
Abstract
Purpose: The purpose of this study was to assess ordering of human papillomavirus (HPV) testing for normal cervical cytology among low-risk women aged 30 to 65 years.
Methods: Audits of 833 cytology request forms for low-risk women completing a Papanicolaou smear, from January 2008 to April 2011, from 5 Michigan family medicine clinics determined HPV orders completed by the clinician performing the Papanicolaou smear. Multivariate logistic regression models examined differences in HPV test ordering by patient age at Papanicolaou test, provider status and sex, and clinic across sites. A Poisson regression model analyzed the annual number of HPV test orders over time.
Results: Cytology requests were completed by 622 faculty (75%), 169 residents/fellows (20%), and 42 nurse practitioner/physician assistants (NP/PAs) (5%). HPV testing for any cytology result was ordered on 324 request forms (39%) by residents/fellows (48%), faculty (38%), and NP/PAs (10%). Female providers were twice as likely as men to order HPV testing for any cytology result across all clinics and provider statuses (P < .001). There were significant differences in HPV test ordering among clinics. Between 2008 and 2011 annual cytology requests increased 46%, including HPV testing for any cytology result after adjusting for faculty provider sex.
Conclusion: HPV test ordering when cytology is collected varied by clinic and provider status and sex. HPV co-testing for any cytology result remains modest, but is increasing over time in these clinics.
For years, the primary cervical cancer screening method has been clinician-collected cervical cytology, or the Papanicolaou smear. In 2000, the US Food and Drug Administration approved the use of HPV DNA testing to triage abnormal cytology results known as atypical squamous cells of uncertain significance (ASCUS). In March 2003, the Food and Drug Administration added a second indication of HPV DNA testing for primary screening in combination with the Papanicolaou smear in women older than age 30 years.1 Cervical cancer screening guidelines from April 2002 to February 2004 generally agreed and supported the combination of cytology and HPV DNA testing as an option for women ≥30 years old.2 Current cervical cancer screening guidelines endorsed by the US Preventive Services Task Force, American Society of Colposcopy and Cervical Pathology, American Cancer Society, and the American College of Obstetrics Gynecology recommend either (1) cytology alone every 3 years in women 21 to 65 years of age or (2) combined cytology and HPV DNA testing in women 30 to 65 every 5 years.3,4
There are limited data about HPV DNA testing practices. In a 2002 survey of 651 American Congress of Obstetricians and Gynecologists fellows, almost two-thirds (65.1%) order HPV testing, usually for reports of ASCUS.5 In 2003, 64% of 213 practicing obstetrician/gynecologists reported they would not adopt triennial Papanicolaou smear plus HPV DNA screening.6 In 2004, of 4305 clinicians who offer Papanicolaou testing, 21% used HPV DNA tests as an adjunct to Papanicolaou smears for screening.7 Among 950 primary care physicians who recommended HPV co-testing in a 2006 survey, only 19% reported that they would extend the screening interval to 3 years with a normal Papanicolaou smear and negative HPV test; the remaining percentage would continue to perform Papanicolaou smears more frequently.8 From 2001 to 2006, there was a 2-fold increase in the use of HPV testing among Florida Medicaid beneficiaries older than age 30 years, but only 26% of HPV DNA tests were used appropriately for screening in women older than age 30 years and only 31.1% were appropriately used to triage ASCUS cytology.2 In one academic center using pathology data from 2004 to 2007, the proportion of HPV testing with normal Papanicolaou smears among patients older than age 30 was 7.8%, and the highest proportion observed was 15% in 2006 compared with 100% for ASCUS triage.9 Neither the Florida study nor the pathology database study ascertained women's risk for cervical cancer or the interval of screening.2,9
The goal of this study was to assess the ordering practices for HPV testing for normal cervical cytology over time for routine cervical cancer screening in low-risk women ages 30 to 65 years among family medicine providers within a community-based, academic-affiliated setting.
Methods
The cytology request forms of low-risk women from 5 family medicine clinical sites were obtained through the university's data warehouse. Low-risk patients were defined as women aged 30 to 65 years with no prior abnormal Papanicolaou smears, no prior colposcopy, no gynecology-oncology history, and no prior hysterectomy and who were not pregnant. This was determined by data on the cytology request form. For any forms with missing data, the woman's medical record was reviewed to determine low-risk status (this occurred in <5% of cases). A single woman could have had her cytology form audited more than once, but only if it was done by a different provider. Cytology and HPV testing were ordered by providers, including faculty, residents/fellows, and nurse practitioners/physician assistants (NP/PAs) between January 2008 and April 2011. In this academic institution, the cytology request forms allowed providers to order HPV testing for any cytology result (referred to as “all results”), “ASCUS only,” or “all atypical/abnormal results.” If left blank, then no HPV testing was done. The forms were audited by a single auditor (MTR), with a random 10% (n = 83) done a second time and blinded to the reviewer. All the double-entry audits were reviewed by an expert medical auditor outside of the research team for arbitration. Of the 83, only 10 were found to have discrepancy and subsequently changed by arbitration. This study's definition of co-testing applied to only low-risk women between the ages of 30 to 65, where the focus was on ordering HPV testing for normal cervical cytology. Among the available cytology request options mentioned above, all results best indicated ordering HPV testing for normal cervical cytology. All 5 family medicine clinic sites (A–E) were included. No other data on providers, patients, or clinics were collected.
