
Abstract
Background: The Colorado Asthma Toolkit Program (CATP) has been shown to improve processes of care with less evidence demonstrating improved outcomes.
Objective: To model the association between pre-and-post-CATP status and asthma-related process and outcome measures among patients ages 5 to 64 years receiving care in safety-net primary care practices.
Methods: This is an implementation study involving secondary prepost analysis of existing structured clinical, administrative, and claims data. Nine primary care practices in a federally qualified health center network implemented the CATP. Processes of care and health and utilization outcomes were evaluated prepost implementation in a cohort of patients with asthma using generalized linear mixed models.
Results: The study cohort included 2678 patients age 5 to 64 years with at least one visit to one of the 9 participating practices during the study period (March 12, 2010 to December 1, 2012). A comparison of 12 months pre- and post-CATP implementation showed improvement in some process measures of asthma care associated with the intervention, including the rate of asthma-severity measurement, although no change in 2 Health care Effectiveness Data and Information Set measures: asthma medication ratio and medication management for people with asthma. We also found no change in asthma outcomes measured across multiple domains: exacerbations, utilization, symptom scores, and pulmonary physiology measures.
Conclusions: Implementation of the CATP in a primary care setting led to some improved processes of asthma care, but no changes in measured outcomes. Recommendations for future work include supplemental follow-up training including case review.
Asthma is one of the most common chronic illnesses in the United States. In 2015, the overall prevalence of active asthma was 8.4% among children (6.2 million)1 and 7.6% among adults (18.4 million),2 and asthma is the lead diagnosis for 2.0 million Emergency Department (ED) visits3 and 340,000 hospitalizations3 annually. When managed appropriately in primary care settings, asthma is a controllable disease,4 such that most asthma exacerbations—episodes of increased airway obstruction—are preventable.5 As asthma exacerbations are the reason for asthma-related ED visits, hospitalizations, missed school/work days, and deaths, evidence on effective disease management strategies is a priority for policy makers,6,7 payers,8 and researchers,9,10 with most interventions targeting the primary care setting.4,11
National asthma guidelines12 and subsequent reviews13⇓–15 provide consistent guidance on what constitutes high-quality asthma care; nevertheless, clinicians' guideline concordance is inconsistent in primary-care settings.16⇓–18 The need for guidelines-focused training in primary care is well established,19⇓–21 but training programs have met with mixed success. Interventions designed to enhance diagnosis and management of respiratory diseases in primary-care settings have had variable success and have not been implemented broadly.22,23 The Colorado Asthma Toolkit Program (CATP) was introduced as a provider-level intervention to improve implementation of guidelines for high-quality asthma care through addressing known barriers and using known facilitators of implementation.24 Barriers to guideline implementation include lack of knowledge of guideline recommendations, doubt about the evidence base, and lack of time and resources.25,26 Facilitators of guideline implementation include improved teamwork, comprehensive training, and improvements in electronic record systems.26⇓–28
To improve guideline-concordance of asthma care in primary care, investigators from National Jewish Health (NJH) partnered with local stakeholders to develop both the content and implementation strategy for an intervention to address the known barriers to and facilitators of asthma treatment guideline concordance. The implementation strategy and content of the intervention—the CATP—was first developed in 2007 and addresses all 4 categories of provider-level asthma intervention.29 To date, 500 providers at 170 Colorado primary care practices serving safety-net patients have been trained using the CATP.30 As part of this program, NJH partnered with the Metro Community Provider Network (MCPN)31 to implement the CATP in 9 practices in 2011.32 MCPN is a network of health centers serving safety-net populations throughout metropolitan Denver.31 The MCPN CATP implementation was adapted from an earlier, stakeholder-designed version of the CATP that successfully changed practice behavior in 57 primary care offices in rural eastern Colorado.24 The CATP has been shown to improve guideline concordance of care processes related to spirometry, asthma action plans and inhaled corticosteroids; the 2 prior studies of the CATP did not assess patient oriented outcomes.24,32
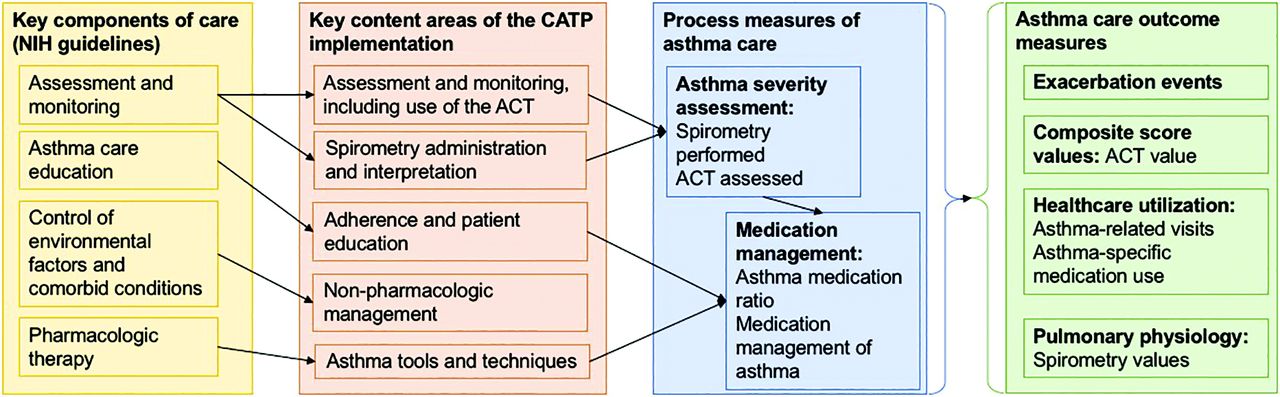
Assessment of the impact of the CATP on processes and outcomes has been limited by the minimal resources typically present in safety-net practices for tracking asthma outcomes longitudinally.32,34 However, MCPN participates in the Scalable Architecture for Federated Translational Inquiries Network (SAFTINet),34,35 an Agency for Health Care Quality and Research–funded practice-based distributed research network supported by a sophisticated technical infrastructure that standardizes clinical and claims data to a common data model and links electronic health record (EHR) and claims data at the patient level to facilitate patient -outcomes research.36,37 The SAFTINet partner databases include both the clinical EHR data and Medicaid claims data necessary for operationalizing standard asthma outcome measures.38 The objective was to perform secondary data analysis of asthma process and outcome measures associated with implementation of the CATP at MCPN practices, using existing data from SAFTINet. We performed a prepost single-group study of the CATP implementation, using generalized linear mixed models (GLMMs) to evaluate prepost changes in processes and outcomes of care at the patient level (Figure 1). Specifically, these measures include use of spirometry, asthma severity assessment, and asthma action plan use among all asthmatics, and controller medication use, and medication ratios among persistent asthmatics.39 We hypothesized that patients in participating practices would have improved asthma control and fewer exacerbations after CATP implementation compared with preimplementation.

