
Abstract
Background:The objective of the study was to determine physicians’ views of the effects of Direct-to-Consumer Advertising (DTCA) on health service utilization, quality of care, and the doctor-patient relationship.
Methods:Cross-sectional survey of a nationally representative sample of US physicians to determine their perceptions of the effects of patients discussing information from DTCA on time efficiency; requests for specific interventions; health outcomes; and the doctor-patient relationship.
Results:Physicians reported that more than half (56%) of patients who discussed information from DTCA in a visit did so because they wanted a specific intervention, such as a test, change in medication, or specialist referral. The physician deemed 49% of these requests clinically inappropriate. Physicians filled 69% of requests they deemed clinically inappropriate; 39% of physicians perceived DTCA as damaging to the time efficiency of the visit, and 13% saw it as helpful. Thirty-three percent of physicians thought discussing DTCA had improved the doctor-patient relationship; 8% felt it had worsened it. The effect on the relationship was strongly associated with doing what the patient wanted.
Conclusions:DTCA can have good and bad effects on quality of care, the doctor-patient relationship, and health service utilization. The benefits might be maximized, and the harms minimized, by increasing the accuracy of information in advertisements; enhancing physicians’ communication and negotiation skills; and encouraging patients to respect physicians’ clinical expertise.
Compared with other sources of health information for the public, direct-to-consumer advertising of prescription medications (DTCA) is pervasive, persuasive, and passive. Patients are exposed to DTCA without actively seeking it. Unlike much public interest advertising,1 it uses effective techniques, including a strong emotional appeal to targeted audiences.2 The pharmaceutical industry spends more than $2 billion annually with the goal of promoting consumer desire for products and hence increasing market share.3
Its advantages and disadvantages are controversial.3,4 Proponents contend that DTCA provides valuable health information5 that helps patients voice health concerns to their physician and increases patients’ sense of confidence and control during visits.6 Both these effects could improve the doctor-patient relationship. DTCA may also raise awareness of underdiagnosed, treatable conditions such as hyperlipidemia or depression, leading to physician visits for prevention and treatment that would not otherwise occur.7 Opponents argue that DTCA contributes to rising drug costs,8 encourages inappropriate prescribing,9–11 and may increase overall health care costs needlessly by leading to requests for tests or referrals that are not clinically indicated. Evidence for these conflicting claims is scanty. Available data are limited by small samples or restricted populations.9,12 This is the first population based survey of physicians, and the first to look at physician views on the impact of DTCA on the doctor-patient relationship and the quality of care. Moreover, it is unknown whether the effects of DTCA vary according to socioeconomic or health status, which is important in view of the widespread concern about health disparities.
We used data from 2 nationally representative surveys of US physicians and the US public on DTCA to examine these claims, and to determine the extent to which the effects of DTCA vary with socio-economic and health status. This article uses data from the physician survey to address the effects of DTCA on quality of care, health outcomes, health service utilization, and physicians’ perceptions of its effect on the doctor-patient relationship. Our forthcoming article uses the public data set to analyze issues pertaining to the individual and to population health.
Methods
Development of Testable Hypotheses
Our first step was to collate published claims and derive hypotheses that could be tested in at least 1 of our 2 data sets (Figure 1). Not all the claimed benefits or harms of DTCA were amenable to examination with the available data (e.g., “DTCA contributes to a cultural expectation of a ‘pill for every ill.’”13,14

Summary of testable hypothesis on the effects of DTCA.
Sample
Two thousand physicians were randomly selected from the national list of physicians provided by the Medical Marketing Service, Inc. (MMS). The MMS list is based on the national database of the American Medical Association (AMA), which contains more than 650,000 physicians, and is the most complete list of physicians available in the US. Physicians who currently spent more than 20 hours a week on direct patient care were included in the survey. The sample was stratified by specialty: primary care, medical specialty, or surgical specialty. Primary care included Family Practice, General Practice, Internal Medicine, and Pediatrics. Ob-Gyn was classified as a surgical specialty.
