
Abstract
Introduction: The declining number of family physicians providing pregnancy care is of concern because they are an important source of pregnancy care in underserved communities. Innovative approaches might reinforce family physician participation in pregnancy care for the underserved. Since group prenatal visits have been shown to improve patient education, support, and satisfaction, we implemented and evaluated a group prenatal visit program for Japanese women in Michigan, an underserved population because of their limited proficiency with English.
Methods: We conducted a convergent quantitative and qualitative mixed methods evaluation involving repeated survey administration (program evaluations, 4-item Patient Health Questionnaire, pregnancy distress questionnaire) to participants during 5 group visits and in-depth postpartum interviews in the University of Michigan Japanese Family Health Program setting. We conducted independent quantitative and qualitative analytics and then thematically integrated these data.
Results: Cultural adaptations to the Centering Pregnancy format involved changes in total visits, educational content, and participation format. Based on 5 groups attending 5 sessions each, 42 women evaluated the program through 158 surveys after the sessions. Participants evaluated multiple parameters positively: being with other pregnant women (98%), improving their understanding about prenatal care (96%), preparation for labor and delivery (96%), organization of visits (94%), and preparation for newborn care (85%). In final evaluations, 96% to 100% of participants rated 7 educational topics as “covered” or “covered well.” Qualitative interviews with 20 women revealed positive views of social support from prenatal group visits and group facilitation but mixed enthusiasm for clinical assessments in the prenatal group visit setting and partner and children attendance at the sessions.
Conclusions: This research demonstrates the feasibility and cultural acceptability of prenatal group visits for Japanese women. Prenatal group visits provided education and social support for Japanese women during the perinatal and postpartum periods that were not otherwise accessible in Japanese. This study confirms the feasibility of family physicians providing prenatal group visits and extends the literature of the applicability of prenatal group visits for patients with limited English skills.
- English as a Second Language (ESL)
- Evaluation Research
- Japanese
- Mixed Methods Research
- Prenatal Care
- Underserved Populations
According to the 2010 US Census, there will be no majority group by 2050,1 a change due to the growth in nonwhite minorities. Thus, family physicians will increasingly need to be prepared to provide linguistically and culturally appropriate care. Patients from the growing minority groups face a host of cultural and linguistic differences from the white majority population during their encounters with the health system.2,3 Even though the National Standards of Culturally and Linguistically Appropriate Services recommend all hospitals and providers to make arrangements for interpretation4 when necessary to communicate, receiving care in one's own language is preferable.
Family physicians train to provide the full breadth of care for common problems across the life span and are particularly recognized as apropos in isolated rural communities and underserved populations. As with family physicians providing care for a geographically isolated population, a bilingual family physician can also be particularly effective for linguistically and culturally isolated groups regardless of rural or urban setting.
Family physicians have long been considered an important source of maternity care, particularly in rural and underserved settings.5⇓–7 The number of family physicians providing maternity care is unfortunately declining—only 9.7% of practicing family physicians in 2011 provided this type of care,8 compared with 23.3% in 2010 and 43% in 1986.6 New and rewarding approaches to pregnancy care might reinforce the motivation of family physicians to participate in birth care.
The group prenatal visit program of the Centering Health Institute (CHI) was originally developed and piloted by a nurse midwife in 1993 to 1994.9 The results of this model have been impressive. Women attending group prenatal care are less likely to have suboptimal prenatal care and have better prenatal knowledge, feel more prepared for labor and delivery, have greater satisfaction with care, and have a higher rate of initiating breastfeeding.10 This model has been adapted successfully for use with African American teenagers, women in the military, and Latinas.11⇓⇓–14 Barr et al15 published the only known empirical article on group prenatal care by family physicians; they reported that women who attended group visits experienced fewer cesarean deliveries and less preterm labor compared with women receiving traditional prenatal care.