Colorado Asthma Toolkit Program (CATP) Conceptual Model. Key content areas were introduced in 3 education and feedback/audit sessions, which were then reinforced via 3 other approaches: 1) organizational change to optimize efficieny integrating CATP processes into practice workflow; 2) decision support tools for asthma management; and 3) online resources to help reinforce and sustain practice changes.
Methods
Study Design and Setting
We performed an implementation study involving secondary prepost analysis of existing structured clinical, administrative, and claims data. The data network from which study data were obtained is SAFTINet, a clinical and claims distritubed data network designed to securely share electronic health data to support quality improvement and research. The SAFTINet databases include existing administrative, clinical, Medicaid claims, patient-reported outcome data including the Asthma Control Test (ACT),40 and enrollment data collected during routine clinical care. Data are standardized to the Observational Medical Outcomes Partnership common data model (Version 4; Observational Health Data Sciences and Informatics).41 The data are limited data sets as defined by the Health Insurance Portability and Accountability act, deidentified with the exception of service dates, birth dates for those <90 years old, and zip codes.
We requested data from the MCPN SAFTINet database for patients who had experienced at least 1 encounter during the study period at least one of the 9 participating practices. Electronic health data from the SAFTINet databases was used to select patients for inclusion in the cohorts, to operationalize patient-level outcomes and covariates, and to associate patients with practices.
Cohort Selection
Inclusion criteria included age between 5 and 64 years by the start of the study period (March 12, 2010 to December 1, 2012); at least one visit to an MCPN practice during the study period; at least 1 month of Medicaid eligibility during the study period; and either an asthma diagnosis or an asthma-specific medication. As our primary outcome measure and other measures included criteria available only in claims (Colorado Medicaid) data, we excluded patients who had no months of Medicaid coverage during the study period. Given the chronic nature of asthma, for asthma diagnosis events, we included any asthma diagnostic code or string assigned for the patient during the study period or 5 years before study inception. As asthma-specific medications, we included any prescription or fulfillment of at least 1 medication from the Health care Effectiveness Data and Information Set (HEDIS) list, “Asthma Controller and Reliever Medications,” that occurred during the study period.42 We included the same cohort in both the pre- and postintervention study periods. For more details on the definitions used for asthma diagnosis events and asthma-specific medications, please see the Technical Appendix.
Intervention
Four provider-level asthma intervention categories29—decision support, organizational change, audit and feedback, and education—have been shown to be effective in improving the quality of primary asthma care processes.5,43 These were all incorporated into the CATP implementation as follows.
Education and feedback/audit: All clinical care team members were invited to 3 training sessions led by a nurse practice coach. A practice-coaching strategy was used to emphasize teamwork and to develop a practice-specific asthma protocol. Session 1 was 7 hours, with content in 6 modules: 1) assessment and monitoring, including use of the ACT, 2) spirometry administration and interpretation, 3) asthma tools and techniques, 4) adherence and patient education, 5) nonpharmacologic management, and 6) case studies. Sessions 2 and 3 were 3 hours long and reviewed module content, spirometry technique, collaborative self-management, and specific cases. For the ACT, clinical care teams administered the childhood version for children age 5 to 11 years (asking the parent to complete it on behalf of the child) and the adult version for ages 12 to 64 years.
Organizational change: At each session, the practice coach used interactive discussion to develop a practice-specific asthma protocol aimed at optimizing efficiency in integrating CATP processes into practice roles and workflow. Practice members were also asked to identify an “asthma champion” to help lead implementation of the practice-specific asthma protocol.
Written and computerized clinical decision support: Each provider received a provider manual containing all content from the training, a spirometry guide, and copies of the ACT and an asthma action plan. The CATP EHR asthma template includes severity assessment tools and decision support guiding initial asthma management and recommended actions for ongoing management based on asthma control.
Online resources: Providers were given access to online support to help reinforce and sustain practice changes, including an Asthma Toolkit Web site and Facebook page. These were made accessible to trained and new MCPN providers. The Web site contains training module videos and provider training manuals. The Facebook page permits providers and the NJH CATP team to interact about the CATP.
Study Periods
The intervention period for the CATP was March 12, 2011 to December 1, 2011. We selected a 1-year pre- and postintervention period (March 12, 2010 to March 11, 2011 and December 2, 2011 to December 1, 2012) for our analysis.
Process Measures Related to Guideline Concordance of Asthma Care
To evaluate the implementation, we selected and assessed several process measures directly related to the content in the CATP training program, as shown in the study's conceptual model (Figure 1).24 Each process measure was assessed at the patient level, resulting in separate, dichotomous variables indicating concordance (yes/no) for the pre- and post-CATP periods. The investigators selected process measures for inclusion based on their use in the initial evaluation of the MCPN CATP intervention, their consistency with the conceptual model (Figure 1), their relevance to the National Institutes of Health asthma guidelines, and their endorsement by the National Quality Forum (NQF).
The 2 NQF-endorsed HEDIS asthma-process measures were the Medication Management for People with Asthma (the percentage of individuals 5 to 64 years of age who were identified as having persistent asthma and were dispensed appropriate asthma controller medications that they remained on for at least 75% of the period) and the Asthma Medication Ratio (the percentage of individuals 5 to 64 years of age who were identified as having persistent asthma and had a ratio of controller medications to total asthma medications of 0.50 or greater during the measurement year).39 The denominator for these 2 measures is “persistent asthma,” defined via both HEDIS measure specifications as having at least 1 of the following during each of 2 successive years: an asthma-specific ED visit or inpatient visit, at least 4 outpatient asthma visits plus at least 2 asthma-specific medications, or at least 4 asthma-specific medications. We used only Medicaid claims data to calculate HEDIS measure values, as instructed in the HEDIS measure specifications39 (more details in Technical Appendix). We chose not to also include EHR data in calculating these measures to avoid including duplicate records of medications or visits from the 2 data sources (EHR and claims).
We included asthma control measurements—both spirometry and ACT—as process measures (how many were assessed in each period) and as outcome measures based on the value of each measure. We assessed spirometry performance based on procedure codes.
