
Abstract
Purpose: To determine public perceptions of the effect of direct-to-consumer advertising (DTCA) of prescription medications on health behaviors, health care utilization, the doctor-patient relationship, and the association between socioeconomic status and these effects.
Methods: Cross-sectional survey of randomly selected, nationally representative sample of the US public using computer-assisted telephone interviewing. Main outcome measures: numbers and proportions of respondents in the past 12 months who, as a result of DTCA, requested preventive care or scheduled a physician visit; were diagnosed with condition mentioned in advertisement; disclosed health concerns to a doctor; felt enhanced confidence or sense of control; perceived an effect on the doctor-patient relationship; requested a test, medication change, or specialist referral; or manifested serious dissatisfaction after a visit to a doctor.
Results: As a result of DTCA, 14% of respondents disclosed health concerns to a physician, 6% requested preventive care, 5% felt more in control during a physician visit; 5% made requests for a test, medication change, or specialist referral, and 3% received the requested intervention. One percent of patients reported negative outcomes, including worsened treatment, serious dissatisfaction with the visit, or that the physician acted challenged. Effects of DTCA were greater for respondents with low socioeconomic status.
Conclusions: DTCA has positive and negative effects on health behaviors, health service utilization, and the doctor-patient relationship that are greatest on people of low socioeconomic status. The benefits of DTCA in terms of encouraging hard-to-reach sections of the population to seek preventive care must be balanced against increased health care costs caused by clinically inappropriate requests generated by DTCA.
Direct-to-consumer advertising (DTCA) of prescription medications may have beneficial or harmful effects on patients, their relationship with physicians, and the health care system.1–9 So far, there are few empirical data on the actual effects of DTCA, and available data are limited by small samples,10 selected populations,11 hypothetical scenarios,12 or have been criticized on methodological grounds.13,14
In an article published in the last issue of the Journal of the American Board of Family Practice, we examined the effects of DTCA on quality of care, health service utilization, and physician perceptions of its impact on the doctor-patient relationship.15 In this article, we use the data from a large telephone survey of a nationally representative sample of the American public to test hypotheses concerning the effects of DTCA on health behaviors, patients’ perceptions of its impact on the doctor-patient relationship and on the health care system, and the extent to which these effects are mediated by socioeconomic status.
Methods
Development of Testable Hypotheses
We undertook a literature review to identify published claims about the effects of DTCA and formulate testable hypotheses.15
Sample
The survey was conducted between March 2000 and March 2001 on a household probability sample from the 48 contiguous states by using random-digit dialing to select households and a random selection method to select one respondent aged 18 or over for interview in each sample household. Verbal informed consent was obtained from all respondents before they began the interview. Eligibility was limited to English and Spanish speakers without cognitive or physical impairments that prevented completion of the interview. A small financial incentive was offered for completion of the interview. At least 15 attempts were made to call nonresponders, and where telephone numbers of nonrespondents could be matched with an address, up to 2 letters were sent to encourage response. The average administration time was 20 minutes. All interviews were conducted by trained interviewers using computer-assisted telephone interviewing (CATI).
An oversample of persons in poor health was achieved by screening a random subsample of households and including only those respondents who described their health as fair or poor (rather than excellent, very good, or good); had a disability or handicap that prevented them from participating fully in school, work, housework, or other activities; or had been hospitalized within the past 12 months, for reasons other than a normal delivery of a child. A total of 2720 interviews were completed in the nonoversample portion of the study, representing a completion rate of 72% and a response rate of 54%, and 489 interviews were completed in the oversample (completion rate, 95%; response rate, 51%).
Data were weighted to adjust for unequal probability of selection (including the oversample of persons in poor health). To adjust for survey nonresponse, stratification weights were developed using the March 2000 Current Population Survey from the US Census Bureau as standard. The poststratification weights were based on gender within age within race, as well as education, health insurance status (insured versus uninsured), and household size.