Given the sparse published data on group prenatal visit programs by family physicians and their potential for unique application among populations who speak limited English, the goal of this study was to examine the feasibility of conducting group prenatal visits in a family medicine setting with Japanese women who have limited English skills and different cultural backgrounds. To achieve this, we describe here our experience developing, implementing, and evaluating this program. Key measures include acceptability of the content of the program; the effect of the program on distress, anxiety, and depression scores over time; and the cultural acceptability of the program and family physicians as providers of birth care.
Materials and Methods
Design
We use a mixed-methods case study approach to describe our translation and cultural adaptation of the Centering Pregnancy program into Japanese. The assessment used a convergent quantitative and qualitative mixed-methods design to assess quantitatively the patients' acceptance of the program as well as the experiential aspects. Data collection required repeated surveys with group participants and in-depth interviews with a sample of survey participants. The University of Michigan Institutional Review Board approved this study.
Setting
The Department of Family Medicine's Japanese Family Health Program (JFHP) at the University of Michigan offers culturally and linguistically sensitive care to the population of Japanese patients residing in Southeastern Michigan.16,17 Staff and family physicians who are fluent in Japanese and knowledgeable about cultural differences provide full-spectrum family medicine services to Japanese-speaking people in the area.
Group Visits
The prenatal group visit model as developed by the CHI consists of 10 group visits that replace all other prenatal visits. A group consists of 8 to 12 women who have expected delivery dates within 1 month of each other. They meet once a month except for the last 3 sessions, which are held every 2 weeks.9 Each group session lasts 2 hours. The first 30 minutes are used for individual prenatal care assessments by a provider in a corner of the room, while other members talk over tea and snacks. The remaining 90 minutes are dedicated to an educational session led by the facilitators.9
With permission from CHI, we created a Japanese group visit program based on their model8 with modifications. Because of the lower numbers of pregnant Japanese women, we allowed women with expected delivery dates within 2 to 3 months to be in the same group. We reduced the number of sessions to 5 so women also could have some private visits. Sessions are held monthly, except for the last 3 sessions, which are held once every 2 weeks. All 5 sessions are facilitated in Japanese by both a family physician and a registered nurse. The educational topics focus on (1) personal goals, nutrition, and exercise; (2) pregnancy-related discomfort and relaxation techniques; (3) danger signs and the flow of labor and delivery; (4) decision making during labor and delivery, birth planning, and car seat instructions; and (5) breastfeeding, baby care, and postpartum care.
Data Collection Instruments
Three bilingual physicians independently translated into Japanese the 4-item Patient Health Questionnaire (PHQ-4), the Pregnancy Distress Questionnaire (PDQ), and the CHI group visit evaluations. They then discussed the differences in translation to develop a reconciled version. The Japanese translation was then translated back into English by an independent bilingual person to confirm the accuracy of the translation. The PHQ-4 is a 4-item validated anxiety (2 items) and depression (2 items) screening and surveillance tool.18 The PDQ is a 12-item instrument assessing distress and worries related to pregnancy on a validated 5-point Likert scale.19 The CHI session evaluation contains 5 Likert scale questions regarding beliefs about the visit and 4 open-ended questions regarding likes, dislikes, desired changes, and general impressions. The CHI program evaluation examines content coverage, support received from the groups, and privacy issues. To our knowledge, the PHQ-4, PDQ, and CHI questions have not been revalidated in Japanese, but doing so was beyond the scope of this study.
For the postpartum interviews, the research team developed a semistructured interview guide using a grand tour approach20 to understand the women's experience with the prenatal group process. The interview content focused on perceptions of the program, acceptability of prenatal group visits, and how group visits affect social support and prenatal education.