Questionnaire
The questionnaire was developed after literature review and focus group discussions and was pretested. It consisted of 3 sections of closed-ended questions and took approximately 12 minutes to complete. The entire sample received Part 1 of the questionnaire, which elicited general information about views on health information on the Internet and DTCA. Questions examined general views on accuracy and effects of such information, and personal use of the Internet at work. Part 2 was sent to a random 50% of the sample. It asked whether any patient had discussed information derived from DTCA in the past 12 months and, if so, specific inquiries were made about the last time this happened. “Last time” methodology was used to minimize recall bias. Areas explored were the relevance and accuracy of the information, physicians’ perceptions of why the patient had brought the information, physicians’ responses to the patient, and their views about the impact on health care, health outcomes, and the doctor-patient relationship. The other 50% of the sample received a different Part 2, which asked about respondents’ experiences with Internet information. Part 3 was received by the entire sample and obtained demographic and workload information: hours per week spent on face-to-face consultations, other tasks related to patient care, and administrative tasks; numbers of patients seen per week; practice income; proportions of patients on Medicaid, from minority groups, having household incomes of less than $20,000 per annum, and with no health insurance; geographic setting of practice; age and racial origin of respondent. This was supplemented with information from the MMS database, including specialty, year of graduation from medical school, geographic region (East, South, Midwest, West), whether hospital or office-based, and whether trained in the United States or overseas.
Response Rate
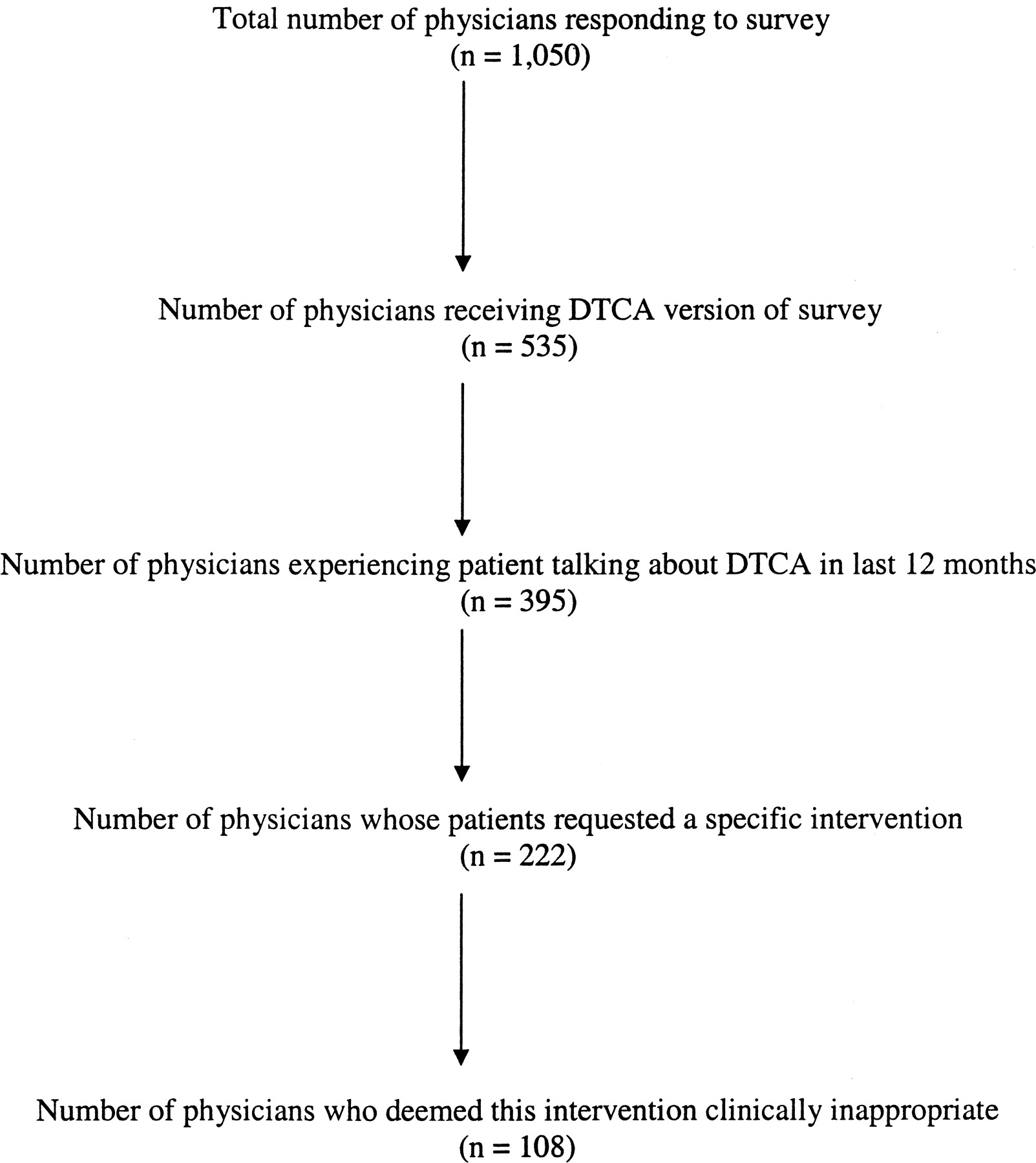
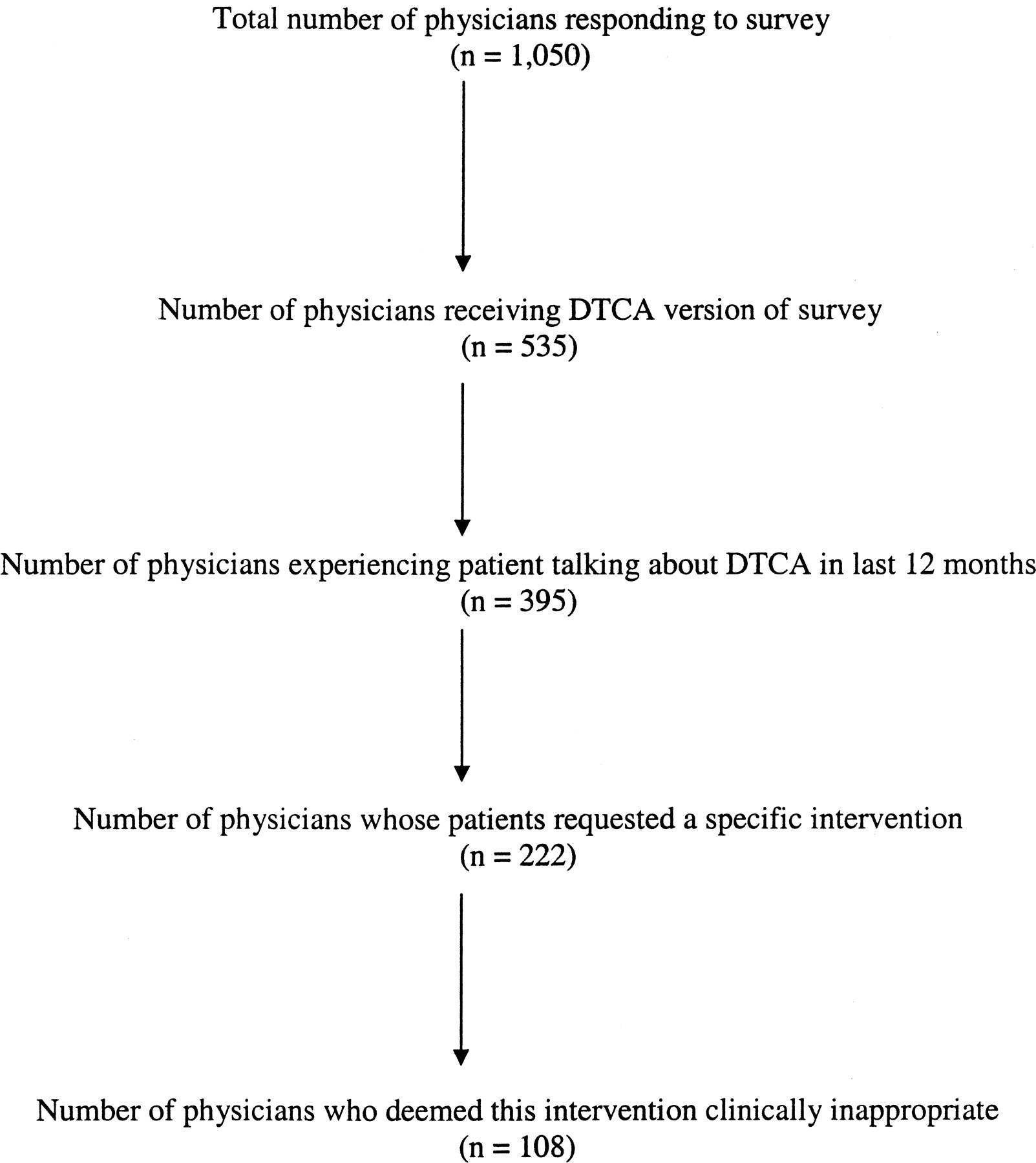
Data collection was undertaken between November 2000 and February 2001. The questionnaire was mailed to the selected physicians with a check for $35 as a token of appreciation for completing the questionnaire. Up to 3 reminders were sent and additional telephone contact made with nonresponders. Of the original 2000 physicians sent the survey, 38 were ineligible because they were deceased, retired, or no longer in practice; 1050 physicians completed the questionnaire (response rate 53%). Of these, 535 received the DTCA version of the questionnaire and 515 the Internet version (Figure 2).