Interview and Data Collection
The interview was developed after literature review and focus group participation and piloted to ensure all questions were easily understood and contained no ambiguities. In the preamble, it was described as a survey on health issues, in particular how Americans make decisions about health care and their feelings about the health care available to them. No mention of DTCA was made in characterizing the survey. Initial questions inquired into respondents’ use of different sources of health information, approaches to health information, and relationships with their physicians. Respondents were then asked about their experience of searching the Internet for health information, because this was the primary focus of the project. Once questions about the Internet were completed, respondents were asked for their experiences of DTCA, whether they had encountered an advertisement that was personally relevant, and their response to that advertisement. Respondents who had sequentially seen an advertisement for a prescription medication in the past 12 months, perceived it as personally relevant, and discussed the information in this advertisement with their physician were asked about the last time they had done this. To avoid overloading respondents, those who had already answered questions about taking health information from the Internet to a visit with their doctor (n = 82) were not asked about the last occasion on which they had discussed information in an advertisement with their doctor.
Demographic and socioeconomic data, including age, self-defined ethnic origin, educational achievement, household income per annum, health insurance status, and current health status were collected from all respondents. Respondents were defined as being proactive about health care information if they stated that they went out of their way to look for information on health topics of personal relevance, rather than simply reading it if they came across it or not reading any such information.
Analysis
Dependent variables organized by hypothesis are summarized in Table 1. These variables include the kinds of requests made to physicians based on DTCA, the responses received to such requests, characteristics of the doctor-patient exchange over such requests, and the outcomes from the exchange. In addition, we included the doctor’s acting challenged as an important outcome variable, because it had been established as such in our previous work.16 We postulated that the doctor’s acting challenged could indicate either that the doctor felt challenged by interacting with an activated, knowledgeable patient or that the patient was failing to acknowledge the doctor’s professional expertise. Independent variables were categorized to maximize opportunities to determine the effect of low SES.
Summary of Hypotheses Tested, Dependent Variables Used to Test Each Hypothesis, Total Number of Respondents Experiencing Each Outcome, and Association with Socioeconomic Status
Univariate relationships between independent variables and the dependent variables were calculated using the χ2 statistic or Fisher exact test as appropriate. Multivariate relationships were analyzed using the same methods of stepwise multiple logistic regression and adjustment for weighting described in the previous article.15
