
Abstract
Objective: Primary care providers should counsel overweight patients to lose weight. Rates of self-reported, weight-related counseling vary, perhaps because of self-report bias. We assessed the accuracy and congruence of weight-related discussions among patients and physicians during audio-recorded encounters.
Methods: We audio-recorded encounters between physicians (n = 40) and their overweight/obese patients (n = 461) at 5 community-based practices. We coded weight-related content and surveyed patients and physicians immediately after the visit. Generalized linear mixed models assessed factors associated with accuracy.
Results: Overall, accuracy was moderate: patient (67%), physician (70%), and congruence (62%). When encounters containing weight-related content were analyzed, patients (98%) and physicians (97%) were highly accurate and congruent (95%), but when weight was not discussed, patients and physicians were more inaccurate and incongruent (patients, 36%; physicians, 44%; 28% congruence). Physicians who were less comfortable discussing weight were more likely to misreport that weight was discussed (odds ratio, 4.5; 95% confidence interval, 1.88–10.75). White physicians with African American patients were more likely to report accurately no discussion about weight than white physicians with white patients (odds ratio, 0.30; 95% confidence interval, 0.13–0.69).
Conclusion: Physician and patient self-report of weight-related discussions were highly accurate and congruent when audio-recordings indicated weight was discussed but not when recordings indicated no weight discussions. Physicians' overestimation of weight discussions when weight is not discussed constitutes missed opportunities for health interventions.
The prevalence of obesity in the United States remains high, with corresponding comorbidity and mortality.1⇓⇓–4 Thus, preventing and managing obesity is vital. Physician counseling or referral to intensive behavioral interventions might promote patient weight loss.5⇓⇓⇓–9 However, before physician counseling or referral can be effective, patients must first receive a message related to their weight. Wide variation exists between patient and provider recall of weight-related discussions.10⇓⇓⇓⇓⇓⇓–17 Greiner et al10 showed that physician reports of weight discussions are not always congruent with patient reports; however, they did not compare physician reports to objective records of what they discussed. None has used audio recordings to verify the accuracy and congruence of weight-related discussions among physicians with overweight and obese patients.8,18⇓–20 The purpose of this study was to compare audio-recorded visits of weight-related discussions with patient and physician reports. A secondary aim was to assess whether any patient-, physician-, or visit-level factors predict the accuracy of patient or physician reports.
Methods
This study's methodology has been described elsewhere.8 In brief, Project CHAT (Communicating Health: Analyzing Talk) was a 3-year observational study that audio-recorded preventive and chronic care encounters. The study was approved by the Duke University School of Medicine Institutional Review Board.8
Physician Recruitment
Research staff approached 54 primary care physicians in community-based practices in North Carolina. Of these, 42 consented; however, 2 physicians withdrew before contacting patients, leaving 40 physicians participating in the study. Physicians were told the study would assess how they discussed preventive health with their patients (the focus on weight was not disclosed). After signing written consent, physicians completed a baseline questionnaire that assessed demographic factors and contained questions regarding their beliefs about counseling about weight, nutrition, and physical activity (PA). To mask the focus on weight, the questionnaire included the same questions for smoking and alcohol use.
Patient Recruitment
Research staff reviewed scheduled appointments via physicians' electronic schedules to identify patients scheduled for visits 3 weeks in advance. Staff mailed patients a letter signed by their physician that described the study as examining how physicians discuss preventive health. Patients could opt out. One week later, research staff called patients to assess eligibility and conduct a baseline questionnaire that assessed demographic factors (including height and weight for self-reported body mass index [BMI]) and psychosocial factors associated with improving weight, nutrition, and PA. Questions about smoking and alcohol use were included to help mask the focus on weight.