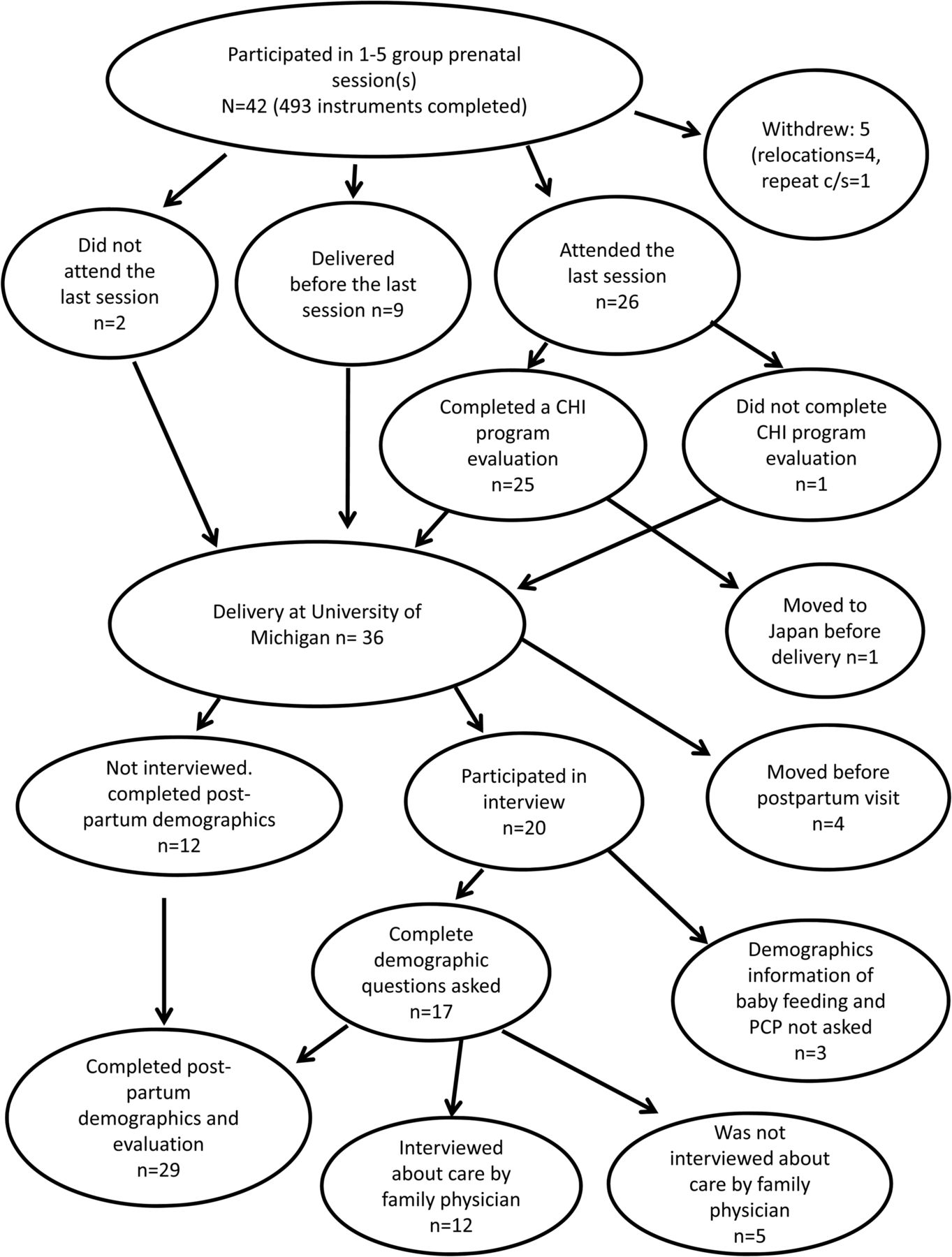
Demographic data of women who participated in a postpartum interview were collected at that time (Figure 1). The demographics questionnaire was mailed 2 months after delivery to group visit attendees who did not participate in a postpartum interview. Patients who moved to Japan or other geographical areas could not be reached to take the demographics instrument.

Flow Diagram Illustrating Japanese Women's Level of Participation in the Study. CHI, Centering Health Institute; PCP, primary care physician.
Recruitment
Using a consecutive sampling strategy, all women attending the JFHP for prenatal care were eligible to participate. Women who attended at least 4 sessions were eligible to participate in the postpartum interview. All subjects provided written informed consent.