Results
Characteristics of Respondents (n = 3209)
The characteristics of the respondents before and after weighting are presented in Table 2, which allows for an assessment of the demographic representativeness of our sample. The small differences between unweighted and weighted data suggest that the random-digit dialing method succeeded in generating a sample similar in profile to that of the US population.
Demographic and Health Characteristics of Respondents
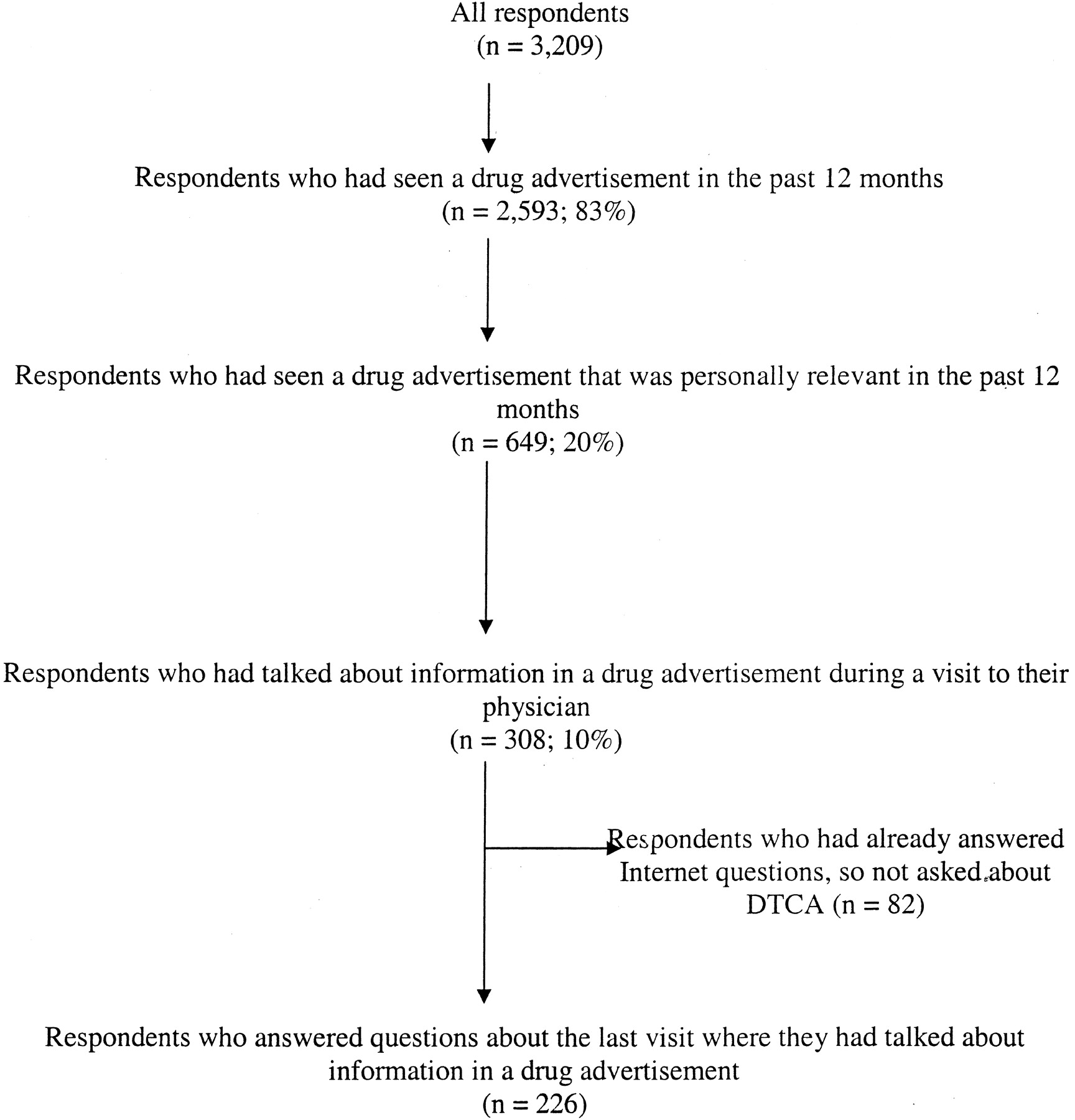
Among the 308 respondents who had discussed information from DTCA with their physician, 82 were not asked about this because they had already responded to questions about taking information from the Internet to a visit (Figure 1). The 226 who did provide information were more likely to be unemployed (33% vs 20%, P = .036); less likely to be in good health (24% vs 43%, P = .011); and more likely to have a regular doctor (95% vs 82%, P = .008) than the 82 who did not provide information.

Flow chart of respondents.
Overall Perceptions of DTCA
Most respondents were fairly positive about the recent increase in drug advertisements; 7% [95% confidence interval (CI) 6 to 8%] thought it was a very good thing and 40% (95% CI, 38 to 43%) thought it was a good thing. Thirty-four percent (95% CI, 31 to 36%) were neutral, and only 19% (95% CI, 18 to 21%) thought it was either very bad or bad. There was no association between socioeconomic status and overall opinion about DTCA. Table 3 presents the proportions of respondents who had seen a DTCA in the preceding 12 months who agreed with various statements about potential benefits and harms of DTCA.
Respondents’ Views about Effects of DTCA (n = 2593)
Response to DTCA
Eighty-three percent (95% CI, 81 to 85%) of all respondents had seen an advertisement for a prescription medication in the preceding 12 months. The most common source of DTCA was television (94%), followed by newspapers or journals (62%) and the radio (22%). In the preceding 12 months, 20% (95% CI, 19 to 22%; n = 649) of respondents had seen a drug advertisement relevant to their health, and 10% (95% CI, 8 to 11%; n = 308) had discussed information in a drug advertisement with their doctors (Figure 1). Seventy-seven percent (n = 171) of these conversations were with a primary care physician.
Effects of DTCA
Table 1 summarizes our research questions, outcome variables, the number of respondents who stated they had experienced each outcome, and the significant associations with each outcome. Both in Table 1 and the text, the main outcomes are grouped into clinical benefits and harms, psychosocial benefits, effect on the doctor-patient relationship, and effect on health service utilization.
Clinical Benefits and Harms of DTCA
Requested Preventive Care
Of the 3209 respondents, 203 had requested preventive care, such as a screening or blood test. Socioeconomic status was strongly associated with this outcome; people who had not completed high school, Hispanics, and people with chronic disease were all more likely to seek preventive care as a result of information in a drug advertisement (Table 4).