We used descriptive statistics followed by univariate comparisons to examine the data between clinics, provider status, and provider sex, using χ2 or t tests as appropriate. This was followed by analysis of variance for age at time of cytology by clinic. We then used a multivariate logistic regression with the outcome of HPV testing ordered for all results to determine significant associations between age at Papanicolaou, provider status (faculty vs. residents/fellows vs. NP/PAs), and provider sex between the 5 clinical sites. Two of the clinics (A and B) were teaching sites with a combination of residents and faculty, whereas the other 3 clinics (C, D, and E) were faculty-only sites. Fellows were equally distributed among all 5 clinics. Comparisons between the 2 clinics with combined faculty and residents and between the 3 faculty-only clinics was performed using separate logistic regression models. The predictor variables of interest a priori for both models were provider sex, provider status (faculty vs. resident/fellow), age at time of Papanicolaou, and year of Papanicolaou. The percent of cytology request forms selecting HPV for all results was plotted over the 4 years of observation to ascertain changes in the frequency of HPV ordering for all cytology results by faculty. There was not enough data on residents/fellows or NP/PAs to examine changes over time. The annual number of HPV tests ordered for all results was analyzed as a Poisson regression model with faculty sex, year of Papanicolaou, and average age of patients seen by the provider in the year as covariates. Natural logarithm of the number of cytology requests by a provider in a given year was used as the offset. We used a generalized estimating equations approach to adjust for the clustering between years within a provider. An unstructured covariance matrix then was used to yield a robust analysis. In all the analyses, we assumed each physician's order for HPV testing for a patient was independent of orders for HPV testing for their other patients. To verify this assumption, the analysis was repeated assuming each clinician's HPV test ordering for each patient was not independent but clustered by provider and clinic. The clustered analysis was not presented since the results were the same. All analysis was done using SPSS statistics version 20 (IBM, Chicago, IL). Before data collection, the university's institutional review board approved the study as exempt human subject research; therefore informed consent was waived.
Results
The cytology request forms of 55 faculty, 37 residents/fellows, and 5 NP/PAs were audited. Among the 833 cytology requests, faculty completed 622 (75%), residents/fellows completed 169 (20%), and NP/PAs completed 42 (5%). HPV was ordered for “all results” on 324 request forms (39%). All the NP/PAs were women. There were 26 female faculty (47%) and 29 female residents/fellows (78%).
Age at Papanicolaou
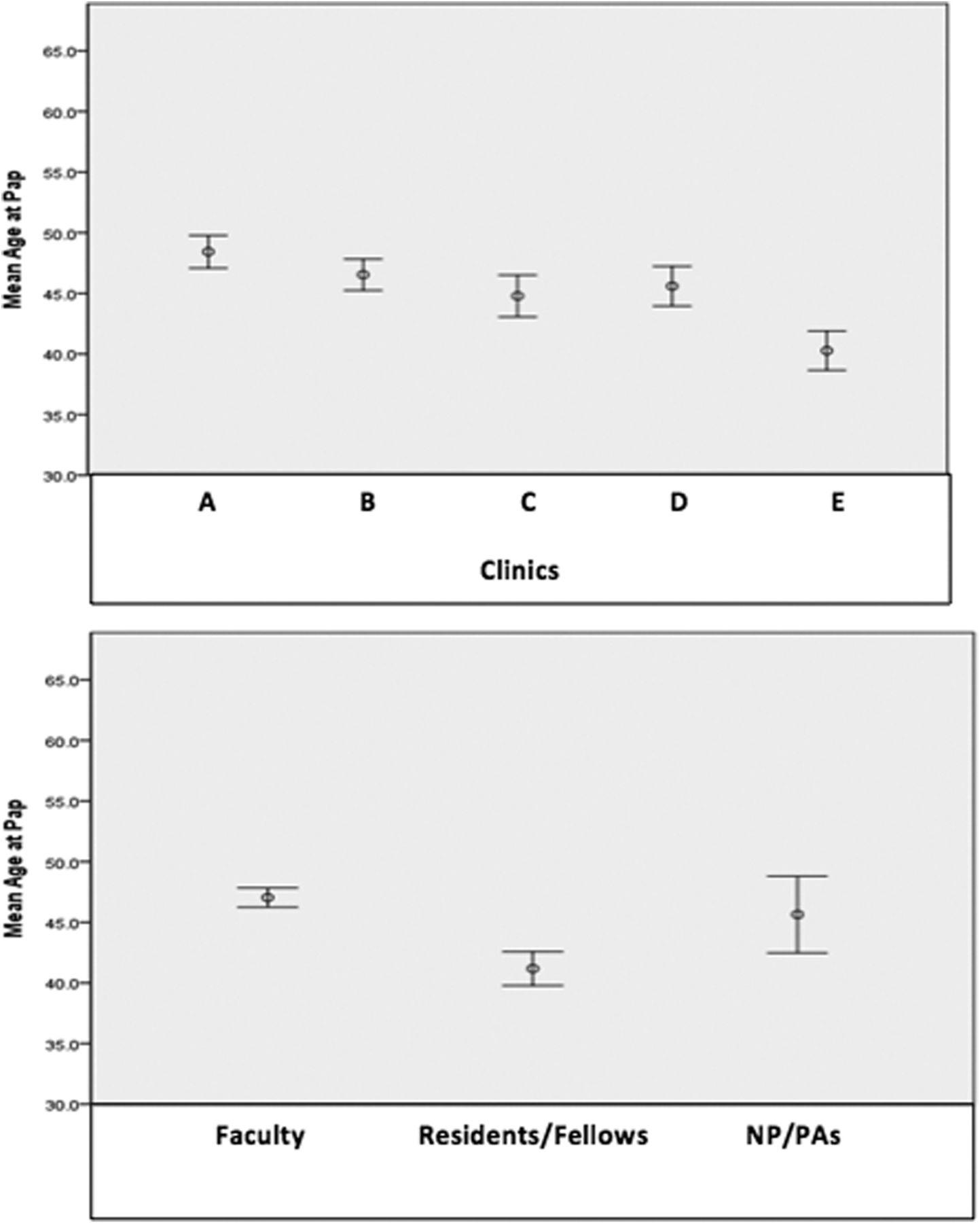
Clinic E had a significantly lower patient age at time of Papanicolaou (P = .001). The residents/fellows' sample of patients was significantly younger than those of the faculty and NP/PAs (P = .05), as noted in Figure 1.