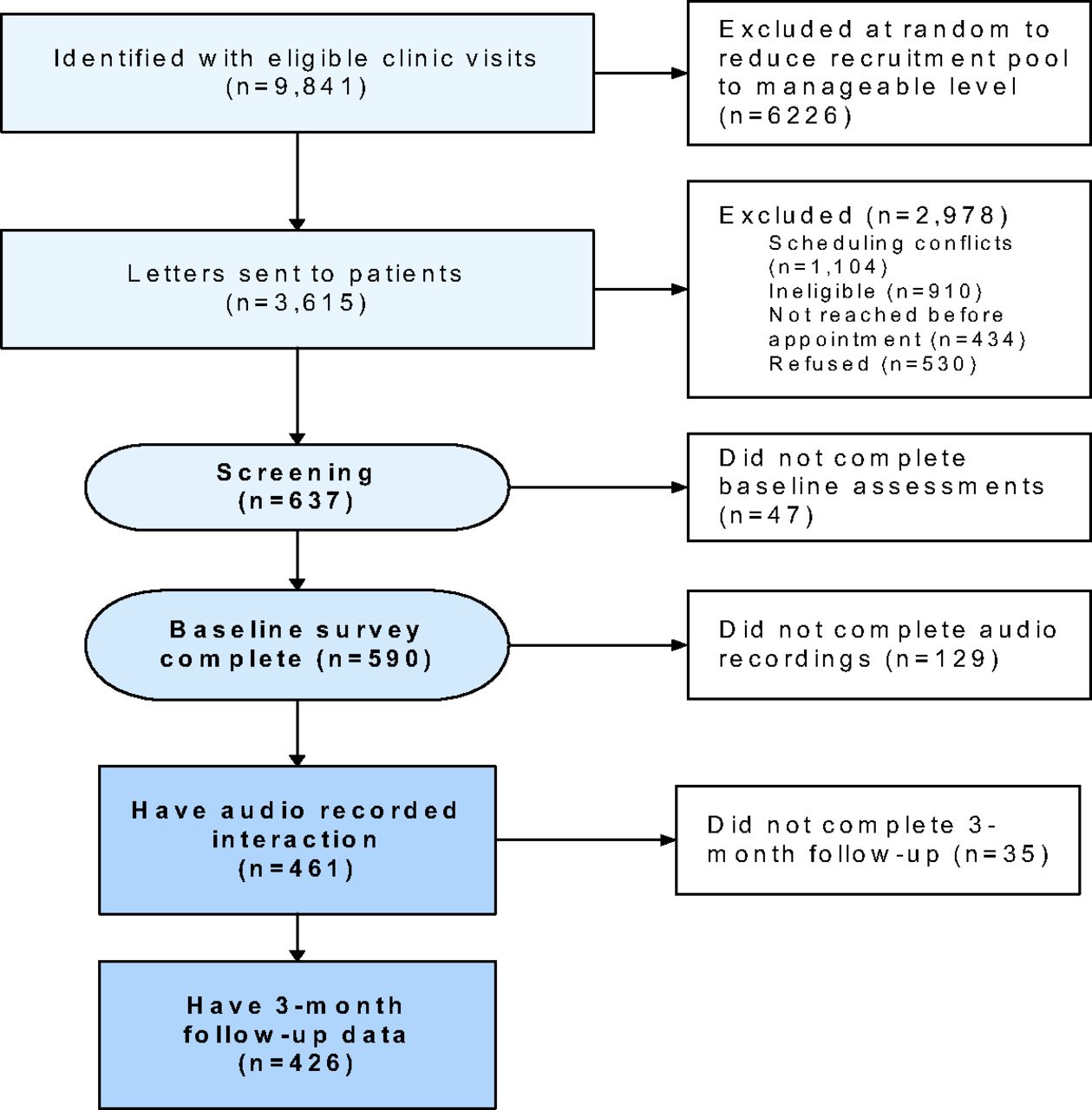
Patients were eligible if they spoke English; were ≥18 years old, cognitively competent, and not pregnant; and had a BMI ≥25. Of the patients contacted, 461 eligible patients gave written consent and participated in the study. Figure 1 shows the patient recruitment flowchart.

Patient recruitment flowchart.
