
Article Figures & Data
Figures
- Figure 1.
Assumptions of “usual care setting” for a decentralized, primary care perspective: Assumptions are based on the prevailing primary care infrastructure at the time of the rating process in 2022.27,28 Abbreviations: LDCT, low-dose CT; LCS, Lung cancer screening; CMS, Centers for Medicare and Medicaid Services.
- Figure 2.
Comparison of least and most pragmatic trials illustrated on the PRECIS-2 wheel: The Lung Screening Study and the ITALUNG trial were the most pragmatic studies, while the Danish Lung trial was the least pragmatic. The organization domain was unratable for the Danish Lung trial due to inadequate information available in manuscripts to complete a rating. Abbreviation: PRECIS, PRagmatic Explanatory Continuum Indicator Summary.
- Figure 3.
Composite ratings of PRECIS-2 domains: Composite ratings were calculated by averaging the domain score for each randomized controlled trial. If a domain was unratable the score was averaged over the number of studies with available rating data. Abbreviation: PRECIS, PRagmatic Explanatory Continuum Indicator Summary.
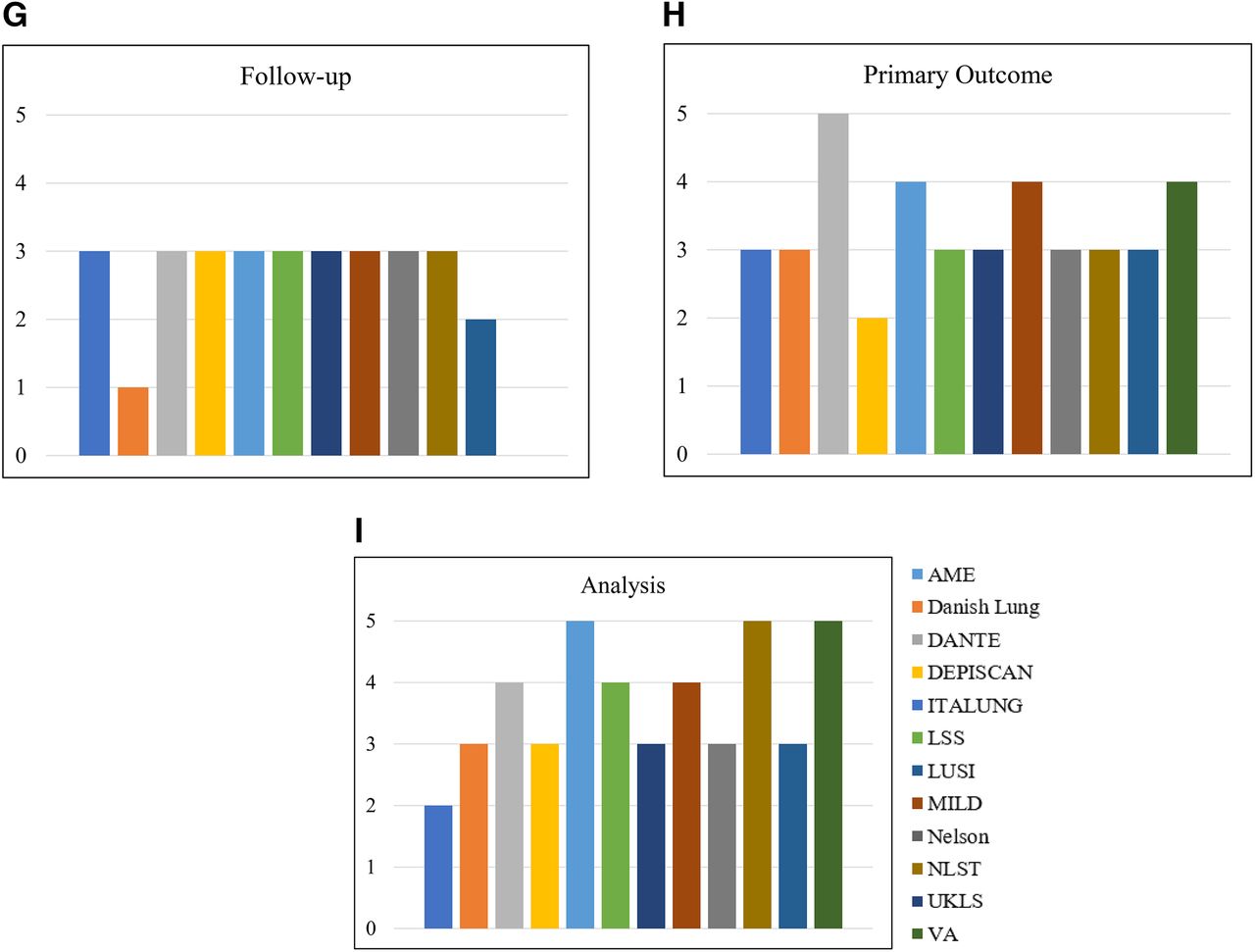
- e-Figure 1.