Age of patient at time of cervical cytology collection (Papanicolaou smear [Pap]) by clinic and provider status, with 95% confidence intervals.
Provider Status
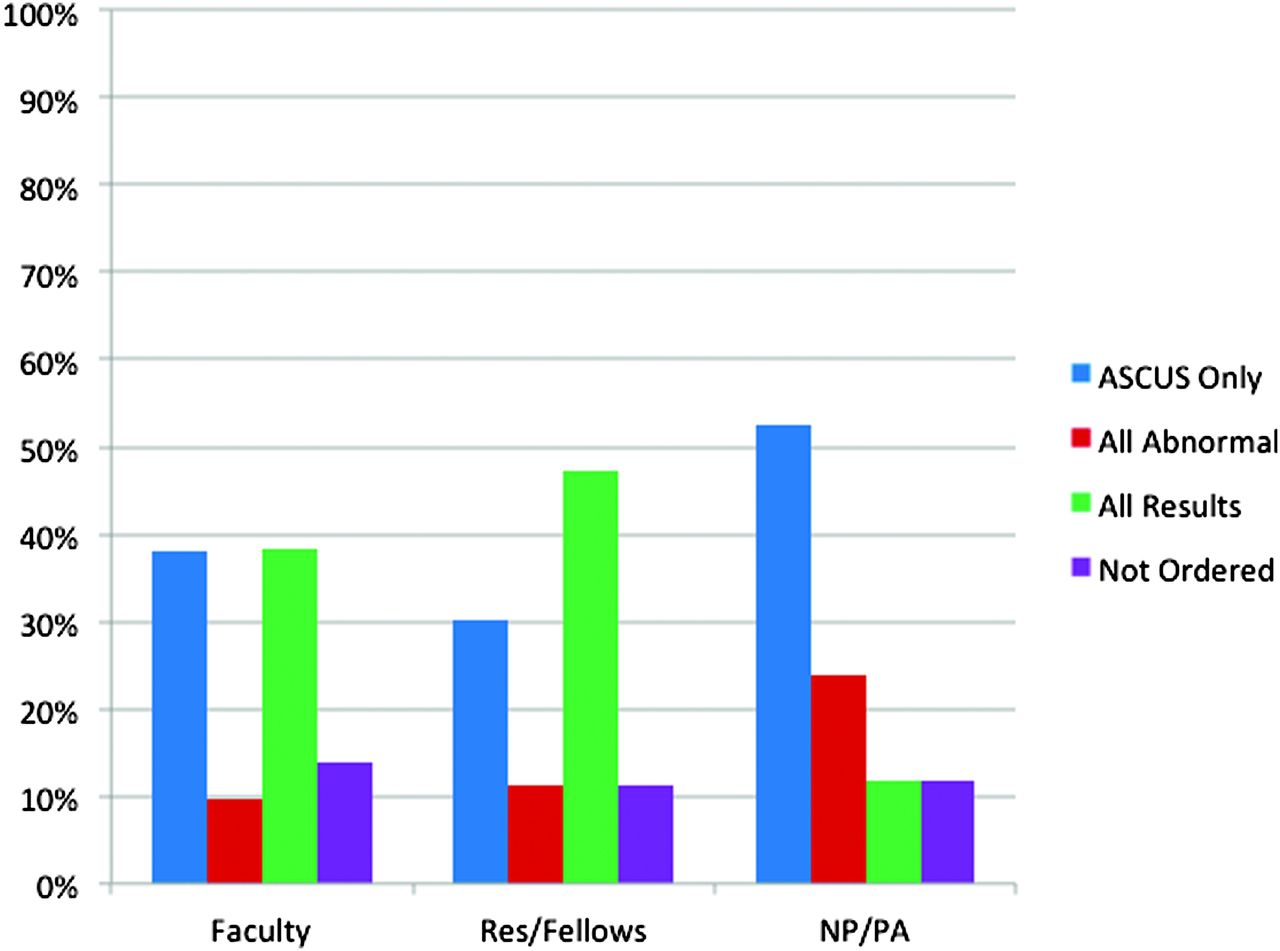
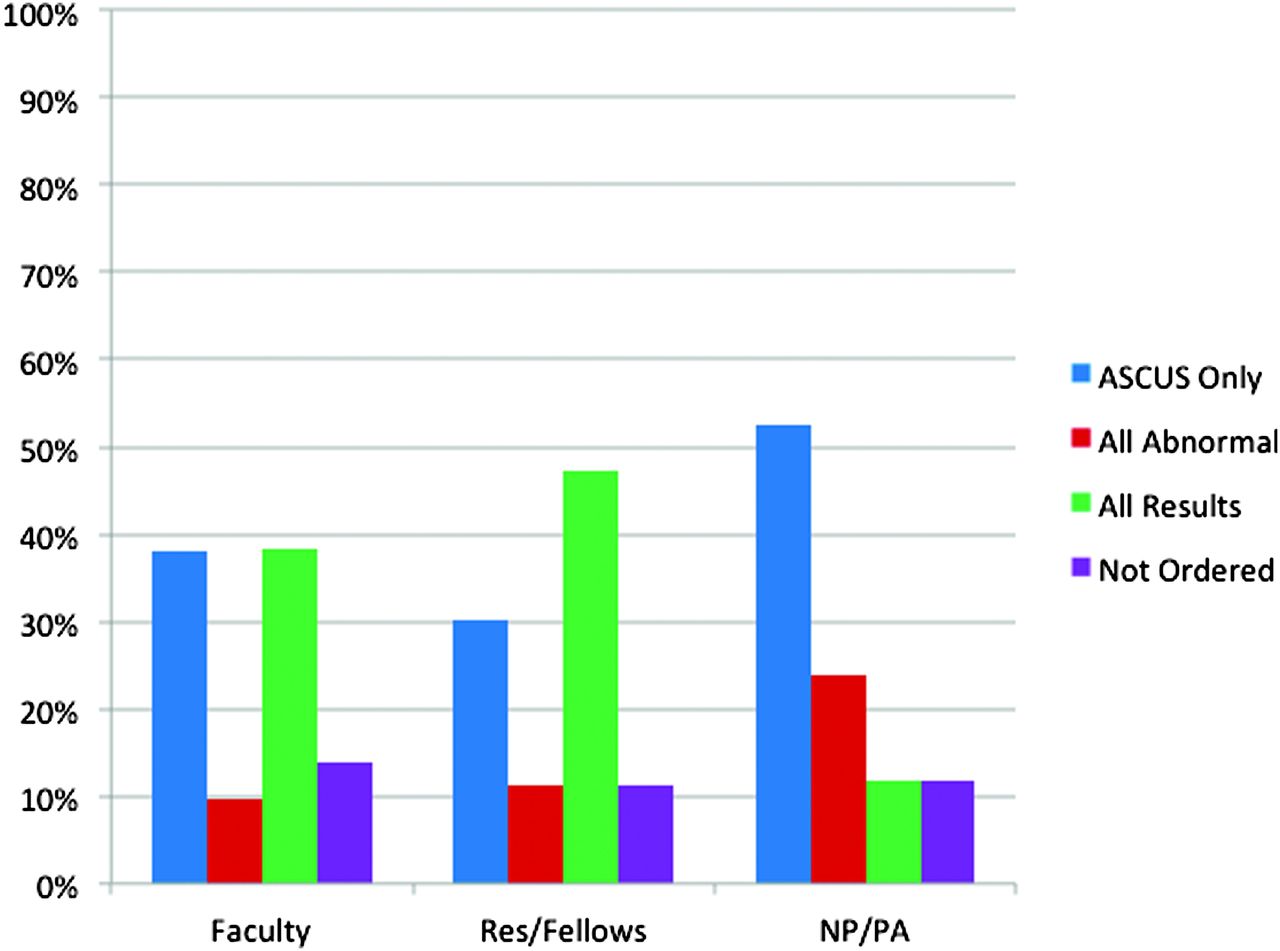
Across all clinic sites, the majority of faculty and residents/fellows order HPV testing for all results (Figure 2). Residents/fellows were significantly more likely (P < .001) to order HPV testing for all results than faculty and NP/PAs. In contrast, the NP/PAs were significantly more likely (P < .001) to order HPV testing for ASCUS only compared with faculty and residents/fellows.
Human papillomavirus testing order by provider status (P < .001).