Data Collection
Research staff inconspicuously placed audio recorders in the examination room and activated them before the clinical encounters. Immediately after the visits, research staff met with patients to verify their self-reported BMI using stadiometers and calibrated scales. Research staff then administered a questionnaire that asked patients to respond yes or no if during the encounter their physician discussed surgery or medication related to weight or asked them about, gave advice for, assessed readiness to change for, assisted with, or referred them to a specialist for diet, PA, or weight. Staff assessed patients' vital signs to mask the focus on weight. To avoid interrupting the flow of the clinic, staff administered a short, easy to complete, and less comprehensive survey with physicians after the visits. Physicians were asked to respond yes or no if during the encounter they had discussed diet, PA, BMI/weight, smoking, or alcohol use with their patients.
Data Analysis
In the audio recordings, coders confirmed 3 primary weight-related topics raised either by physicians or patients: diet, PA, and BMI/weight. Coders used a detailed codebook that provided specific instructions, including precise definitions of codes and examples. A weight-related topic was defined as any mention of weight/BMI, diet/nutrition, or exercise/PA by the patient or physician. Four coders were rigorously trained (by SA) for 20 hours to identify weight-related content until a high level of reliability was achieved. All 4 coders coded a random sample of 20% of all audio recordings to obtain interrater reliability of the coding system. Cohen's κ was used to calculate interrater reliability for each segment. All coders had strong agreement (diet: Cohen's κ = 0.79, 95% confidence interval [CI], 0.77–0.82; PA: Cohen's κ = 0.69, 95% CI, 0.67–0.72; weight: Cohen's κ = 0.67, 95% CI, 0.64–0.71).
Patient and physician responses to the questionnaires administered after the visits were cross-tabulated with audio recordings to assess the accuracy of their self-report of any weight-related discussions. Patients or physicians were deemed “accurate” if the audio recording confirmed their response on the questionnaire after the visit that they did or did not discuss one or more topics related to diet, PA, or BMI/weight. Physicians and patients were deemed “congruent” if they were both accurate and their reports matched the audio recording.
PROC GENMOD was used to fit 2 generalized linear mixed models with a logit link to account for clustering of patients within physician to examine the likelihood of patients (model 1) and physicians (model 2) being inaccurate when weight was not discussed, using covariates described in the baseline questionnaire. We identified the following theoretically relevant covariates a priori to include in the analyses. For model 1, covariates included patient sociodemographic factors (age, sex, education) and physician race; visit factors included length of conversation and patient's motivation to lose weight (very motivated vs somewhat to not at all motivated). Motivation to lose weight was measured using a 7-point Likert scale (1 = not at all, 7 = very much). For model 2, covariates included physician sex and physician race as well as patient BMI (overweight vs obese); visit factors included length of conversation and physician level of comfort discussing weight (very comfortable vs mostly to not at all comfortable). Physician comfort discussing weight was measured using a 5-point Likert scale (1 = not at all comfortable, 5 = very comfortable). Few patients and physicians rated themselves as Asian; thus for race concordance dyads of whites and Asians/Pacific Islanders were categorized as white. Model building started with testing the association of all covariates. To be conservative, only those covariates significant at P ≤ .50 were retained for modeling. However, the small sample size for the “no weight discussed” group (n = 141) limited the number of covariates that could be included in the model. All analyses were performed using SAS software version 9.2 (SAS Institute, Inc., Cary, NC). Significance for models was set at P < .05.
Results
Participant and Visit Characteristics
Table 1 contains relevant sociodemographic variables, race concordance, and visit characteristics. Forty physicians (mean age, 47.3 ± 7.2 years) and 461 patients (mean age, 58.9 ± 3.9 years) participated in the study. Of the 461 patients, 90% had at least one or more of the following weight-related chronic diseases: diabetes, hypertension, hyperlipidemia, and arthritis.
Accuracy and Congruency
Table 2 describes the accuracy and congruence of patients and physicians. According to the objective coding, weight was discussed in 69% of the encounters (n = 320). Weight discussions were cross-checked against audio recordings for 461 dyads (patients and their physician) and stratified into “weight discussed” (n = 320) and “weight not discussed” (n = 141). When surveyed immediately after the encounter, physicians reported discussing the following topics: weight (48%), nutrition (52%), PA (62%), smoking (34%), and alcohol use (20%).