Outcome Measures
To evaluate the effectiveness of the CATP, we evaluated a variety of health and utilization outcomes. The study used 4 categories of outcomes recommended for observational studies by the Asthma Outcomes Workshop convened by the National Institute of Health and Agency for Health care Research and Quality.39 These include exacerbations44 (primary outcome), health care utilization,45 composite scores,50 and pulmonary physiology measures.47
We defined the primary outcome measure, asthma exacerbations, using the recommended observational study standards for exacerbation measurement from the Asthma Outcomes workshop.44 Specifically, we defined an exacerbation as at least 1 of the following qualifying events, with qualifying events occurring within 14 days of each other defining a single exacerbation.
An emergency department or inpatient visit with a primary diagnostic code for asthma.
A cluster of 2 visits of at least one of the following 2 types within 1 and 14 days: a) an outpatient visit (primary care or subspecialty) with a primary diagnostic code for asthma, or b) an ED, inpatient (IP), or outpatient visit with any diagnostic code (not just primary) for asthma. We excluded visits on the same day to avoid double counting the same visit.
Any ED, IP, or outpatient visit with an ICD-9 code for asthma that has a fifth digit, or a diagnosis text string, indicative of an exacerbation.
Any prescription or fulfillment of a systemic corticosteroid medication from 0 to 3 days after the date of any type of visit where the visit includes a diagnostic code for asthma. Medication codes for systemic steroids were identified using Generic Product Identifier (GPI) codes. As prescription duration data showed high rates of missing data, we did not include steroid prescription duration in this definition.
For exacerbation criteria events, and 2 events within a 14-day span were considered the same exacerbation; thus, 3 or more events could create an exacerbation with a duration of more than 14 days. This is based on evidence showing a median 10-to-14-day duration of typical asthma exacerbations.48 For further details of the exacerbation definition, please see the Technical Appendix.
In accordance with the Asthma Outcomes Workshop recommendations, we also provide descriptive statistics on the specific components of the exacerbation definition: asthma-specific ED, IP, and outpatient (OP) visits, and steroid prescriptions. We also provide summary statistics for the other categories of asthma medications prescribed in each period.
The second category of outcome measures is health care utilization events. Here we report each of the 3 visit type categories—IP, ED, and OP—as well as asthma-specific medication use (reliever or controller medications). Due to duplicate medications occurring within both the clinical and claims data, we deduplicated medication records by person, start date, and by GPI code to avoid double counting the same prescription.
The third category of outcome measures is composite symptom scores—namely, the ACT values. The range for the ACT is 5 to 25 and the Childhood ACT range is 0 to 27. For both versions, a score less than 19 is considered poor control and thus ACT results were dichotomized at 19.
The fourth category of outcome measures is physiologic measures, including the results of spirometry (FEV1/FVC ratio percent predicted values49,50) and of peak expiratory flow monitoring. For descriptive statistics, the median was reported for patients with >1 observation recorded. For analyses, we dichotomized forced expiration at 80% of the FEV1 predicted value.
Covariates
We adjusted for those variables available in the dataset that were potential confounders of the association between the CATP and asthma control. These include patient demographics (age, sex, race/ethnicity), health care insurance coverage and chronic medical complexity. We categorized age using the categories defined in the age-specific guideline recommendations in the National Asthma Education and Prevention Program guideline on asthma management.5 We categorized race and ethnicity using the categories present in MCPN′s EHR. Race and ethnicity are documented through each clinic's patient registration process at the time of initial registration in the MCPN system.
We defined health care insurance coverage as the number of months of Medicaid eligibility for each patient during the study period. Because we limited the cohort to patients with at least 1 month of Medicaid eligibility, our sample included no patients with zero months of eligibility.
To measure medical complexity of each patient in the cohort, we used the Health care Cost and Utilization Project's Chronic Condition Indicator (CCI) tool's 17 body system categories. For each patient, we counted the number of body systems affected by CCIs, excluding the category for diseases of the respiratory system, as every cohort member had a condition in this category (asthma).51
Statistical Methods
GLMMs were used to evaluate prepost changes in process, health, and utilization outcomes within-patient. A random effect was included to account for correlation among observations from the same clinic. Models where comparisons were made between preintervention and postintervention on paired data from individuals also included a random effect for individual-level correlation. Count variables were assumed to follow Poisson distributions when the means were approximately equal to the variances. For all binary outcomes, binomial GLMMs were fit with logit link functions. Data cleaning was performed in R (R Project for Statistical Computing, Vienna, Austria, Version 3.3.3) and SAS (Version 9.4m4, Cary, NC) and all models were fit in SAS using the PROC GLIMMIX procedure.