Provider Sex
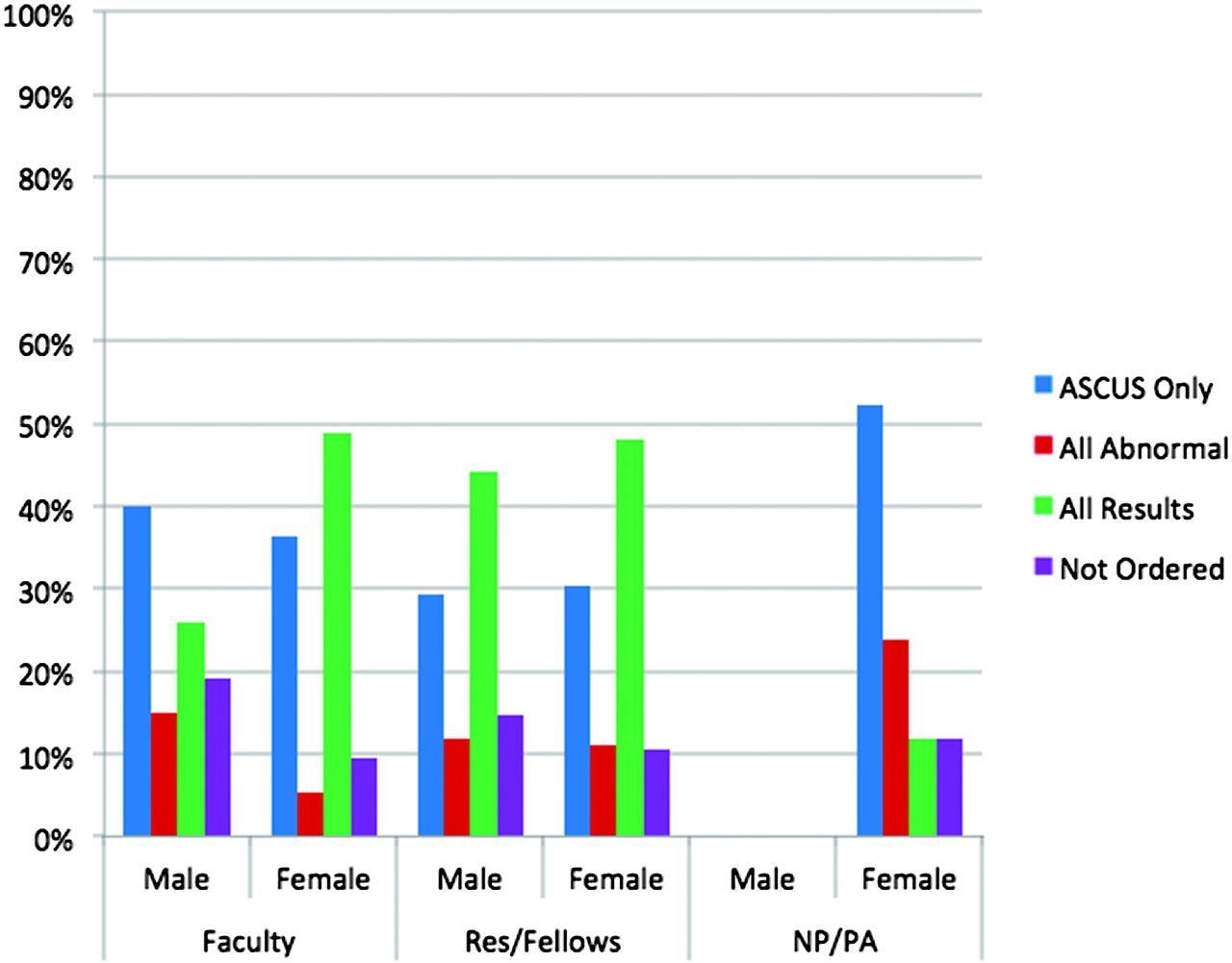
Female providers were significantly more likely (P < .001) than male providers to order HPV testing for all results across all clinics and provider types (Figure 3). Male providers were more likely to order HPV testing for ASCUS only. Male and female residents/fellows did not have significantly different rates of ordering HPV testing for all results. Since all NP/PA providers were female, we did not carry the NP/PA category forward in further analyses.

Human papillomavirus testing order by provider status and provider sex (P < .001). ASCUS, atypical squamous cells of uncertain significance.
Ordering HPV Testing Between Combined Faculty-Resident Clinic Sites
In comparing the 2 resident training sites (clinics A and B), clinic A providers were twice as likely as clinic B providers to order HPV testing for all results after adjusting for age at the time of Papanicolaou and provider status (adjusted odds ratio [OR], 2.3; 95% confidence interval [CI], 1.4–3.7) (Figure 4). Female providers were twice as likely as male providers to order HPV testing for all results (adjusted OR, 2.3; 95% CI, 1.4–3.7). Despite a significantly younger patient population at clinic B, with age at Papanicolaou being approximately 6 years younger, age at Papanicolaou and provider status were not significantly different (P > .5). There was no significant interaction between provider sex and clinic site (P > .5).

Human papillomavirus testing order by provider sex at clinics A and B (resident and faculty clinics) (P < .001). ASCUS, atypical squamous cells of uncertain significance.