Overall, accuracy (self-report confirmed by audio recording) was 70% for physicians and 67% for patients; congruence (patient and physician agreement confirmed by audio recording) was moderate (62%). In encounters coded as containing weight-related content (n = 320), overall accuracy was almost perfect: 97% among physicians and 98% among patients. In terms of physician accuracy, 31 physicians (78%) were 100% accurate for all their patients (n = 247, or 77% of total patients). In terms of patient accuracy, all the patients of 36 physicians (n = 290, or 91% of total patients) were 100% accurate. For discussions that included weight, overall congruence between patients and physicians was 95%: 179 encounters (56%) were 100% congruent if 1 (7 of 320), 2 (21 of 320), or all 3 topics (151 of 320) were discussed.
When weight was not discussed (n = 141), overall accuracy was much lower for physicians (44%) and patients (36%). In terms of physician accuracy, 10 physicians (25%) were 100% inaccurate for all their patient encounters (n = 26, or 18% of total patients), whereas 9 physicians (23%) were 100% accurate for all their patient encounters (n = 25, or 18% of total patients). The remaining 21 physicians (58%) were accurate for 37 patients (26%) and inaccurate for 53 patients (38%). In terms of patient accuracy, all the patients of 9 physicians (n = 21, or 14.9% of total patients) were 100% inaccurate. For the remaining 120 patients, 42 (29.8%) were accurate and 78 (55.3%) were inaccurate across 31 physicians.
Overall, congruence was also low (28%) when weight was not discussed. In particular, 13 physicians (33%) had encounters with 33 patients (23%) in which both the patient and physician were inaccurate (0% congruence); 27 physicians (67%) had encounters with 37 patients (26%) in which both the patient and physician were accurate (100% congruence). In the remaining 71 patient encounters (51%) either the patient or physician was inaccurate (0% congruence).
Models
Given the lack of variability in encounters coded as containing weight-related content, we did not model for the predictors of accuracy for these encounters. In encounters where weight was not discussed, no significant factors predicted patient accuracy (Table 3). However, in the physician model, physicians who were less comfortable discussing weight were more likely to report that weight was discussed when the audio recording indicated that weight was not discussed (odds ratio, 4.5; 95% CI, 1.88–10.75) (Table 4). Race concordance of the dyad was also a significant predictor. White physicians with African American patients were more likely to report accurately that weight was not discussed than white physicians with white patients (odds ratio, 0.30; 95% CI, 0.13–0.69).
Discussion
There were 3 key findings in this study. First, physician and patient self-reports of weight-related discussions were highly accurate and congruent when weight discussions occurred. Second, when weight was not discussed, physicians and patients were much less accurate and congruent. Finally, physicians who were less comfortable discussing weight and dyads in which both physician and patient were white/Asian were more likely to report that a weight discussion had occurred when it did not.
That patients and physicians are highly accurate and congruent when weight is discussed suggests that there is value in assessing patient and physician self-reports of weight discussions (ie, diet, PA, weight). It seems that when physicians talk about weight, patients recall that weight was discussed. The findings of this study should be encouraging for physicians who discuss weight-related matters with their patients given that patients recalled that weight-related topics were discussed and many accurately recalled the specific components of those discussions (ie, PA, nutrition). Weight-related messages, when delivered, seem to be received.
However, there is a difference between reporting that a message is received and whether that message is understood. This is a complex issue. In our study it is possible that both patients and physicians accurately reported that a weight-related topic was discussed during the clinical visit, but what the patient heard was not what the physician thought they discussed. Implications of these results might be that to ensure that messages that are given are received; physicians who discuss weight with their patients might summarize the discussion and allow patients to make any corrections.
Future studies using audio recordings to assess physician-patient communication can include qualitative measures after the visit to help clarify what health messages physicians think they impart and what health messages patients believe they receive.