Results
Sample Characteristics
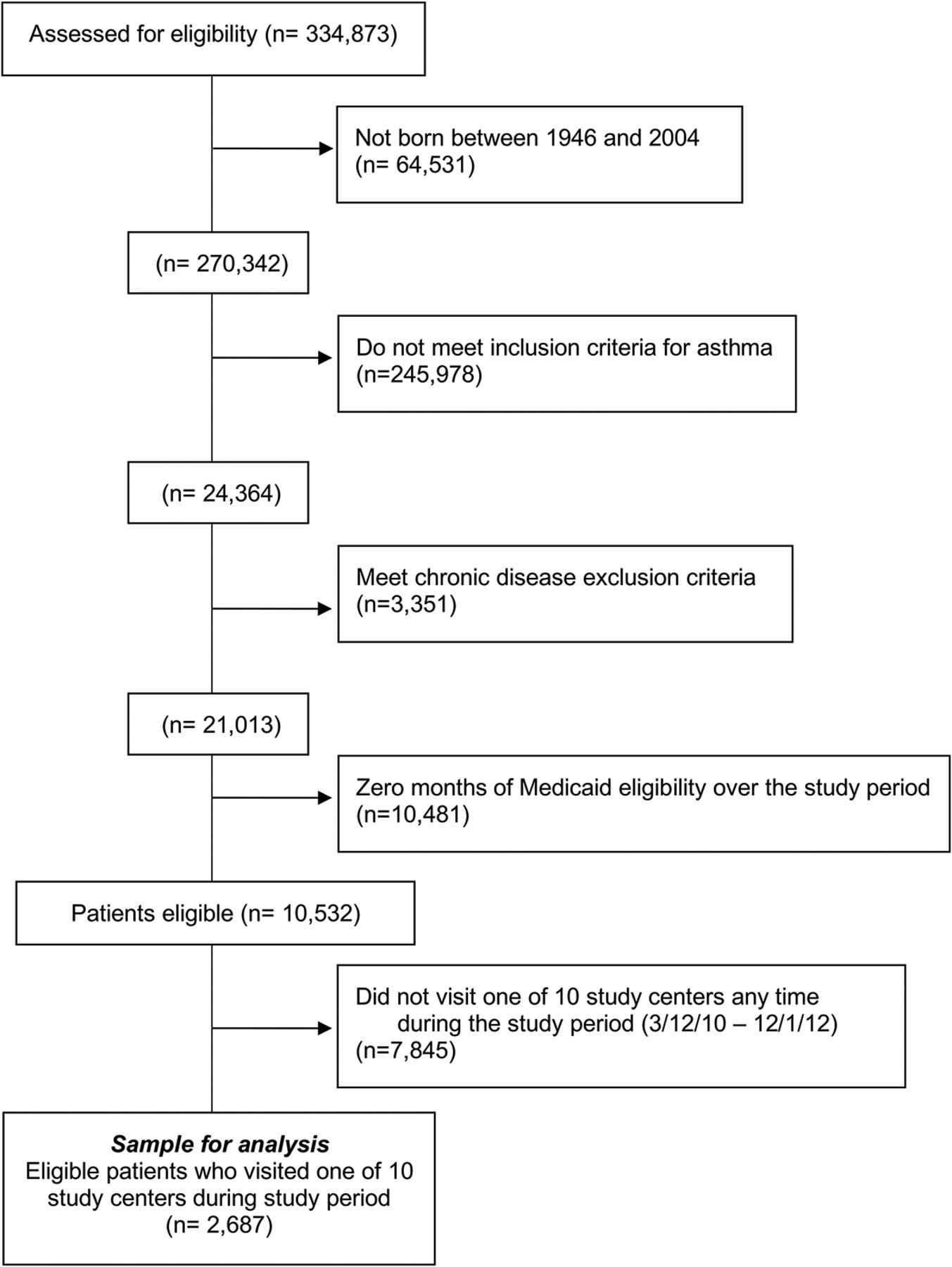
After applying inclusion and exclusion criteria, the resulting asthma study cohort included 2687 patients (Figure 2). The median age was 23 years, with 58.3% of patients in the adult age range (18 to 64 years), and 66.5% were female (Table 1). More than half (51.8%) had unknown race, with 32.5% reported as white race and 10.9% as black race. By ethnicity, 31.8% were Hispanic/Latino, 46.7% were not Hispanic/Latino and 21.6% had unknown ethnicity. The count of comorbidity categories were as follows: 12.6% had none and 52.1% had more than 2. The median duration of Medicaid eligibility was the full study period duration—33 months—with 89.5% having at least 20 months of eligibility.

The study cohort flow diagram.
Asthma Cohort Demographics
Process Outcomes
For process measures, rates pre- and postintervention were mixed (See Table 2. Both types of asthma severity assessment—spirometry and ACT performance—increased significantly from pre- to postintervention; Table 2) The 2 NQF-endorsed HEDIS process measures—asthma medication ratio and medication management for people with asthma—did not change significantly from pre-to postintervention, although the percentage of patients meeting the HEDIS definition criteria for “persistent asthma” (the measure denominator for both measures) did increase significantly from 4.8% to 8.5% of the cohort, largely driven by more patients meeting medication-dispensing criteria for asthma in the postintervention period.
Process Measures
Health Outcomes
Exacerbations
As shown in Table 3, during the study period, 581 (21.6%) patients experienced at least 1 asthma exacerbation, with a total of 1063 exacerbations; 356 experienced 1 exacerbation, 119 experienced 2, 52 experienced 3, and the remaining 54 experienced 4 or more exacerbations. The rate of exacerbations did not change between pre- and postintervention, nor did the proportion with each of the 4 exacerbation qualifying events in our study definition of exacerbation.
Outcome Measures
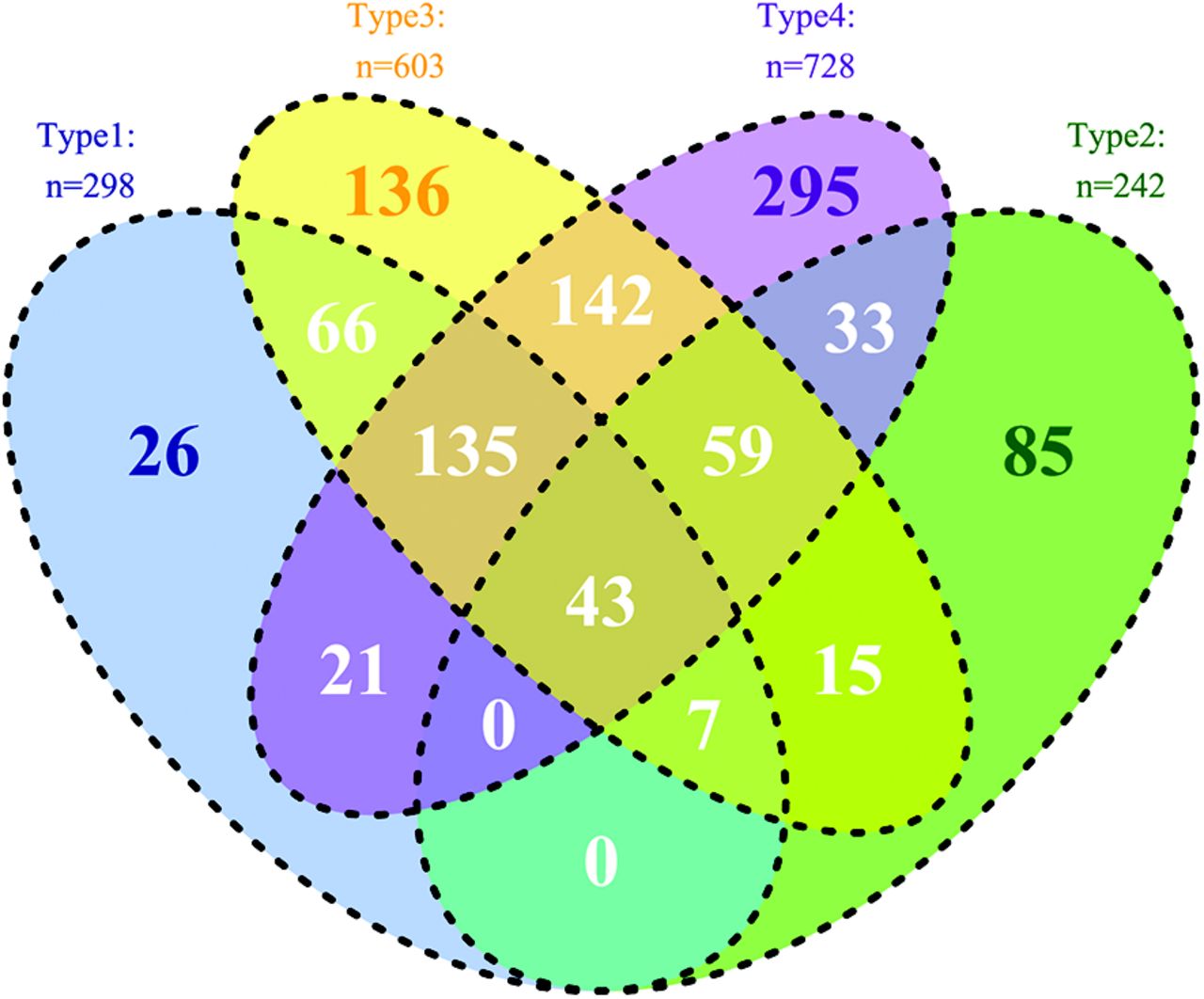
Of the 4 qualifying events in the study definition of an exacerbation, the most common was a type 4 event (systemic corticosteroid medication, 728 events), although we found that many exacerbations were characterized by more than 1 event type (Figure 3). For example, of the 728 exacerbations that included a type 4 event, 433 included at least 1 other qualifying event type. None of the event types changed in frequency between the pre- and postintervention periods (Table 3).