Ordering HPV Testing Between Faculty-Only Clinic Sites
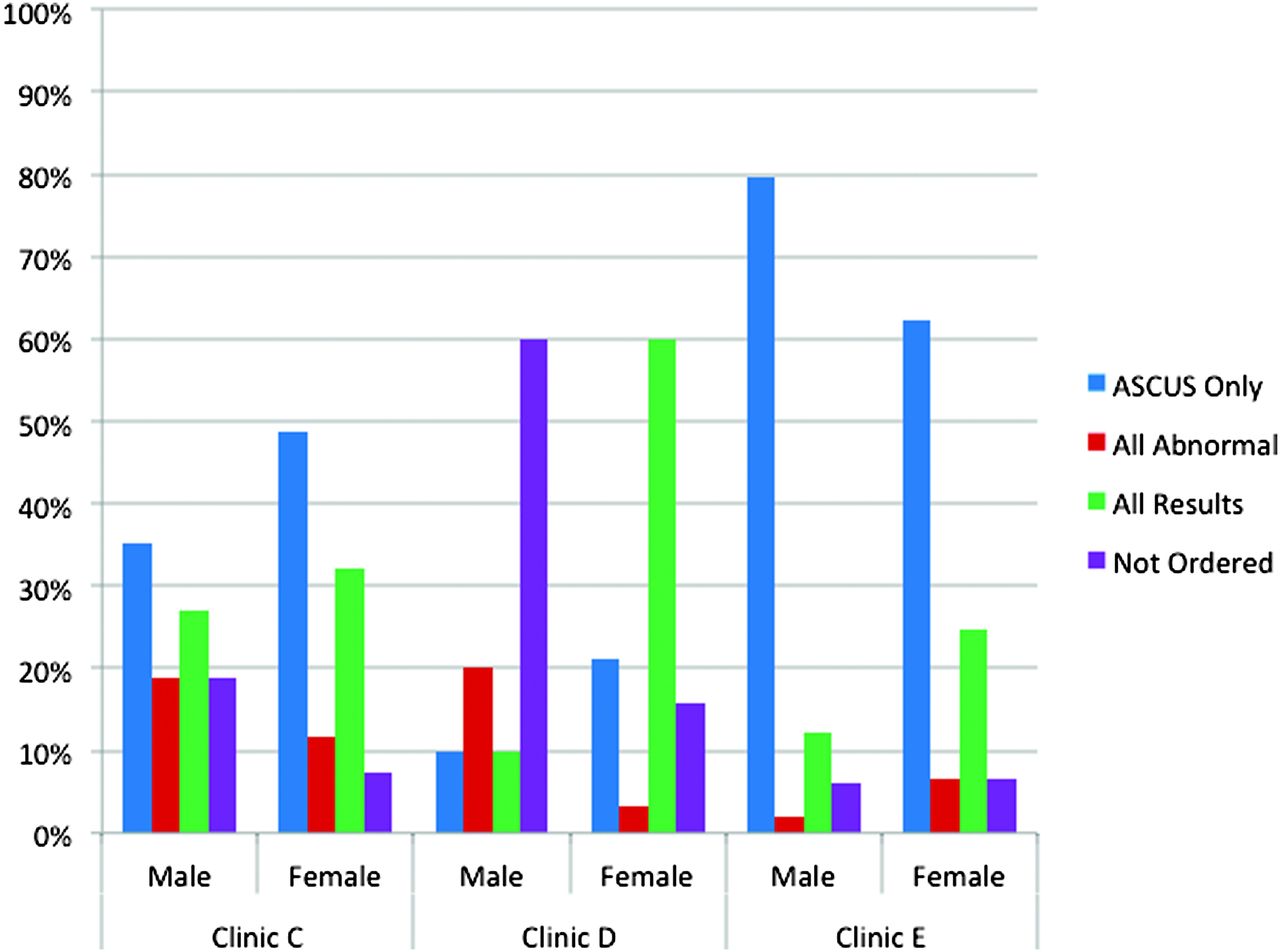
When examining faculty-only sites (clinics C, D, and E), female faculty providers were twice as likely to order HPV testing for all results than male faculty (adjusted OR, 2.1; 95% CI, 1.3–3.3) (Figure 5). Regarding specific clinic differences, clinic C providers were twice as likely as clinic D providers to order HPV testing for all results (adjusted OR, 1.9; 95% CI, 1.1–3.3), whereas clinic D was 4 times as likely to do so compared with clinic E faculty (adjusted OR, 3.8; 95% CI, 2.1–7.0). In clinic E, the majority of orders for HPV testing by both male and female faculty was for ASCUS only, as seen in Figure 5. There were no significant interactions (P > .5) between provider sex, clinic site, or patient age at time of cytology.