Data Collection
Data collection spanned from May 2010 to January 2012. The CHI session evaluation, PHQ-4, and PDQ were given to participants after each session, while the CHI program evaluation was administered during the last session only. The first 20 women who met study criteria for interviews and consented to participate were enrolled. The research assistant scheduled interviews 6 to 10 weeks after delivery. Interviews were conducted in Japanese either in person in the clinic (n = 10) or by telephone (n = 10), according to each woman's preference. Additional questions were added during the study to explore new issues raised by the participant's responses, for example, baby's primary care physician, benefit of a family physician to care for mother and baby, and breastfeeding. The interviews were tape recorded and transcribed. The analysis was conducted iteratively in Japanese.
Analysis
We used SPSS Statistics version 20 (IBM, Chicago, IL) to calculate descriptive statistics on all quantitative data. Qualitative data were analyzed using a team approach lead by a primary analyst (SM). Transcripts were read multiple times with initial open coding. We iteratively developed and used a coding scheme for text searches. For the mixed-methods analysis, we integrated through narrative the scores from quantitative questions with related content from the qualitative data.
Results
A total of 42 women participated during the 4 groups, although not all women attended all sessions. Of 509 instruments distributed to these 42 women during the study, 493 questionnaires were collected (response rate 96.8%). Of the 42 women, 4 returned to Japan during pregnancy and 1 patient withdrew from the group visit program after finding out that she required a repeat cesarean delivery (Figure 1). Of the 37 women who remained in the program, 26 women attended the last session; 25 completed the CHI program evaluation, and 1 returned to Japan. Because each group included women with estimated due dates within 3 months, 9 women delivered before the last session. As a consequence, the attendance at the last session was the lowest. Of the 36 women who delivered at our affiliated hospital, 4 moved out of the area before the demographic questionnaire was mailed to them. Since demographic data were not collected until the postpartum survey or interview 2 months after delivery according to our protocol approved by the institutional review board, demographic data could be collected from only 32 women.
All women who provided demographic information had term deliveries and were breastfeeding at 8 weeks postpartum (Table 1). Among 29 women who answered the question, 27 chose a JFHP physician for the baby's health care.
Summative evaluations of the group prenatal visit session evaluation reveal that women unanimously enjoyed being in a group with other pregnant women (Table 2). A majority of women felt well prepared for labor and delivery, learned a lot about prenatal care, and liked the organization of prenatal care as group visits. Although only 85% of the women reported being well prepared for newborn care in surveys collected over all 5 visits, teaching about newborn care was not provided during the first 3 sessions. When considering only responses from the fourth and fifth session, when the topic of newborn care actually was covered, 96% of the women reported feeling well prepared. The positive responses to other questions did not change over time. The summative evaluation after the last session revealed that women felt the 7 educational topics emphasized during the prenatal group visits were “covered” or “covered well” (Table 2).
Data on social support came from the final evaluations and interviews. Of 25 women who completed a final evaluation, 21 (84%) answered that they were able to get to know other women. Interview comments about the value of prenatal group visits for social support are provided in Table 3. Comments from the CHI program evaluation were similar. Other representative comments included “Somehow we felt connected as a group as pregnant women whose due dates are close together” and “I did not have many friends and it was great that I could get to know other women and exchange information.”
To evaluate continued social support after each group ended, the program evaluation also asked whether women wanted to get together after delivery for a reunion. Sixteen women (62%) stated they wanted to get together again, and 13 (52%) said they planned to stay in contact with other participants. Similar statements were given during interviews: 8 of 20 women interviewed mentioned they had support from other participants after delivery. Representative comments included, “We could exchange information about where to buy baby goods”; “I really enjoyed the reunion after delivery”; and “We exchanged E-mails at the reunion and I am still in frequent contact with one of the group members.”
Complementary qualitative comments about the value of group prenatal program are depicted in Table 3. Main themes were “it was easy to ask questions and talk” and “it was a calm and relaxing atmosphere.” Some women felt that time restrictions limited questions.
Overall, depression, anxiety, and stress scores were low; a lower score on the PHQ-4 means less depression or anxiety, and a lower score on the PDQ means less distress. The mean scores on the PHQ-4 and PDQ were 1.4 (standard deviation, 1.4; range 0–12) and 13 (standard deviation, 6.6; range 0–48), respectively, and the scores did not change significantly over time. For all items, there were no significant or clinically meaningful differences between multiparous and primiparous women.