Distribution of exacerbations by qualifying event. Type 1: single Emergency Department (ED) or inpatient (IP) visit with primary diagnosis of asthma. Type 2: cluster of 2 visits with asthma diagnosis <14 days apart. Type 3: ICD code or string indicating exacerbation. Type 4: systemic corticosteroid within 0 to 3 days after any type of asthma visit. Note: exacerbations occurring within 14 days of each other were grouped into a single exacerbation.
Utilization Outcomes
As shown in Table 3, for the utilization outcomes, the number of ED, IP, and OP visits for asthma were similar pre- and postintervention. The number of asthma-specific medication events (prescriptions, dispensing events) rose by 36.3% from 5221 to 7116. This increase occurred for both controller medications (34.3% rise) and relievers (37.7% rise).
We could not analyze composite asthma score values as an outcome as there were no ACTs measured in the preintervention period. This was expected, as the ACT was part of the intervention. For our pulmonary physiology outcome, we found no change in the FEV1/FVC percent predicted values pre- to postintervention.
Discussion
In this prepost analysis of the CATP in one network of federally qualified health centers, we found improvement in some process measures of asthma care associated with the intervention: increased use of spirometry and administration of the ACT measure. At the same time, no change occurred in the 2 HEDIS asthma process measures: asthma-medication ratio and medication management for people with asthma. We also found no change in asthma outcomes measured across multiple domains: exacerbations, utilization, symptom scores, and pulmonary physiology measures.
These findings are similar to those of prior studies of asthma care processes associated with CATP implementation. One prior study of the CATP found that practices reported they increased their use of inhaled corticosteroids, increased their use of asthma action plans, and initiated or increased their use of spirometry.24 An analysis of the MCPN CATP intervention using only EHR data found increased use of spirometry, severity assessments, asthma action plans, and prescription of inhaled corticosteroids.32 Although we could not measure asthma action plan use in our current study, we confirmed using SAFTINet data that both spirometry and ACT measurement improved. Unlike these 2 prior CATP studies, the current study also assessed asthma outcomes but found no change.
A plethora of evidence using the Reach-Effectiveness-Adoption-Implementation-Maintenance (RE-AIM) Framework has shown that consistent implementation of an intervention (eg, CATP process of care) is prerequisite for realizing effectiveness in real-world care settings.52,53 The lack of effects on outcomes in this study may be attributable to the limited changes in guideline-adherent process of care. While spirometry and ACT use increased, simply measuring asthma control was not enough to change either medication management (reflected in the 2 HEDIS measures) or patient outcomes (Figure 1). Further attention to taking action on observing poor control is needed. The finding that measuring asthma control is not sufficient to make an impact reflects findings from other domains of primary care—for instance, implementation of the PHQ-9, a recommended tool for measuring symptoms of depression, does not in and of itself improve depression outcomes.54
Among our secondary outcomes, the only change was a rise in the number of asthma controller and reliever medications prescribed or fulfilled. This increase also explained the rise in the number of patients meeting HEDIS measure denominator criteria (persistent asthma). This is consistent with the rise in controller medication administration reported in the 2 prior CATP studies.24,32
Targeting specific provider behaviors reflecting change in processes of care is important because practice change is an essential step toward changing outcomes. Nonetheless, as reflected in these findings, changing provider behaviors is no guarantee of change in outcomes, which are influenced by a host of variables including patient-level adherence to treatment55 and the unique characteristics of the patient population served by the practice and the characteristics and context of the practices themselves.56 Further improvements in provider behaviors may yield greater effectiveness at the patient level. A survey of 784 primary care providers concluded that continuing medical education programs addressing respiratory disease management had not adequately reached primary care practices, and that clinicians were less interested in attending distant sessions with opinion leaders, preferring live presentations, information they could access from their office, and content relevant to their daily practice.57 Tailored approaches that engage providers and include multiple opportunities for interaction and feedback are markedly more likely to change practice behavior.58 These training guidelines have been adopted in the CATP.
Still, additional research is needed to further improve CATP training and with it to improve patient outcomes. Results from this study of processes of change can help inform such refinements to the CATP, continuing to improve care delivery with the objective of decreasing asthma symptoms and health care utilization. Informal feedback from providers participating in CATP have indicated a desire for more follow-up training to include spirometry interpretation and decision support through case studies. Future directions include exploration of which elements of the provider-level CATP implementation are most effective in improving process measures, and in collecting process and outcome measures more specifically related to the components of the CATP intervention. For example, if future training involves more emphasis on ACT interpretation and decision support—shown to improve outcomes elsewhere—future process and outcome measures could quantify provider concordance with recommended responses to ACT values, and the associated asthma symptom burden or exacerbation in the weeks following each ACT measurement.