Factors Associated with Seeking Preventive Care Because of Information in a Drug Advertisement
Scheduled Checkup
Of the 3209 respondents, 189 had visited a health professional for a check-up as a result of information in a DTCA. The relationship between this outcome and socioeconomic status was very similar to that for requesting preventive care (data not shown).
Diagnosed with Condition Mentioned in Advertisement
Of the 226 people who discussed information from a drug advertisement with a doctor, 28 were told they either had, or were at risk for, the condition mentioned in the advertisement during or immediately after the visit during which DTCA was discussed. This outcome was not associated with socioeconomic status but was associated with being in managed care (2% in managed care vs 0% not in managed care; P = .012). A further 149 respondents had previously been diagnosed with the condition mentioned in the advertisement.
Improved Treatment
Of 226 respondents, 67 were given the medication mentioned in the drug advertisement and told by their doctors that it would improve their health. This outcome was more prevalent in people with low incomes (61% annual income <$15,000 vs 35% ≥$15,000, P = .032); low educational status (61% not completed high school vs 34% for high school graduate or higher, P = .021); and people who were not proactive about health information (45% not proactive vs 25% proactive, P = .006).
Worsened Treatment
Twenty-six people reported requesting and receiving an advertised medication that their doctor said would not help them. This was more likely to occur for persons aged 18 to 24 than for those over 25 (75% vs 9%, P < .001).
Psychosocial Benefits of DTCA
Enhanced Sense of Control during Visit
Of 226 people, 168 said that they had felt more in control during a visit to a doctor as a result of information in a DTCA. Women were more likely than men to experience this enhanced sense of control (85% vs 68%, P = .003), as were people who were not proactive about health information compared with those who were (83% vs 72%, P = .041).
Enhanced Sense of Confidence during Visit
Of 226 people, 142 said they had felt more confident during the visit as a result of information in a drug advertisement. This was not related to respondents’ socioeconomic status.
Effects of DTCA on Doctor-Patient Relationship
Disclosed Health Concerns to Doctor
Of 3209 people, 455 stated they had talked about concerns about their own health to a doctor as a result of information in a DTCA. This outcome was associated with low socioeconomic status (Table 5).
Factors Associated with Disclosing Health Concerns to a Doctor Because of DTCA
Changed Global Rating of Doctor-Patient Relationship
Of the 226 people who provided information about discussing DTCA during a visit, 51 thought the relationship had improved as a result, 163 thought there had been no change, and 11 thought it had worsened. This outcome was strongly related to socioeconomic status. Respondents who made a request but did not get what they asked for were more likely to report a worsened doctor-patient relationship (Table 6).
Factors Associated with Changes in the Doctor-Patient Relationship
Doctor Acted Challenged
Of the 226 people, 30 reported that their doctors had acted as if they felt their authority was being challenged by the patient’s discussing information from a drug advertisement during a visit. Respondents were more likely to perceive their doctor as acting challenged if they were of low educational status (33% not completed high school vs 12% graduated from high school, P = .010) and if they were proactive about health information (18% proactive vs 9% not proactive, P = .046).
Patient Manifested Serious Dissatisfaction after Discussing DTCA during a Visit
Of 226 people, 46 sought a second opinion (n = 29), changed their doctor (n = 19), or changed their health care plans (n = 11) as a result of dissatisfaction with a discussion with their doctor about DTCA during a visit. This was more prevalent in people of low socioeconomic status but was not related to getting or not getting a specific intervention requested (Table 7).
Factors Associated with Manifestations of Serious Dissatisfaction (ie, Seeking Second Opinion, Changing Doctor, or Changing Health Plan)
Effects of DTCA on Health Care System
Scheduled a Visit to a Physician to Discuss Information in DTCA
Most respondents waited to discuss information until they had some other reason for visiting their doctors; however, 55 of 226 respondents scheduled a visit to a physician specifically (n = 27) or partly (n = 28) to discuss information from an advertisement. This outcome was related to socioeconomic status, with people of low education (58% not completed high school vs 22% completed high school, P = .009) and people in managed care (27% in managed care vs 13% not in managed care, P = .021) more likely to do so.