We also assessed these women's views about the cultural acceptability of the prenatal group program relative to personal boundaries and involvement of other family members in prenatal group sessions. Receiving a prenatal assessment with only a free-standing curtain divider to create a semiprivate space between other patients and the patient-physician dyad was a new experience for the women. Of the 25 women responding to questions about interpersonal boundaries in the CHI program evaluation, 16 (64%) stated that they were comfortable with an examination in the group setting, and 17 women (68%) were satisfied with the examination and assessment. If given a choice, 15 women (60%) preferred an individual assessment in the group setting instead of a private room. When asked during interviews, 11 of 20 women said that they had no problem having the examination in the group setting, although 10 stated they preferred a private examination room rather than the group setting (Table 4). Representative comments included “I was fine as I had delivered before, but if this was the first pregnancy, I might have been more hesitant”; “I was worried if there was no heart tone or something bad happens where everybody is in the room”; and “It was hard to ask questions about vaginal discharge because people can hear us.”
Regarding the decision to let husbands join the group, results from the CHI program evaluation (n = 25) showed that 20 women (80%) felt okay with having men in the group discussion, and 15 women (60%) felt okay allowing men to be in the same room during patient examinations conducted behind the curtain. In the individual interviews, a majority of women welcomed a spouse's presence and stated that they thought it was a good idea for the partner to learn about pregnancy and baby care (Table 4). Some mentioned positive feelings about their spouse's presence in the group. However, 5 of 20 women interviewed stated that there was no need for men to join the group, and 7 of 20 women expressed that some subjects are difficult to discuss in the presence of men. Comments about husband participation ranged from not favorable (“I enjoyed the women only group better”) to reluctant but accepting (“At first, there were men I didn't know and it made me nervous, but it didn't bother me after I got used to the group”) to enthusiastic (“It didn't bother me at all, it is good for husbands to learn about labor and delivery”).
Contrary to the Centering Pregnancy approach, we allowed children in our group because most women are homemakers and do not routinely use child care services. Despite preparations to minimize disruptions, children sometimes created distractions. Of the 20 interviewees, 8 women (3 primiparous and 5 multiparous) felt there was no problem with children's attendance (eg, “The children were behaving and I was not bothered at all”); 6 women (1 primiparous and 5 multiparous) reported that they were distracted by the children.
After birth, a majority of women chose to receive care for their infant from the family physicians in our program. Regarding the choice to have the same physician for both mother and baby, 11 of 12 women discussed the sense of security and satisfaction of continuity (Table 5). Still, 2 of 12 expressed concern about whether family physicians have the same level of competency of obstetricians and gynecologists.
Discussion
This research demonstrates the feasibility of implementing a group prenatal visit program for Japanese women in a family medicine setting. We culturally modified the Centering Pregnancy program based on our previous clinical experience16,17 and research.21 To our knowledge, this is the first-ever application of a group prenatal visit program in Japanese. We firmly believe that sociocultural adaptations to the Centering Pregnancy model were critical. Especially important changes included fewer sessions and changes in the topics covered, for example, dropping the topic of domestic violence and adding newborn care and teaching about differences in pregnancy care between Japan and the United States.21⇓–23 We did not modify the approach to a semiprivate clinical examination in the room, but opinions about this varied: about half expressed concerns about compromised privacy, a primary source of discontent related to them not wanting other participants to overhear conversations.
This study adds to the literature on the applicability of the Centering Pregnancy model of prenatal group visits for patients with limited English skills. For example, Robertson and colleagues14 demonstrated the benefits of group prenatal visits in previous work with Latinas. Given the importance of culturally and linguistically sensitive care,24 government interest in reducing health disparities,25 and previous work suggesting that minority populations with limited English proficiency and different cultural beliefs benefit from programs tailored to their needs for optimal pregnancy care,26⇓–28 expanding group prenatal visits is needed. Limitations in developing such programs include the availability of bilingual providers and staff and sufficient volume of patients: a minimum of 6 to 8 patients per group is needed to be financially neutral. For the care of populations with limited English ability and diverse cultural backgrounds, family physicians are particularly apropos because of the breadth of care they provide.