Analysis
Weighting
Data were weighted to represent the national population of physicians on the MMS database who spend 20 or more hours per week on direct patient care using the MMS variables mentioned above.
Outcome Variables
The effect of DTCA on the doctor-patient relationship was tested using physician perceptions of the relationship and whether the doctor had felt that the patient was challenging his or her authority during the discussion. Outcomes pertaining to the effect of DTCA on health service utilization were: physicians’ perceptions of the effect of DTCA on the time efficiency of the visit; the proportion of patients who made requests for specific interventions as a result of DTCA; the proportion of these requests that the doctor deemed clinically inappropriate; the proportion of appropriate and inappropriate requests filled by the physician; and physicians’ perceptions of the effects of DTCA on quality of care and ultimate health outcomes.
Independent Variables
We used 4 categories of independent variables: practice demographics (as a proxy for patient socioeconomic status); pre-existing physician views about DTCA; physician’s emotional and cognitive responses to the last time a patient brought information from a DTCA to a visit (whether they perceived the patient as taking responsibility for his/her health or challenging the doctor’s professional authority, why the patient discussed the information with them, whether any requests made by the patient were clinically appropriate, whether the request(s) was filled, whether there was enough time to discuss the information, and whether they knew the patient well enough to have good communication); and physicians’ perceptions of the accuracy and relevance of the information in the advertisement discussed.
Univariate relationships were calculated using the χ2 statistic or Fischer exact test as appropriate. In the absence of a priori hypotheses, multivariate relationships were determined by entering correlates with univariate relationships (P < .20) into a stepwise multiple logistic regression to identify the “most important” correlates, where importance is defined solely by statistical criteria. Each analysis went through several iterations, with each new iteration using successively more stringent statistical criteria for inclusion in the model. Each iteration included consideration of a model yielded by a forward stepwise procedure and a model yielded by a backward stepwise procedure. The goal was to identify the most parsimonious model while still achieving adequate fit, which was operationalized as P > .20 on the Hosmer-Lemeshow goodness-of-fit test.
Because all data were weighted (except where specified), the appropriate procedures to correct p-values and standard errors were undertaken. We used the SVYTAB procedure in STATA to obtain the Rao and Scott F test p-values15 and the SVYLOGIT procedure in STATA to obtain corrected standard errors for parameter estimates.
Results
Characteristics and Representativeness of the Sample
The characteristics of the respondents before and after weighting are presented in Table 1. Weighting made only minimal difference, confirming that respondents were representative of the national population of physicians. From this point on, all data presented are weighted.
Demographic, Workload, and Practice Characteristics of Respondents (n = 1050)
General Views of DTCA
Positive and Negative Effects of DTCA
Of all respondents (n = 1050), more than half had a negative response to the recent increase in advertising prescription drugs directly to consumers: 52% [95% confidence interval (CI), 49 to 55%] thought it was bad or very bad, 17% (95% CI, 15 to 19%) were neutral, and only 31% (95% CI, 28 to 34%) thought it was good or very good. Despite this, most doctors agreed that DTCA gives patients confidence to talk to their doctors about health concerns and encourages patients to follow the doctor’s instructions or advice (Table 2). No demographic, practice, or workload variables were associated with respondents overall opinion about DTCA.