The current study also describes the distribution of asthma exacerbation events operationalized using hybrid (claims-and-EHR) data. Although prior studies have used the Asthma Outcomes standards for exacerbations,44,59 we found no prior studies detailing the distribution of exacerbations defined using observational data by type of qualifying event. The fact that 295 exacerbations were characterized by systemic corticosteroid prescribing or prescription-filling alone suggests that these may represent a different, milder form of exacerbation than those exacerbations also characterized by asthma-related ED and/or inpatient events.
Several types of bias are possible given the prepost, nonexperimental design, including selection bias and confounding. Selection bias (nonrandom selection into the study population) could be introduced by improved asthma detection—perhaps more so with milder asthma severity—following the intervention. As we included the same study population in both pre- and postintervention study populations, this bias is unlikely to impact our findings. Confounding may have been introduced by a secular trend—for example, if the pre- or postintervention periods differed in the severity of asthma triggers in the regional environment, such as seasonal allergens or circulating respiratory viruses. Given the lack of a control group, any number of other influences on asthma processes of care may have led to the effects observed in this study. Subsequent research should include pragmatic trial and quasi-experimental designs to test both the implementation and the effectiveness of CATP in diverse clinical settings.64
In conclusion, although we found improvement in some process measures of asthma care in this prepost analysis of the CATP in one network of practices, we found no change in asthma outcomes measured across multiple domains: exacerbations, utilization, symptom scores, and pulmonary physiology measures. Future directions may include a randomized trial of the toolkit in another setting, and subgroup analysis of findings based on exacerbation-qualifying events.
Technical Appendix
Selection and Description of Participants
Inclusion criteria included age between 5 and 64 years by the start of the study period (3/12/2010 to 12/1/2012); at least 1 visit to 1 of the participating Metro Community Provider Network (MCPN) practices during the study period; at least 1 month of Medicaid eligibility during the study period; and either a diagnostic code or medication prescription or fulfillment indicative of asthma.
1. Age Inclusion Criteria
Inclusion criteria included age between 5 and 64 years old, inclusive, by the start of the study period (3/12/2010 to 12/1/2012). We exclude patients less than 5 years old because of the difficulty in obtaining objective diagnostic criteria (spirometry values) in young children and the common occurrence of wheeze and other asthma-like symptoms in viral respiratory illnesses in young children.1 We excluded patients 65 years and older because of the diagnostic difficulty in distinguishing chronic obstructive pulmonary disease from asthma in older patients and because patients in this age-group are Medicare-insured and our dataset did not contain Medicare claims data. As the SAFTINet dataset only includes year of birth, based on the study years (2010 to 2012) we defined our cohort as those born during or after 1946 and before or during 2004.
2. Linkable to an Intervention Practice
To be included, each patient had to have at least 1 visit of any type during the study period at 1 of the 9 MCPN study practices.
3. Medicaid Eligibility Inclusion Criteria
As our primary outcome measure and other measures included criteria available only in claims (Colorado Medicaid) data, we excluded patients who had no months of Medicaid coverage during the study period.
4. Diagnostic code or medication prescription or fulfillment indicative of asthma
Inclusion criteria used to identify patients with asthma were: either a diagnostic code or a medication (prescription or fulfillment) event indicative of asthma. Inclusion and exclusion diagnoses were available in 2 formats: either numeric (ICD-9 code) or free text in 1 of the diagnosis fields.
4a. Diagnostic codes indicative of asthma
INCLUSION asthma diagnosis events
In defining asthma diagnosis events, we first selected all patients with an ICD-9 code for asthma. We used all 493 codes except 493.20, 493.21, and 493.22, as these 3 5-digit codes are used to indicate chronic obstructive pulmonary disease. From this group of patients with an asthma ICD-9 code, we then compiled asthma synonyms from among the free text diagnoses assigned to each patient in electronic health record data (claims data only contains ICD-9 codes as diagnoses). From these, we derived the following list of strings:
“asthma,” “exercise induced bronchospasm” and “reactive airway”
From among the remaining patients with no ICD-9 code for asthma, we then selected all who had a diagnosis field containing 1 of these 3 strings. We then inspected the free-text diagnosis fields for all patients in this second group, and thereby derived exclusion strings—strings indicative of either diagnostic uncertainty
“?”, “r/o” (abbreviation for “rule out”) and “possible”
or a diagnosis relevant to a family member but not the patient:
“fh of,” “family hx of,” “fh”:, “fhx”: and “fhx of”
To define inclusion and exclusion strings for asthma, we first perused all free-text diagnoses assigned to patients with either an ICD-9 code for asthma or an asthma-specific medication (more on medications below) and identified all strings that included “asthma” or a synonym thereof. We then searched for these strings in the list of patients meeting inclusion criteria 1 to 3, above, and identified additional strings that indicated uncertainty about the diagnosis in the patient—these exclusion strings contained abbreviations for “rule out,” “possible” or “family history of.”
Thus, the following constituted our definition of a diagnosis of asthma:
ICD-9 code 493.XX excluding 493.20, 493.21, and 493.22
Or strings:
o Include if diagnosis field contains: “asthma,” “exercise induced bronchospasm” or “reactive airway”
o But not if it contains: “?”, “r/o,” “possible,” ”fh of,” “family hx of,” “fh”:, “fhx”: or “fhx of”
EXCLUSION diagnostic codes
We excluded patients from the cohort who during the study period or 5 years before study inception had a diagnostic code contained in the HEDIS Core Value Sets2 excluded in the HEDIS measures for asthma.3,4 We used an approach similar to that used in defining asthma diagnosis events, described above. We started with the ICD-9 codes for each of the excluded value sets:
Acute respiratory failure: ICD-9 code 518.81
Chronic respiratory conditions due to fumes/vapors: ICD-9 code 506.4
COPD: ICD-9 codes 493.20, 493.21, 493.22, 496
Cystic fibrosis: ICD-9 code 277.0
Emphysema: ICD-9 codes 492.0, 492.8
Obstructive chronic bronchitis: ICD-9 codes 491.20, 491.21, 491.22
Other emphysema: ICD-9 codes 518.1, 518.2
In defining asthma exclusion diagnosis events, we first selected all patients with an ICD-9 code for 1 or more of these exclusion diagnoses. From this group of patients, we then compiled diagnostic name synonyms from among the free text diagnoses assigned to each patient. From these, we derived the following list of strings:
Acute respiratory failure: “acute respiratory fa”
Chronic respiratory conditions due to fumes/vapors: “fume” or “vapor”
COPD: “COPD,” “chronic obstructive” “chronic obst” or “chrn obst”
Cystic fibrosis: “cystic fibros” and “cystic fibrosis”
Emphysema: “emphys” and “emphysema
Obstructive chronic bronchitis: “chronic bronchitis”
Other emphysema: no additional strings other than the inclusion/exclusion for Emphysema, above
From among the remaining patients with no ICD-9 code for at least 1 exclusion diagnosis, we then selected all who had a diagnosis field containing 1 of these 3 strings. We then inspected the free-text diagnosis fields for all patients in this second group, and thereby derived exclusion strings. We arrived at the same list as we derived for asthma diagnosis events: strings indicative of either diagnostic uncertainty or a diagnosis relevant to a family member but not the patient.