*Spread of PRECIS-2 ratings over each domain. a) eligibility criteria, b) recruitment path, c) setting, d) organization, e) flexibility (delivery by staff), f) flexibility (adherence), g) follow-up, h) primary outcome, g) analysis. *If a domain was classified as unratable the study column is left empty on each chart. Abbreviation: PRECIS, PRagmatic Explanatory Continuum Indicator Summary.
e-Figure 1. Continued
Appendix 1













Tables
PRECIS-2 Domain Domain Description* Completely Explanatory
(PRECIS-2 anchor = 1)Equally Explanatory/Pragmatic
(PRECIS-2 anchor = 3)Completely Pragmatic
(PRECIS-2 anchor = 5)1) Eligibility Criteria Who is selected to participate in the trial? Sample much more narrow than representative population (meets USPSTF or CMS guidelines) Most “typical” participants included some exclusions that limit study population Sample representative of population expected to receive intervention in usual care setting (meets USPSTF or CMS guidelines) 2) Recruitment Path How are participants recruited in the trial? General advertising without relevance to usual care population, recruitment requires extra effort Some extra effort/resources used to recruit beyond usual care Participants recruited unobtrusively during clinic visits 3) Setting Where is the trial being done? Few or one clinical sites that are not at all representative of usual care site More than one clinical sites that is partially representative of usual care Multiple sites nearly identical to usual care 4) Organization What expertise and resources are needed to deliver the intervention? Intervention requires many extra hours of staff time or infrastructure Intervention requires some extra time of infrastructure Intervention integrated into usual care and requires no extra time or resources 5) Flexibility (delivery by staff) How should the intervention be delivered? Intervention is protocol-driven with extensive oversight from clinicians Intervention allows flexibility at discretion of clinician Intervention oversight and follow-up managed by clinician 6) Flexibility (adherence) What measures are in place to make sure participants adhere to the intervention? Close monitoring to maximize participant adherence Few strategies to monitor and increase adherence Methods to maximize adherence within realm of usual care (i.e., send reminders) 6) Follow-up How closely are participants followed-up? Frequent visits for data collection during intervention period Some added visits for data collection during intervention No additional visits than what would be completed in usual care 7) Primary Outcome How relevant is it to participants? Measures/terms collected not relatable to participants/society and requires additional training to measure Measures/terms somewhat understandable to participants/society and can be assessed in usual care Measures/terms understood by participants/society and easy to assess 8) Primary Analysis To what extent are all data included? Analysis excludes data from individuals with poor adherence or missing data (“per protocol analysis”) Data from all study participants included but rigor slightly reduced Data from all participants included with imputation if needed Abbreviations: CMS, Centers for medicare and medicaid services; PRECIS, PRagmatic Explanatory Continuum Indicator Summary.
*Domain descriptions are from Loudon, et al. BMJ, 2015.19
Study Country Study Design Eligibility Criteria Based on Smoking History LDCT Arm Characteristics Control Arm Characteristics Number of Study Sites Overall PRECIS-2 Score* AME Thoracic Surgery Collaborative Group (AME)31 China 1:1 randomization
• Control: No screening
• LDCT frequency: Baseline and one biennial scan
• Ages: 45–70
• Smoking history: Minimum 20 pack years, current or quit within past 10 years.