Physicians’ Views on the Effects of DTCA (n = 1050)
Accuracy and Relevance of DTCA
Eight percent (95% CI, 7 to 10%) of respondents thought that advertisements were very accurate, 67% (95% CI, 64 to 69%) thought they were somewhat accurate, and the remainder thought they were not very or not at all accurate. Most physicians thought that their patients were not good at assessing whether the information in a drug advertisement was personally relevant: only 4% (95% CI, 3 to 6%) thought their patients were excellent or very good at this, 18% (95% CI, 15 to 21%) thought they were good at it, 54% (95% CI, 51 to 58%) thought their patients were fair, and 24% (95% CI, 21 to 27%) thought they were poor at this.
Experience with Patients Bringing Information from DTCA to a Physician Visit
Respondents were asked about the last time a patient talked about information from a drug advertisement during a visit. 80% (n = 395; Figure 2) had experienced this in the previous 12 months. Data in the remainder of this article refers to those 395 physicians. Of these, 51% reported that less than 20% of their patients had talked about information from a drug ad during a visit, and a further 35% stated that between 21 and 40% of their patients had done this.
Effect on Doctor-Patient Relationship
General Impact
More physicians believed that patients talking about information from a drug advertisement had a positive effect (33%; 95% CI, 28 to 38%) than a negative effect (7%; 95% CI, 5 to 11%) on the doctor-patient relationship. On univariate analysis, an improved relationship was associated with physicians’ perceptions that the information in the advertisement was relevant and accurate, the patient seeking only the doctor’s opinion rather than a specific intervention, and the doctor’s responses during the discussion (Table 3). Specifically, the doctor doing what the patient wanted, feeling that the patient was taking responsibility for his or her health, and perceiving the request as clinically indicated were all associated with an improved relationship. Conversely, inaccurate, irrelevant information was associated with a deterioration in the relationship, as was the doctor feeling that the patient was challenging his