Human papillomavirus testing order by provider sex at clinics C, D, and E (faculty-only clinics) (P < .001). ASCUS, atypical squamous cells of uncertain significance.
HPV Test Ordering Over Time
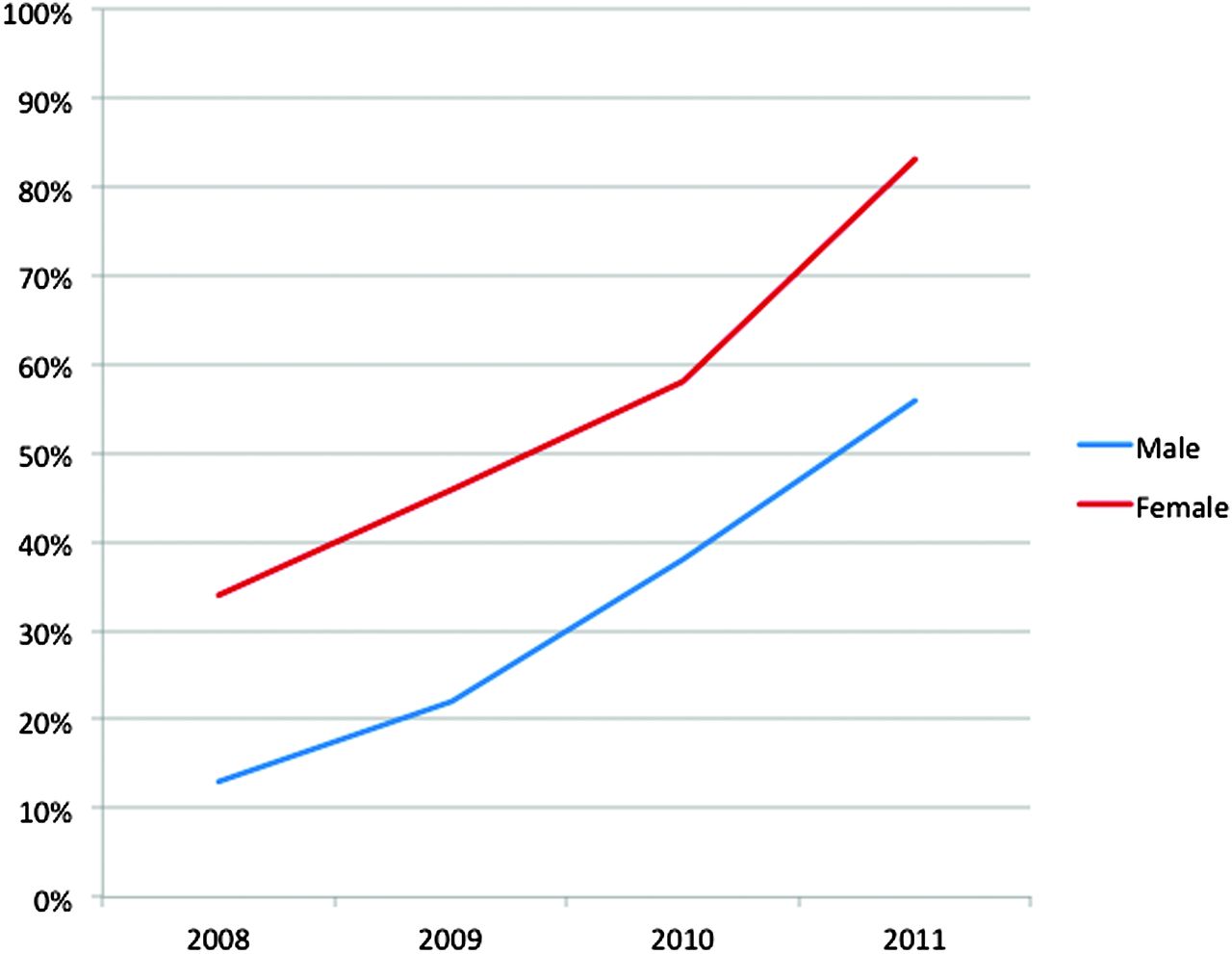
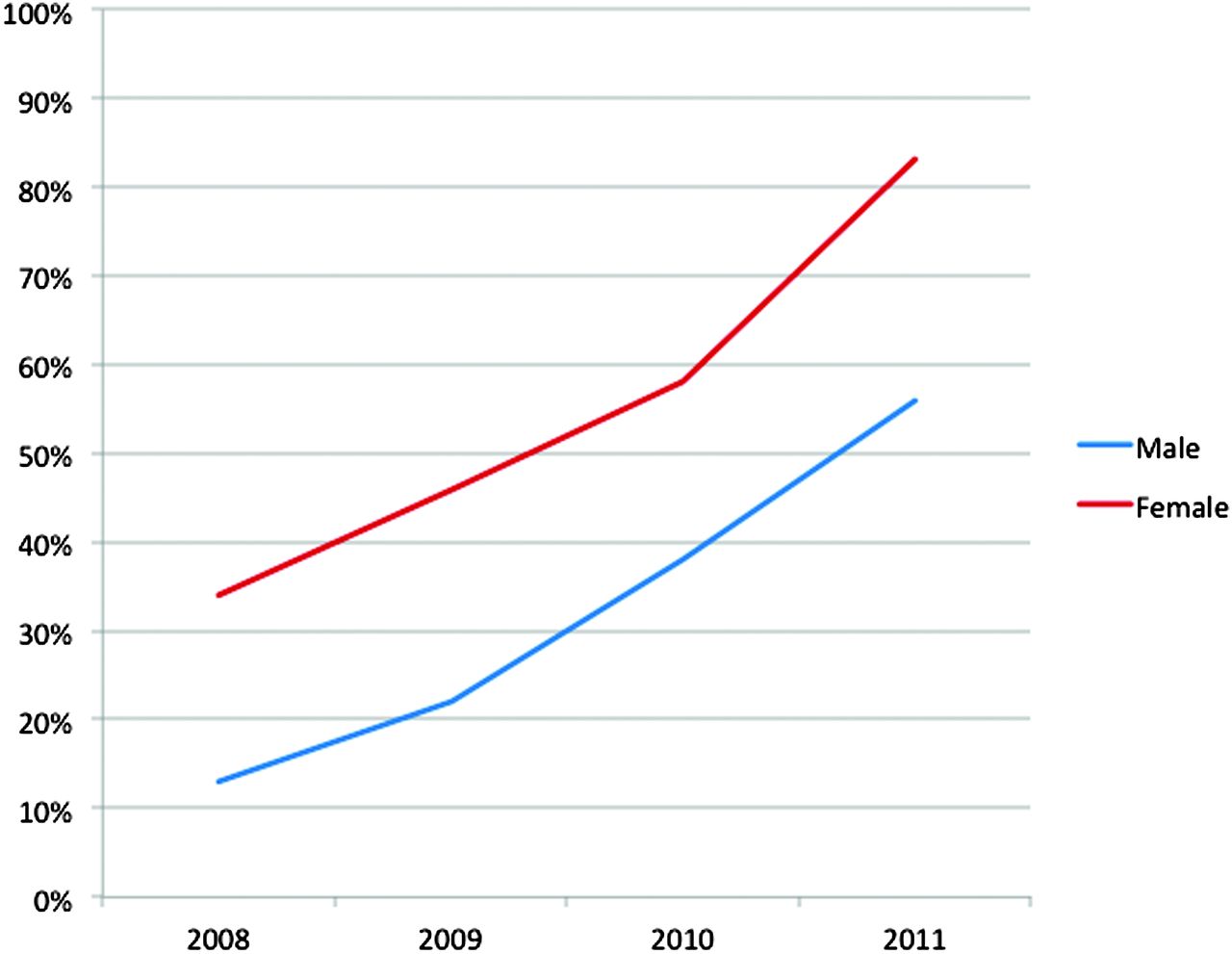
The number of cytology requests ordered by faculty each year is summarized in Table 1, stratified by clinic site and faculty sex. Female faculty providers ordered HPV testing significantly more often (P = .001) than male faculty providers from 2008 to 2011, as shown in Figure 6. In the regression model, the data for faculty sex and year of cytology request are summarized in Table 2.