• Other: also enrolled based on additional risk factors, did not necessarily need smoking history
• n = 3,512
• Mean age (±SD): 59.9 (±5.8)
• Female: 54%
• Currently smoke: 21%
• n = 3,145
• Mean age (±SD): 59.7 (±5.8)
• Female: 53%
• Currently smoke: 22%
1 screening site 2.83 (±0.41) DANTE32 Italy 1:1 randomization
• Control: No additional follow-up
• LDCT frequency: Baseline and four annual
• Age: 60–74
• Smoking history: Minimum 20 pack years, current or quit within past 10 years
• Other: Only males included
• n = 1,264
• Mean age: 64.6 (SEM 0.14)
• Female: 0%
• Non-white: NR
• Currently smoke: 56%
• n = 1,186
• Mean age: 64.6 (SEM 0.12)
• Female: 0%
• Non-white: NR
• Currently smoke: 57%
3 cancer centers within same network 3.00 (±1.00) DESPISCAN33 France 1:1 randomization
• Control: Chest radiograph
• LDCT frequency: Baseline and two annual
• Ages: 50 to 75
• Smoking history: ≥ 15 cigarettes per day for 20 years, current or quit within 15 years
• n = 385
• Median age (range): 56 (47 to 75)
• Female: 29%
• Non-white: NR
• Currently smoke: 65%
• n = 380
• Median age (range): 56 (47 to 76)
• Female: 30%
• Non-white: NR
• Currently smoke: 64%
14 centers 3.11 (±0.78) Danish Lung Cancer Screening Trial (DLCST)34 Denmark 1:1 randomization
• Control: No screening
• LDCT frequency: Baseline and four annual
• Ages: 50–70
• Smoking history: Minimum 20 pack years, current or quit after age of 50 and less than 10 years prior
• n = 2,052
• Age over 65: 9%
• Female: 45%
• Non-White: NR
• Currently smoke: 77%
• n = 2,052
• Age over 65: 9%
• Female: 44%
• Non-White: NR
• Currently smoke: 75%
1 medical center 2.12 (±0.83) ITALUNG35 Italy 1:1 randomization
• Control: No screening
• LDCT frequency: Baseline and three annual
• Ages: 55–69
• Smoking history: Minimum 20 pack years, current or quit within past 10 years
• n = 1,613
• Age over 65: 18%
• Female: 36%
• Currently smoke: 66%
• n = 1,593
• Age over 65: 19%
• Female: 35%
• Currently smoke: 64%
3 screening centers in same region 3.33 (±0.87) Lung Screening Study (LSS)36 United States 1:1 randomization
• Control: Chest radiograph
• LDCT frequency: Baseline and one annual
• Ages: 55 to 74
• Smoking history: 30 pack-years and currently smoke or quit within past 10 years
• n = 1,660
• Age > 65: 32%
• Female: 42%
• Non-White: NR
• Currently smoke: 58%
• n = 1,658
• Age ≥ 65: 32%
• Female: 41%:
• Non-White: NR
• Currently smoke: 57%
6 cancer/medical centers 3.33 (±0.50) German Lung Cancer Screening Intervention Trial (LUSI)37 Germany 1:1 randomization
• Control: No screening
• LDCT frequency: Baseline and four annual
• Age: 50–69
• Smoking history: 1) 25 cigarettes for 15 years or 2) 10 cigarettes for 30 years, must have quit within past 10 years
• n = 2,029
• Age over 65: 11%
• Female: 35%
• Non-White: NR
• Currently smoke: 38%
• n = 2,023
• Age over 65: 11%
• Female: 35%
• Non-White: NR
• Currently smoke: 38%
1 cancer research Center 2.86 (±1.07) Multicentric Italian Lung Detection (MILD)38 Italy 1:1:1 randomization (biennial, annual, control)
• Control: No screening
• LDCT frequency: Baseline and five annual or baseline and three biennial
• Ages: 49–75
• Smoking history: Minimum 20 pack years, current or quit within past 10 years
• n (annual) = 1190
• n (biennial) = 1186
• Age >65 (annual): 15%
• Age >65 (biennial): 15%
• Female (annual): 32%
• Female (biennial): 31%
• Currently smoke (annual): 69%
• Currently smoke (biennial): 68%
• n = 1,723
• Age >65: 13%
• Female: 37%
• Currently smoke: 90%
1 cancer institution 3.00 (±1.15) Dutch-Belgian Randomized Lung Cancer Screening Trial (NELSON)2 Netherlands/Belgium 1:1 randomization
• Control: No screening
• LDCT frequency: Baseline and follow-up at year 1, year 3. And year 5.5 (1 year, 2 years, and 2.5 year intervals
• Ages: Adult (not specified)
• Smoking history: 1) 15 cigarettes/day for 25 years or 2) 10 cigarettes/day for 30 years, current or quit within past 10 years
• n = 7,900
• Age ≥ 65: 17%
• Female: 17%
• Currently smoke: 56%
• n = 7,892
• Age ≥ 65: 17%
• Female: 16%
• Currently smoke: 55%
4 screening centers 2.78 (±0.44) National Lung Screening Trial (NLST)1 United States 1:1 randomization
• Control: Chest radiograph
• LDCT frequency: Baseline and two annual
• Age: 55 to 74
• Smoking history: Minimum 30 pack years, current or quit within past 15 years
• n = 26,722
• Age ≥ 65: 27%
• Female: 41%
• Currently smoke: 48%
• n = 26,732
• Age ≥ 65: 27%