or her authority, not having enough time to discuss the request, and not doing what the patient wanted. Practice characteristics were not associated with a positive or negative impact on the doctor-patient relationship. On multivariate analysis, the most important factor independently associated with an improved doctor-patient relationship was the doctor doing what the patient wanted (Table 3).
Effects of the Patient’s Talking about a DTCA on the Doctor-Patient Relationship
Doctors Who Feel Challenged
Twelve percent (95% CI, 10 to 16%) of doctors felt that their authority was being challenged by the patient during the discussion about DTCA (Table 4). On univariate analysis, doctors were more likely to feel challenged if the patient wanted a specific intervention, if the intervention was not clinically indicated, if the doctor did not do what the patient wanted, or if the doctor did not know the patient well enough to have good communication (Table 4). Multivariate analysis confirmed that these responses by the doctor, rather than practice characteristics, were independently associated with feeling challenged (Table 4).
Factors Associated with Respondents Feeling That Their Authority Was Being Challenged during the Discussion about DTCA
Effect on Quality of Care, Health Outcomes, and Health Service Utilization
Patients’ Reasons for Talking about DTCA During a Visit
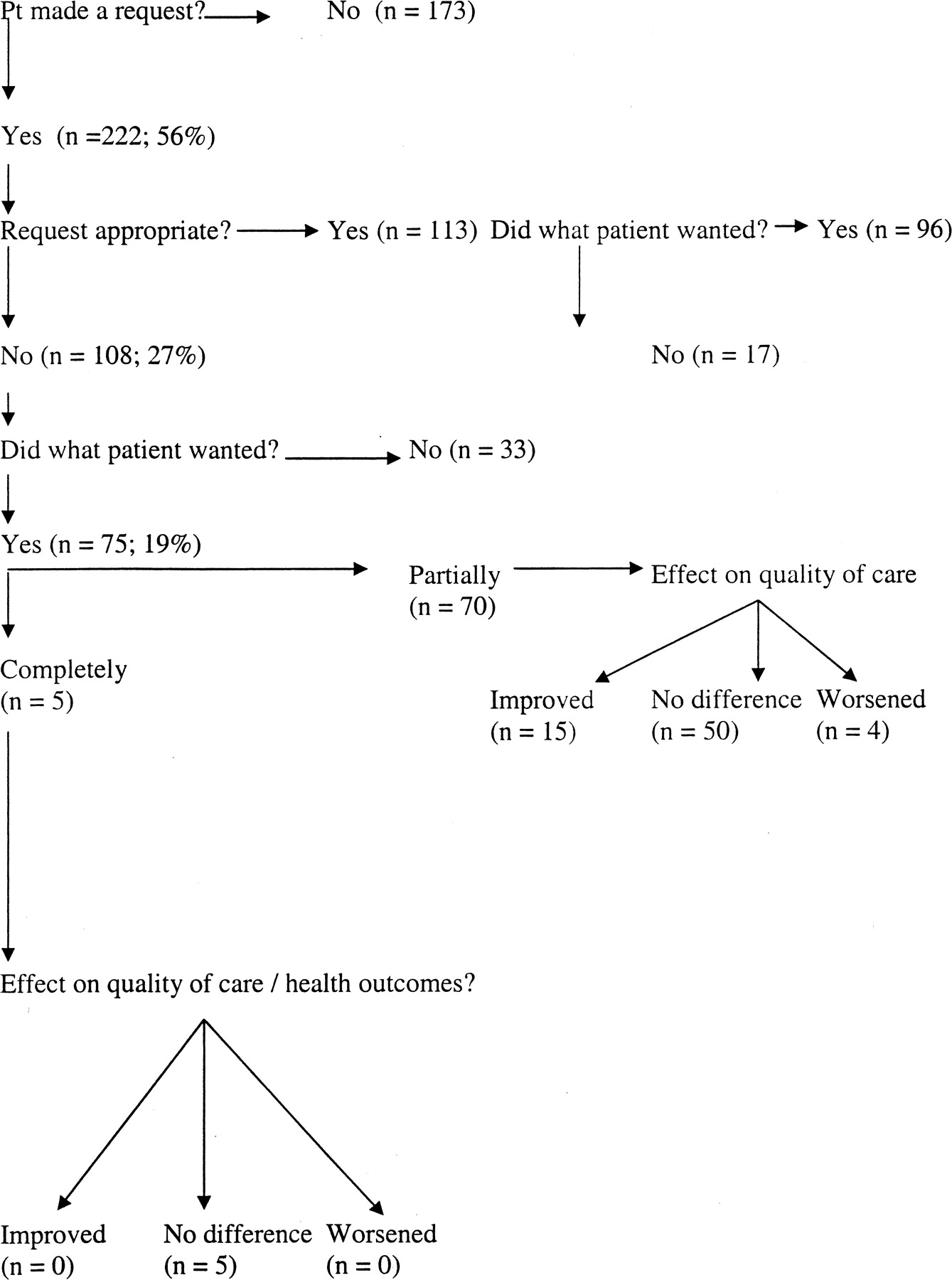
In 56% (95% CI, 51 to 61%; n = 222) of the visits in which patients talked about DTCA, the doctor perceived the patient’s reason for doing this as wanting at least 1 specific intervention, such as a test (n = 110; 28%), change in medication (n = 190; 48%), or referral (n = 54; 14%). In the remaining cases, the doctor perceived the patient as only wanting the doctor’s opinion.
Physician’s Response
Of the 222 cases in which the patient made a request, doctors deemed the request inappropriate for the patient’s health in 108 cases (Figure 3). In 75 of these cases (19% of all visits in which DTCA was discussed; 69% of inappropriate requests), the doctor did what the patient wanted, either completely (n = 5) or partially (n = 70). In 33 cases, the doctor did not do what the patient wanted at all.
