prominent US health organizations including the Centers for Disease Control & Prevention (CDC), the American Medical Association, and the American Public Health Association.14⇓–16 In fact, the CDC is an integral part of the H.R. 666 Anti-Racism In Public Health Act of 2021 introduced to Congress by Rep. Ayanna Pressley to mitigate racism and its impact on health and well-being.17 Given the national attention, DFM leaders may have already understood antiracism training is complex and necessary, thus, thwarting our ability to detect a difference in complexity and trialability. However, we cannot rule out our modest sample size may have limited our power to detect differences.
Surprisingly, we did not find associations between Chair and program characteristics with antiracist training, or the development of policies or practices. In DOI, an organization's structure is associated with uptake of an innovation.18 For that reason, we expected their characteristics would be significant predictors. However, there may be unassessed characteristics for mediating relationships, such as broader institutional resources or politics. Future studies should explore this assumption. The distribution of race, sex and ethnicity of our study sample were similar to national estimates.31
Concerns of “performative allyship” in antiracism training have been previously raised.19,20 As such, the importance of action, beyond training, is critical. However, we are encouraged by the number of Chairs that reported implementation of antiracist practices or policy changes. We are hopeful this signals a cadre of who might be considered “antiracist long-haulers” – those invested in and committed to the work needed to dismantle racism. There are a growing number of antiracism models, tools and learning kits, particularly suited for DFM, to help sustain such efforts.21⇓⇓–24
Study Implications
A major strength of our study is that it uses the DOI theoretical underpinnings to understand how and why some DFM engaged in antiracist training and enacted policy or practice-level changes. Our findings can be used to support DFM contemplating such training and to guide those planning to implement antiracist work in their own departments by focusing on the DOI attributes to facilitate adoption.25 For example, relative advantage was significantly associated in our model and had the largest difference in innovation agreement scores among those who implemented antiracist action (37%) versus those that did not (3%). It may behoove DFM to focus on explicitly aligning their mission and vision to be reflective of antiracist principles, and act on them accordingly.26
Limitations
We note a few limitations. First our sample size (n = 104) and response rate (54.12%) were modest, potentially limiting our power to detect statistical differences.27 Our sample may not fully represent DFM residency programs (n = 707) currently listed on the AAFP website,28 which may limit the generalizability of our findings. Second, our DOI scale was developed de novo. Data were self-reported and limited potentially, by social desirability. There are currently no validated scales to measure DOI for antiracism. Our survey seems to exhibit good face-validity, but we cannot rule out sampling or measurement errors.29,30 Finally, our data did not allow us to explore the type, impact, quality or quantity of antiracism training activities, policies or practices that were implemented in the respective DFM. Future studies should explore these important outcomes.
Conclusion
The majority of our DOI associations were confirmed, and our findings support the credibility of DOIs influence on antiracism uptake in DFM. Our findings can be leveraged to implement antiracism training activities that may translate to actionable and impactful antiracist policies and practices.
Acknowledgments
The authors would like to thank Kathleen Silver for her assistance with submission of this article.
Notes
This article was externally peer reviewed.
Conflicts of interest: None.
Funding: None.
To see this article online, please go to: http://jabfm.org/content/35/4/803.full.
- Received for publication November 23, 2021.
- Revision received December 15, 2021.
- Revision received February 2, 2022.
- Accepted for publication February 8, 2022.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Response: Re: Evaluating the Uptake of Antiracism Training, Policies, and Practices in Departments of Family Medicine
- Re: Evaluating the Uptake of Antiracism Training, Policies, and Practices in Departments of Family Medicine
- Family Medicine Researchers Explore the Social Determinants of Health, COVID-19 Issues, and Cancer Survivor Care