Percent of Papanicolaou smear with orders for human papillomavirus testing for all results over time by faculty sex.
Discussion
To our knowledge, this is one of the first studies to examine differences in HPV test ordering with regard to provider sex and provider status by clinic. We note several unique observations never previously reported. First, female clinicians were more likely to order HPV testing for normal cytology except at one site. Second, residents/fellows were more likely than faculty to order HPV testing for normal cytology, possibly because they receive more current training on gynecology and the most recent cervical cancer screening guidelines. Third, NP/PAs were more likely than faculty to order HPV testing only for triage of ASCUS cytology. Finally, providers at one of the sites (clinic E) were more likely to order HPV testing for ASCUS triage than for normal cytology. After presenting the data to each clinical site, we learned that clinic E trained all their clinical staff to complete the cytology request forms for the clinicians. The training included marking HPV testing for “ASCUS only” on the form for women aged 30 to 65 years unless otherwise instructed by the clinician. Since the presentation of this data, clinic E has retrained its staff in the completion of cytology request forms. None of the other clinics had any systematic training of their support staff related to completing the cytology order form.
The strength of this study is the use of cytology request forms that include selection for HPV co-testing. This has advantages over secondary billing data2 and self-reports,7 with findings more consistent with pathology reports.9 Our findings demonstrate a higher percentage of ordering HPV testing (39%) at the time of cervical cytology compared with other studies.2,8,9 In addition, we found that one of the clinical sites' staff training on completion of the cytology request form resulted in a disparate ordering of HPV testing compared with the other clinics. Price2 similarly found that only 26% of HPV DNA tests were ordered appropriately in women older than age 30 and only 31% of HPV DNA tests were ordered appropriately for ASCUS triage. Overall, our results do demonstrate an increase in ordering HPV testing for normal cytology over time by both male and female faculty, as noted by others.2,8,9
The results of this study are important because they indicate that clinic differences based on training can lead to variations in ordering practices for HPV testing and possibly inappropriate ordering of HPV testing. As HPV testing becomes more frequent, there should be an emphasis on improving the current options to order HPV tests. As more departments and practices develop and shift to more advanced electronic medical records, HPV co-testing at the time of cervical cytology can be more precisely ordered. The current recommendations for HPV co-testing are to order it for normal results if extending the interval of cytology to 5 years or to triage ASCUS cytology. Our current options for HPV ordering at time of cervical cytology results in more women than necessary getting HPV testing. One suggestion for primary care clinics that perform cervical cancer screening would be to have 2 different options: (1) cytology every 3 years or (2) cytology with HPV testing every 5 years (where ordering HPV testing is checked by default). For women ages 21 to 29, the ordering system could be set to a default order for HPV testing for ASCUS only.
There were several limitations to this study. During the review of all the cytology request forms, we were unable to determine intervals of screening for each patient. If some women opted for frequent cytology, such as annually or every 3 years, providers may not have ordered the HPV test. However, we did not observe any patients with annual or biannual cytology. Some women may have opted not to have HPV testing because of cost or lack of insurance coverage. We have no data to address these issues. We also could not determine who actually completed the forms (ie, the physician, medical assistant, or nurse). Because of this, the total denominator of Papanicolaou smears performed by each physician could not be calculated. The data presented also do not reflect whether any changes were made to the orders for HPV testing after the cytology results were presented to the ordering clinician. Clinicians may have requested HPV testing after the cytology was reported. However, we did not see any evidence of these requests since any changes are supposed to be recorded on the original request form by the cytology service. This study included our best definition of low risk (as all-inclusive as we could define it). Our interest was in the uptake of ordering HPV testing for normal cytology. While the order option of “all results” is not precise, it does include normal cytology. We assume all clinicians understood the order was for HPV testing to be done when there was normal cytology. Finally, the number of cytology orders examined for some clinicians was small and may not reflect their actual practice patterns.
Conclusion
Overall, our study shows that there are significant differences in practices of ordering HPV testing for normal cytology results based on provider sex, provider status, and provider clinic. The results also demonstrate that the frequency of HPV testing is increasing over time. Additional interventions should focus on best practices to facilitate appropriate HPV testing to improve cervical cancer screening and long-term outcomes for women.
Acknowledgments
The authors thank Jill Bowdler and David Tumbarello for their technical and editorial assistance.
Notes
This article was externally peer reviewed.
Funding: This study was supported by a grant from the National Institutes of Health/National Cancer Institute (CA080846–06A1 to MTR), and the Dr. Max and Buena Lichter Research Professorship in Family Medicine at the University of Michigan (MTR).
Prior presentation: This work was presented as an oral presentation at the 34th Annual Michigan Family Medicine Research Day Conference, Howell, MI, May 2011.
Conflict of interest: none declared.
- Received for publication September 18, 2012.
- Revision received June 17, 2013.
- Accepted for publication June 25, 2013.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}