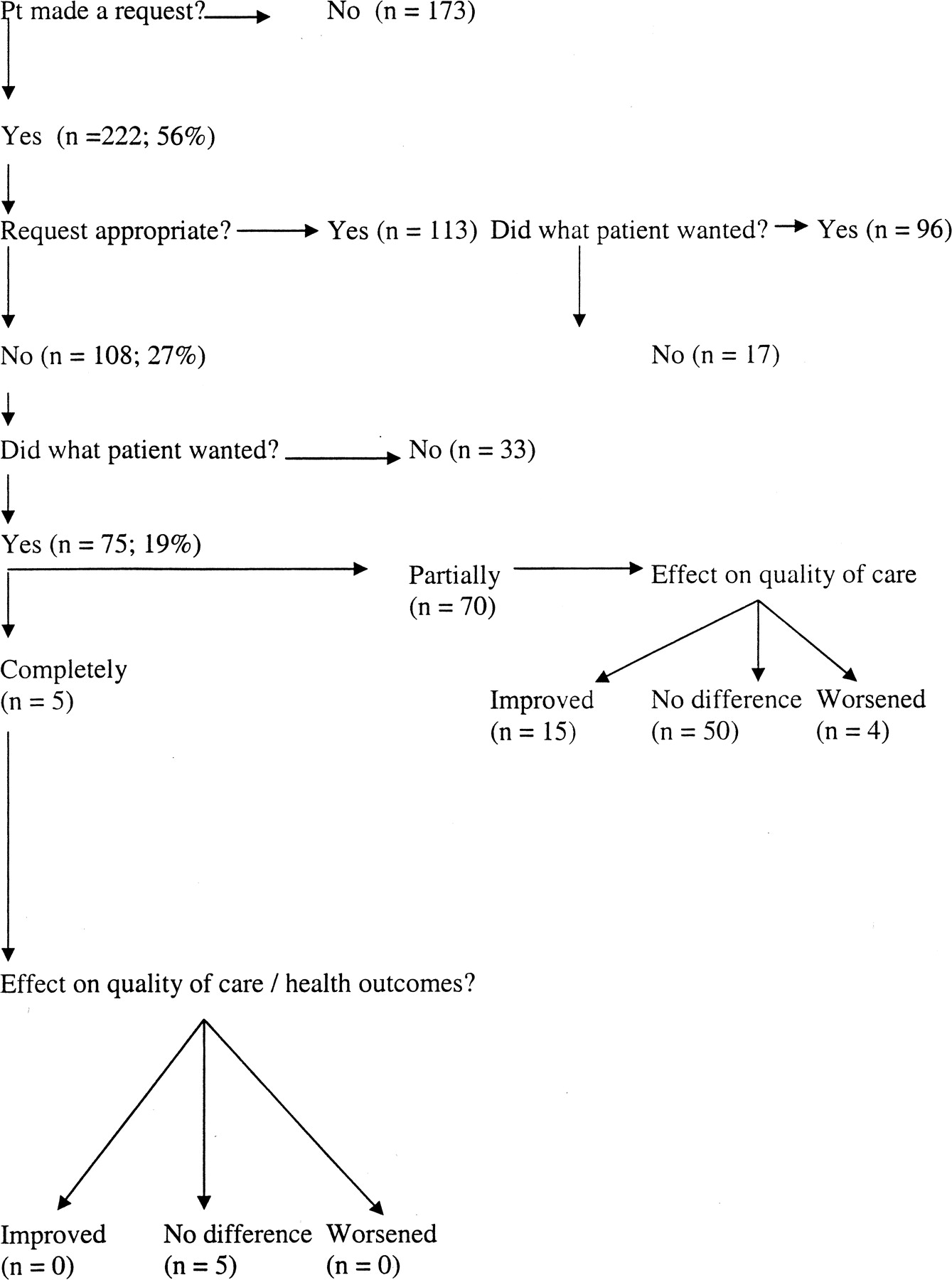
Outcomes when patients brought information from DTCA to a visit (n = 395).
Effect on Time-Efficiency
More physicians viewed discussing information from a drug advertisement as worsening the time efficiency of the visit (39%; 95% CI, 34 to 44%) than helping it (13%; 95% CI, 10 to 17%). On univariate analysis, factors associated with worsened time efficiency included inaccurate or irrelevant advertisements, patients wanting a specific intervention, and the doctor’s response. Not doing what the patient wanted was strongly associated with worsened time efficiency, as was thinking that the request was not appropriate or that the patient was challenging the doctor’s authority (Table 5). On multivariate analysis, inaccurate ads, specific requests, inappropriate requests, and the doctor’s feeling challenged were independently associated with worsened time efficiency (Table 5).
Effect of DTCA on the Time-Efficiency of the Visit
Effect on Quality of Care
We further analyzed the 75 cases in which the patient had made a request that was deemed inappropriate by the physician (Figure 3). In the 5 cases in which the physician did what the patient wanted completely, the impact of this on quality of care was viewed as neutral. In the 69 cases in which the doctor had done partially what the patient requested, the effect on quality of care was viewed as positive in 15 cases (22%), neutral in 50 cases (73%), and harmful in 4 cases (6%).