Physicians and patients were less accurate in their recall of weight-related discussions when weight was not discussed (ie, reported a weight discussion when none occurred). Our results differ from those of earlier studies that showed that physicians and patients tend to underreport health promotion discussions.19 In contrast, we found that when audio recordings indicated that weight was not discussed, many physicians and patients overestimated the occurrence of weight-related discussions. This finding is perplexing. It is possible that on some rare occasions, physicians and patients recalled weight-related conversations that did not have a direct weight-related purpose. One example could be when physicians and patients were discussing adding more fiber to help with constipation. Even though adding fiber might help with weight loss, coders would not have counted this as nutrition that was weight related, but patients and physicians might have counted this as discussing nutrition. There is error in every measurement tool. We cannot tease apart patients' and physicians' interpretations of what was weight related. It also is possible, but unlikely, that physicians and patients did not answer the questions carefully and agreed that all topics were discussed, or that physicians who, for the most part, were completing the questionnaires immediately after the encounter may have been rushed. However, the data do not confirm this: physicians reported discussing alcohol use and smoking to a much lesser extent than weight, nutrition, or PA. Also, neither patients nor physicians knew the study was about weight; only 2% of patients (7 of 461) and 3% of physicians (1 of 40) guessed the study hypothesis involved examining weight-related discussions. Regardless of the reason behind the high recall of weight-related discussions, many physicians and patients reported weight-related discussions when they did and did not occur.
Finally, there were no significant factors that predicted patient inaccuracy when weight was not discussed. This is inconsistent with previous reports indicating that demographic and psychosocial factors are related to patient recall.21,22 Two factors predicted whether physicians overreported. First, physicians who were uncomfortable discussing weight may have avoided talking about weight yet reported they did because they know or believe it is part of their clinical responsibility and they desire to appear more conscientious.19 Second, race concordance was also a significant predictor. White physicians with African American patients were more likely to report accurately that weight was not discussed than white physicians with white patients. Previous work indicates that clinical visits that are race concordant are longer and patients tend to be more participatory (ie, they ask more questions).23 However, some reports suggest that race concordance does not seem to be positively associated with the prevalence of weight-related discussions.24
Only 6 African American physicians were in this sample, making it difficult to assess effects for the African American physician-patient dyad. However, in the white-white dyads, patients might have been acting in a more participatory manner, and this influenced physicians to recall weight discussions even when coders did not observe weight-related content. Because we grouped whites with Asians/Pacific Islanders, it is possible that cultural differences and communication (ie, limited English language proficiency) may explain in part why white physician–white patient dyads were more likely to report the occurrence of a weight discussion when none took place. However, this is unlikely given the small numbers of Asians/Pacific Islanders in the study.
There were limitations to this study. First, this study is limited by potential bias in reporting weight discussions. Patients and physicians were aware that the study was about preventive health, which may have influenced them to report that weight was discussed when it was not.7 Furthermore, we grouped Asian/Pacific Islanders with whites for race concordance analyses, potentially affecting model significance. Also, little information was collected on the physician-patient relationship (only 2% of patients were “new patients”), in particular the length of that relationship (which could influence trust), or preferences for communication strategies/style, both of which may have the potential to influence the interpretation of communication.
Conclusion
When weight is discussed by physicians, patients are cognizant of those discussions, including details of the message (ie, weight, nutrition, and PA). Physicians who discuss weight with their patients can follow up to ensure that the health messages delivered are received and understood by patients. Discussions about weight can act as a “priming effect” for behavior change in patients; physician advice along with follow-up or referral can positively affect a patient's attempt to lose weight.25,26 The overestimation of weight discussions by some physicians (particularly those who are less comfortable discussing weight) constitutes a missed opportunity for a health intervention. Discomfort with discussing weight is one of several systemic barriers reported by physicians and highlights the need for physician training for weight management counseling.27 Future studies also are needed to further explore race concordance as a variable in physician communication with patients who are overweight/obese.
Notes
This article was externally peer reviewed.
Funding: This work was supported by grants R01CA114392 and R01HL092403 from the National Institutes of Health.
Conflict of interest: none declared.
- Received for publication March 30, 2013.
- Revision received June 28, 2013.
- Accepted for publication July 22, 2013.




{kind=link}