Thus, the following constituted our definition of an exclusion diagnosis:
Acute respiratory failure
o ICD-9 code 518.81
o strings:
include if contains “acute respiratory fa”
exclude if also contains “?”,“possible,” ”r/o“ or ”fh of,” “family hx of,” “fh”:, “fhx”: or “fhx of”
Chronic respiratory conditions due to fumes/vapors
o ICD-9 code 506.4
o strings:
include if contains “fume” or “vapor”
exclude if also contains “?”,“possible,” ”r/o“ or ”fh of,” “family hx of,” “fh”:, “fhx”: or “fhx of”
COPD
o ICD-9 codes 493.20, 493.21, 493.22, 496 – we will keep the 493's in this exclusion
o strings:
include “COPD,” “chronic obstructive” “chronic obst” or “chrn obst”
exclude if also contains “?”,“possible,” ”r/o“ or ”fh of,” “family hx of,” “fh”:, “fhx”: or “fhx of”
Cystic fibrosis
o ICD-9 code 277.0
o strings:
■ include “cystic fibros” and “cystic fibrosis”
■ exclude (same as for others: if also contains “?”,“possible,” ”r/o“ or ”fh of,” “family hx of,” “fh”:, “fhx”: or “fhx of”) or “gene” or “carr”
Emphysema
o ICD-9 codes 492.0, 492.8
o strings:
■ include “emphys” and “emphysema
■ exclude if also contains “?”,“possible,” ”r/o“ or ”fh of,” “family hx of,” “fh”:, “fhx”: or “fhx of”
Obstructive chronic bronchitis
o ICD-9 codes 491.20, 491.21, 491.22
o strings:
■ include “chronic bronchitis”
■ exclude if also contains “?”,“possible,” ”r/o“ or ”fh of,” “family hx of,” “fh”:, “fhx”: or “fhx of”
Other emphysema
o ICD-9 codes 518.1, 518.2
o strings:
■ no additional strings other than the inclusion/exclusion for Emphysema, above
4b. Medication codes for asthma
As medications, we included any prescription (from electronic health record data) or fulfillment (from claims data) during the study period of at least 1 asthma medication from the HEDIS list “Asthma Controller and Reliever Medications.”5
To identify medications on this list, first we identified all medications with the Generic Product Identifier (GPI) codes assigned to the category asthma medications (initial digits of 44) and assigned these to the appropriate category–controller or reliever. To assign medications to controller or reliever categories, we used the HEDIS list5 and assigned all medications categorized as “short-acting inhaled β-2 agonists” to the “reliever” category and all others to the “controller” category. Our second step was to identify medications without a GPI number that had the identical name to a medication with a GPI number starting with 44, and assigned these to the appropriate category (controller or reliever). Our third step was to identify common strings from the medication names in the list with GPI codes and search for these strings in medication prescriptions that had no GPI code. If there was a valid match, we assigned the GPI code-less prescriptions to the appropriate medication category (controller or reliever). We deduplicated medication records by person, start date, and by GPI code.
Process Measure Specifications
Persistent Asthma Subgroup Definition
For the 2 HEDIS process measures for asthma, we applied the measure specifications to derive a subgroup of patients with persistent asthma—the denominator group for these 2 measures.6,7 We derived denominator elements from claims data only so as to avoid double-counting visits or prescriptions that occurred in both claims and electronic health record data.
First, we identified members as who met at least 1 of the following criteria during each year of a 2-year period. Criteria need not be the same across both years.
At least 1 ED visit with asthma as the principal diagnosis, using all 493 ICD-9 codes except 493.20, 493.21, and 493.22 to define asthma
At least 1 acute inpatient encounter with asthma as the principal diagnosis, using all 493 ICD-9 codes except 493.20, 493.21, and 493.22 to define asthma
At least 4 outpatient asthma visits with asthma as 1 of the listed diagnoses (using all 493 ICD-9 codes except 493.20, 493.21, and 493.22 to define asthma) and at least 2 asthma medication dispensing events. As medications, we included any fulfillment (from claims data) from the HEDIS list “Asthma Controller and Reliever Medications.”5
At least 4 asthma medication dispensing events, defined by the HEDIS list “Asthma Controller and Reliever Medications.”5
Second, for those meeting criteria for the fourth bullet—at least 4 asthma medication dispensing events—where leukotriene modifiers were the sole asthma medication dispensed in that year, to be included they must also have at least 1 diagnosis of asthma (using all 493 ICD-9 codes except 493.20, 493.21, and 493.22 to define asthma) in any setting, in the same year as the leukotriene modifier.
To define 2-year periods for the pre- and postintervention periods, we used the preintervention period (12 March 2010 - 11 March 2011) and the year prior (12 March 2009 - 11 March 2010) for the preintervention period measurement, and the postintervention period (2 December 2011 - 1 December 2012) and the year before it (2 December 2010 – 1 December 2011) to define the postintervention period measurement. Multiple asthma medication prescriptions on the same day were treated as a single asthma dispensing event.
The table below shows the number of patients defined as having persistent asthma using this definition by measurement period.
Outcome Measure Specifications
Asthma Control Test
For the Asthma Control Test (ACT), we used the childhood version for children age 5 to 11 years (asking the parent to complete it on behalf of the child) and the adult version for ages 12 to 64 years. The range for the ACT is 5 to 25 and the Childhood ACT range is 0 to 27; for both versions, a score less than 19 is considered poor control and thus ACT results were dichotomized at 19.