When the patient’s request was deemed appropriate by the doctor, the effect of doing what the patient wanted, either completely or partially, was viewed as positive or neutral in all cases. The findings were similar for effect on ultimate health outcomes (data not shown).
On multivariate analysis, several factors were independently associated with the patient making a request for an intervention that the doctor deemed inappropriate: the physician regarding the advertisement as not very or not at all accurate [odds ratio (OR) 2.0; 95% CI, 1.1 to 3.5]; the physician regarding patients as poor (rather than fair to excellent) at assessing the relevance of a drug ad (OR 2.2; 95% CI, 1.2 to 4.2), and the physician feeling that he or she did not know the patient well enough to have good communication (OR 5.4; 95% CI, 1.1 to 26.2).
Discussion
We found that DTCA has complex effects on quality of care and health service utilization. DTCA results in patients making almost as many inappropriate requests as appropriate ones. This puts physicians in a quandary, facing 3 conflicting ethical obligations. First, physicians aim to “do no harm.” Second, physicians seek to maintain and develop a strong doctor-patient relationship because it enhances future care and health outcomes. In addition, patient satisfaction is now used as a benchmark for quality of care and, as such, may determine physician income. Third, physicians have a duty to ensure fair allocation of health care resources and avoid wasteful expenditure. In the United States, such stewardship of societal resources is regarded as a weaker obligation than promoting the well-being of the individual patient.16–18 We found that physicians find responding to inappropriate requests time-consuming and that they often seem to acquiesce to such requests as long as the patient is not harmed. Thus, physicians attempt to mitigate negative effects of DTCA but at the cost of physician time or health care dollars. Furthermore, more doctors perceive the effect on the relationship as beneficial than harmful, but this is dependent on physicians doing what the patient wants, a finding confirmed in our forthcoming article presenting patients’ views.
Our findings have several implications for maximizing the benefits of DTCA while minimizing the harms. Inaccurate DTCA increases costs without improving health outcomes. Increased regulation of DTCA may ensure that information in advertisements is accurate and includes possible harms of treatment, as well as nonpharmacological alternatives.
In addition, patients need stronger skills in critically appraising drug advertisements to determine whether the material is personally relevant and accurate. Patients should seek the physician’s opinion on the relevance and accuracy of information in DTCA. This would both strengthen the doctor-patient relationship and avoid clinically inappropriate interventions. Just as physicians need to acknowledge that patients are expert in knowing their own health utilities, patients need to recognize physician clinical judgment.
Finally, physicians need to learn how to negotiate inappropriate requests efficiently without jeopardizing the doctor-patient relationship or feeling that patients are challenging their authority. Enhanced communication skills may enable doctors to follow their professional judgment, without damaging the doctor-patient relationship.19
Methodological Issues
Several methodological issues limit the generalizability of our findings. First, this article reports on a secondary analysis of an extant data set, so not all hypotheses could be evaluated with the desired precision. Second, we have no objective measures of the appropriateness of patient requests; however, because this is a professional judgment of the type clinicians make daily, respondents’ opinions have a degree of face validity. Finally, the response rate is moderate at 53%, despite every effort to maximize it. However, comparison of unweighted with weighted data suggests that the sample obtained was representative of US physicians, and sampling weights were applied to adjust for survey nonresponse.
Conclusions
DTCA can have both good and bad effects on the doctor-patient relationship and health service utilization. The benefits can be maximized and the harms minimized by increasing the accuracy and relevance of the information in the advertisements, enhancing physicians’ communication and negotiation skills, and encouraging patients to respect physicians’ clinical expertise.
Acknowledgments
We are grateful to Kinga Zapert and Rachel Turner of Harris Interactive Inc. for developing and fielding the survey instrument and to Joseph Catania, PhD, director of the Health Survey Research Unit, for advice on the analytical strategy.
Notes
This project was funded by the Robert Wood Johnson Foundation. EM was a Harkness Fellow in Health Care Policy 2001–02, supported by the Commonwealth Fund.
- Received for publication March 24, 2003.
- Revision received March 24, 2003.




{kind=link}
{kind=link}
{kind=link}