This research also illuminates potential variations in the Centering Pregnancy model that stipulate partner attendance is decided by group member discussion and children are not allowed. In our study, some women supported the participation of men, while others felt that it is easier to discuss topics without men present. We decided to allow attendance by husbands without discussion in each group because all women were married, prenatal classes in Japan typically involve the partner's attendance, and participation of partners was requested by many Japanese women. While the number of negative comments was limited, the presence of children was distracting to some mothers regardless of whether they had their own children. In our setting this was important because allowing children to attend facilitated the participation of women with previous birth experiences who were important role models for nulliparous women and knowledgeable about differences between Japan and the United States.
There are a number of potential limitations of this research. First, in group prenatal research, selection bias can arise from studying only those who choose to participate, although nearly all primiparous women and the majority of multiparous women from our clinic chose to participate. Second, the study has a relatively small sample size because of a small overall pool of eligible women, although the JFHP has a very high penetration in the Japanese market in Michigan, and the sample accounts for nearly the entire population of eligible women from this community. Third, among the sample, participation was inconsistent because of social factors that were not likely to bias the results, such as transportation, relocation to Japan, and wide variations in estimated due dates. Fourth, while the PHQ-4 and the PDQ have been validated in English, they have not been validated in Japanese. Many studies using instruments validated in English do not do additional validation work when the instruments are translated. Moreover, the investigators have high levels of bilingualism and biculturalism and believe the translations are accurate and that the content has face validity.
The number of family physicians providing birth care is declining.8,29,30 Reasons for the decline in recent years are not well studied, but previous research suggests fear of malpractice suits,31 cost of protection against such suits,7 and disruption of personal and professional life.32 While denied privileges, inadequate specialty backup, concerns about insufficient training, and other factors have been cited, according to data from the American Academy of Family Physicians, most family physicians who are not delivering babies cite “not desiring” to do so as their reason.33
Group prenatal visits could help rejuvenate and/or sustain family physician interest in birth care. There are no known data in the literature on provider satisfaction with group prenatal visits,34 and, even if available, they likely would be biased positively since providers choose whether to offer it. However, we find that our own physicians and staff members enjoy the program. This finding is consistent with a previous report of provider satisfaction with group visits for diabetic patients and group prenatal visits.35 In addition, group prenatal visits may provide a marketing edge for attracting pregnant women into family medicine offices and provide novel educational opportunities for residents. We hope our experience will inspire other family physicians to leverage the advantages and fun of group prenatal visits regardless of whether their patient population is underserved in some way.
Conclusion
These results demonstrate the feasibility of an innovative, supportive group prenatal visit model for providing prenatal care to Japanese women. Moreover, it extends the research on using the model for women who speak limited English and their positive responses to this method of care. The results show mixed enthusiasm for the inclusion of children and partners in group-based prenatal care. Finally, the study extends the literature on the positive experiences of family physicians providing prenatal group visits.
Acknowledgments
The authors thank Haruko Osaki-Wurtz for clinical support, Michelle Thurston and Beth Ragle for research support assistance, and Ananda Sen, PhD, who provided consultation on the statistical analyses.
Notes
This article was externally peer reviewed.
Funding: This program and research was made possible by the generous support of a faculty grant from the University of Michigan Center for Japanese Studies; the Family Medicine Education Scholars Program, Department of Family Medicine, University of Michigan; and the Jitsukokai Foundation.
Conflict of interest: none declared.
- Received for publication January 6, 2013.
- Revision received May 16, 2013.
- Accepted for publication May 23, 2013.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- What are the mechanisms of effect of group antenatal care? A systematic realist review and synthesis of the literature
- Japanese Women's Concerns and Satisfaction With Pregnancy Care in the United States
- Fundamentals of case study research in family medicine and community health
- Family Physicians Improve Patient Health Care Quality and Outcomes