Requests Made and Filled
One hundred and sixty-one people requested at least one intervention from their doctors as a result of DTCA. Most requests were for changes in medication (n = 131), followed by tests (n = 69) and referrals to a specialist (n = 50). Of these people, 89 received the specific intervention requested. Receiving the specific intervention requested was associated with higher socioeconomic status. Respondents were more likely to get what they asked for if they were white (whites 63% vs nonwhites 30%, P = .001) or had completed high school (58% completed high school vs 29% not completed, P = .033). There was no association with being in managed care and having requests filled.
Discussion
Implications
We found significant positive and negative effects of DTCA on health behaviors, health service utilization, and the doctor-patient relationship. The impact was greatest on people of low socioeconomic status. This information is important to those seeking to maximize the benefits and minimize the harms of DTCA.
DTCA encourages members of the public, particularly those of low socioeconomic status, who are traditionally considered hard to reach with public health campaigns,11,12 to request preventive care and schedule a checkup. It encourages people to disclose health concerns to their doctor, and enhances some patients’ sense of confidence and control during a visit. From a policy or population health perspective, these undoubted benefits have to be weighed against the well-documented effect of DTCA on increasing health costs. In our previous article, we demonstrated that physicians experience DTCA as having an adverse effect on time efficiency and resulting in numerous, clinically inappropriate requests for tests, specialist referrals, and changes in medication. About half such requests are acquiesced to, with negative consequences on health care expenditure without commensurate health benefits. When considering the overall benefits and harms of DTCA, could the $2.5 billion spent on DTCA last year have achieved equivalent health benefits if the techniques of advertising were focused on interventions that are known to improve health outcomes?
Although only 5% of respondents who brought DTCA information to their doctors reported a negative impact on the doctor-patient relationship, 13% perceived that their doctor felt his/her authority had been challenged, and 21% reported sufficient dissatisfaction that they sought a second opinion, a change in doctor, or a change in health care plan. These data could represent the positive outcome of an informed health consumer or the negative outcome of information provided by a biased third party that undermines the consumer’s confidence in the health system. More research is needed to answer this question.
Methodological Issues
Several methodological issues limit the generalizability of our findings. First, this article reports on a secondary analysis of an extant data set, so not all hypotheses could be evaluated with the desired precision. In addition, lack of information from respondents’ physicians and/or medical records precludes direct verification of respondents’ perceptions. For example, we cannot determine whether requests made and filled were clinically indicated. Finally, respondents who discussed health information from the Internet with their physicians were not asked about the last time they took information from DTCA to a physician visit; hence, generalizability is restricted to the population that does not take information from the Internet to their doctor. However, these data are important because the 226 respondents who provided information about taking DTCA to a physician visit were of lower socioeconomic status than the 82 who did not. Other data from responses by all 3209 respondents indicate that DTCA has greatest effect on people of low socioeconomic status. To accommodate for this limitation, we conservatively assumed that the subsample that was not asked about discussing DTCA during a physician visit experienced no effects (ie, would not have sought an appointment or made a request). Thus, all our estimates of the population effects of DTCA are minimum estimates.
Conclusions
DTCA has positive and negative effects on health behaviors, health service utilization, and the doctor-patient relationship that are greatest on people of low socioeconomic status. The benefits of DTCA in terms of encouraging hard-to-reach sections of the population to attend for preventive care must be balanced against the increased costs to the health service from clinically inappropriate requests generated by DTCA.
Acknowledgments
We are grateful to the Robert Wood Johnson Foundation for funding this research, Kinga Zapert and Rachel Turner of Harris Interactive, Inc., for developing and fielding the survey instrument and to Joseph Catania, PhD, director of the Health Survey Research Unit, for advice on the analytical strategy. Elizabeth Murray was a 2001–02 Harkness Fellow in Health Care Policy, supported by the Commonwealth Fund.
Notes
This project was funded by the Robert Wood Johnson Foundation. EM was a Harkness Fellow in Health Care Policy 2001–02, supported by the Commonwealth Fund, based in the Program for Medical Ethics at UCSF.
- Received for publication March 24, 2003.
- Revision received March 24, 2003.
References




{kind=link}
Jump to section
Related Articles
Cited By...
- US FDA breakthrough therapy designation and consumer drug advertising: a recipe for confusion
- Direct-to-Consumer Prescription Drug Advertising and Patient-Provider Interactions
- Direct-to-Consumer Advertising in Oncology.
- Symposium: Introducing Technology into Orthopaedic Practice: How Should It Be Done?