Exacerbation Definition
We derived our definition of an asthma definition from the recommendations of an expert panel convened in 2012 by the National Institutes of Health and other federal agencies.8 The expert group proposed how asthma exacerbation should be assessed as a standardized asthma outcome in future asthma clinical research studies, using comprehensive literature reviews and expert opinion to compile a list of asthma exacerbation outcomes. The expert panel definition from which we derived our measure is as follows:
An “asthma-specific” inpatient or emergency/urgent care visit with a primary diagnosis of asthma, OR
A prescription for systemic steroids.8
We derived 4 “qualifying events” defining an exacerbation, any of which would constitute the first of the 2 measure. The first 3 correspond to the first expert panel criterion and the fourth correspond to the second expert panel criterion.8 To identify an event as asthma-related, we used the same asthma-diagnosis inclusion/exclusion criteria (“asthma diagnosis criteria”) for the Cohort Definition, described above in Diagnostic codes indicative of asthma.
Number of Patients Defined as Having Persistent Asthma by Measurement Period
Exacerbation Qualifying Events
1. Any Single Asthma-Specific Emergency Department (ED) or Inpatient (IP) Visit
For the first exacerbation qualifying event, we included all ED and IP visits that had a primary diagnostic code of 493.XX excluding 493.20, 493.21, and 493.22. For both types of visits, the entire duration of the visit was included in the exacerbation. Thus, if an inpatient visit lasted 10 days and then there was an ED visit 5 days after the end-date of the inpatient visit, this still counted as a single exacerbation event because the ED visit was within 14 days of the end-date of the inpatient visit.
2. A Two-Visit Combination Including an Outpatient Visit with a Primary Diagnosis of Asthma
For the second exacerbation qualifying event type, we included groupings of at least 2 visits of any type (ED, IP, outpatient) occurring within 1 to 14 days of each other where
both visit records contain a diagnosis of asthma (primary, nonprimary) AND
1 of these visits is an outpatient visit that contains a primary diagnostic code that meets the Asthma Diagnosis Criteria above. This could be either
o a claims record for an encounter with a primary dx flag for asthma
o a visit for which all diagnoses are asthma diagnoses
We excluded visits occurring on the same day to avoid double-counting the same visit.
3. Asthma-Specific Visit with a Diagnostic Code or String Indicating an Exacerbation
For the third exacerbation qualifying event, we selected all encounters with a diagnosis indicative of an asthma exacerbation. To define diagnoses indicative of exacerbations we used an approach like that used in defining asthma diagnosis events, described above. We started with the ICD-9 codes for asthma exacerbations—specifically any ICD-9 code 493.XX (excluding 493.20, 493.21, and 493.22) with fifth digit of either 1 or 2.
From this group of patients, we then compiled diagnostic name synonyms for an asthma exacerbation code from among the free text diagnoses assigned to each patient. From these, we derived the following list of strings: “active” “acute” “attack” “flare” or “exacerbation” “status.”
From among the remaining patients with no ICD-9 code indicative of an exacerbation, we then selected all who had a diagnosis field containing 1 of these strings. We then inspected the free-text diagnosis fields for all patients in this second group, and thereby derived exclusion strings. We arrived at the same list as we derived for asthma diagnosis events: strings indicative of either diagnostic uncertainty or a diagnosis relevant to a family member but not the patient.
Thus, the following constituted our definition of a diagnosis indicative of an exacerbation:
ICD-9 code 493.XX (excluding 493.20, 493.21, and 493.22) with fifth digit of either 1 or 2
Strings:
o Include if contains ”active“ ”acute“ ”attack“ ”flare“ or ”exacerbation“ ”status.”
o exclude if also contains “?”,“possible,” ”r/o“ or ”fh of,” “family hx of,” “fh”:, “fhx”: or “fhx of”
4. A Systemic Corticosteroids Prescription or Fulfillment Event Associated with an Asthma-Related Visit
For the fourth exacerbation qualifying event, we included any systemic steroid prescription or dispensing that occurred between the initial date of any type of visit and 3 days after the end date of the visit when that visit included a diagnostic code or string that met asthma diagnosis criteria for the Cohort Definition, described above in Diagnostic codes indicative of asthma. The date associated with this event is the date of the medication (prescribed or filled). If both the prescribed date and the fill date are within 3 days after the visit date, we took the fill date as the date of the exacerbation qualifying event. As for controller and reliever medications, we deduplicated medication records by person, start date, and by GPI code. As prescription duration data showed high rates of missing data, we did not include steroid prescription duration in this definition.
To define systemic corticosteroids, first we identified all medications with the GPI codes assigned to the category systemic corticosteroids (initial digits of 22). Our second step was to identify medications without a GPI number that had the identical name to a medication with a GPI number starting with 22. Our third step was to identify common strings from the medication names in the list with GPI codes and search for these strings in medication prescriptions that had no GPI code. If there was a valid match, we included these codes. Finally, we checked to make sure we had included all medication names that matched those in the HEDIS Table PCE-C: Systemic Corticosteroids.9
Clustering of Exacerbation Criteria
Qualifying events that occur within 14 days of each other are considered the same exacerbation event. This is based on evidence showing a median 10 to 14-day duration of typical asthma exacerbations.10 If 15 days occur between exacerbation qualifying events, these count as 2 separate exacerbations.
Covariate Measure Specifications
Chronic Conditions Indicator
To characterize our study population by comorbid chronic medical complexity, we used a count of the number of chronic condition categories for each patient. To quantify chronic conditions, we used the Health care Cost and Utilization Project (HCUP)'s Chronic Condition Indicator (CCI) tool11 to count the total number of body systems, out of the 17 included in the CCI tool, affected by CCIs for each patient.
Using an approach similar to what we used in defining asthma diagnosis events, described above, we first used all ICD-9 codes in the CCI tool to assign CCI's to patients. We then performed a string search for the ICD-9 text labels in the CCI groups and included those diagnostic free text strings that matched these strings. Because all patients in the study cohort met criteria for the CCI's respiratory system category, we eliminated this group from our chronic conditions variable. The chronic conditions variable was a count of the number of CCI's per person.
The distribution of CCI body systems in our study sample was as follows:
Exacerbation-Qualifying Events in This Patient Population
Notes
This article was externally peer reviewed.
Funding: The work described in the article and the writing of the article were funded by grant 5R21HL123589-02 from the National Heart, Lung, and Blood Institute.
Conflict of interest: none declared.
To see this article online, please go to: http://jabfm.org/content/32/1/37.full.
- Received for publication May 24, 2018.
- Revision received September 30, 2018.
- Accepted for publication October 2, 2018.




{kind=link}
{kind=link}
{kind=link}