• Female: 41%
• Currently smoke: 52%
33 screening centers 3.11 (±0.78) UK Lung Cancer Screening (UKLS)39 United Kingdom 1:1 randomization
• Control: No screening
• LDCT frequency: based on work-up protocol
• Ages: 50 to 75
• Other: 5-year lung cancer risk of ≥5%, calculated by Liverpool Lung Project
• n = 2,028
• Mean age (S.D.): 67.1 (4.1)
• Female: 25%
• Currently smoke: 38%
• n = 2,027
• Mean age (SD): 66.9 (4.1)
• Female: 26%
• Currently smoke: 39%
2 hospitals 2.55 (±0.53) VA Demonstration Project26 United States N/A† • Age: 55 to 80
• Smoking history: Minimum 30 pack year, current or quit within 15 years
• n = 2,106
• Mean Age (SD): 64.9 (5.1)
• Female: 4%
• Currently smoke: 57%
N/A† 8 sites affiliated with academic medical centers 3.00 (±1.19) ↵* PRECIS-2 ratings are presented as mean (±standard deviation). Each rating anchor was developed for the decentralized primary care lens.
† Study design and control arm characteristics are not available for the VA Demonstration Project because it is not a randomized controlled trial.
Abbreviations: LDCT, low-dose computed tomography; PRECIS, PRagmatic Explanatory Continuum Indicator Summary; SD, standard deviation; SEM, standard error mean.
- Table 3.
Comparison and Rationale for PRECIS-2 Ratings of Least and Most Pragmatic Randomized Controlled Trials
PRECIS-2 Domain Most Explanatory Trial (Danish Lung) First Most Pragmatic Trial (Lung Screening Study) PRECIS-2 Rating Description and Rationale for Domain Rating PRECIS-2 Rating Description and Rationale for Domain Rating Eligibility criteria 2 • Age/Smoking History Inclusion: 50–70 years and minimum 20 pack year smoking history, currently smoke or quit within past 10 years.
• Important exclusion: If formerly smokes, must have quit after age 50.
• Rationale: Only including individuals through 70 years, having quit smoking within past 10 years, and must have quit smoking after age 50 excludes some typical LCS-eligible individuals.
4 • Age/Smoking History Inclusion: 55–74 and minimum of 30 pack year smoking history, currently smoke or quit within past 10 years.
• Important exclusion: Participation in another cancer prevention trial
• Rationale: Eligibility is slightly less inclusive of current LCS-eligible individuals by CMS guidelines, with added exclusion that does not match current eligibility.
Recruitment path 2 • Interested individuals responded to advertisements in regional newspaper and weeklies.
• Rationale: Recruitment completed without relevance to LCS population, but didn’t appear to utilize a lot of extra effort or incentive.
3 • Participants recruited from sites participating in the Prostate, Lung, Colon, and Ovarian screening trials. Recruitment through flyers and clinician recommendation.
• Rationale: Recruitment completed at research centers with existing staff and partially recruited through clinician recommendation.
Setting 2 • Screening completed at one medical center.
• Rationale: Only one screening site, however, appeared partially representative of usual care sites.
3 • Study completed at six academic or cancer centers with specialized resources.
• Rationale: Most study sites are academic medical centers and not completely representative of usual care.
Organization Not ratable Adequate information not available in manuscripts to rate organization domain. 3 • Primary care involved in specialist referral for high-risk nodules. No tobacco cessation was incorporated in study.
• Rationale: Primary care had discretion to follow and work-up positive, high-risk nodules, however, annual screening was considered a study procedure.
Flexibility (staff) 1 • Diagnostic follow-up was very specialized and protocol driven with no discretion for clinicians.
• Rationale: No discretion for clinicians, especially primary care, for LDCT results follow-up and work-up
4 • Work up of positive results left to participants’ medical team, although referrals and suggested diagnostic algorithms were provided if asked.
• Rationale: Primary care had flexibility for work-up of positive LDCT results with suggested diagnostic algorithms available if needed.
Flexibility (adherence) 3 • Tobacco cessation was offered and annual visits with high adherence across all screening rounds.
• Rationale: Annual study visits are not too burdensome and the same frequency as annual screening although study visits are more involved than a yearly LDCT.
3 • Yearly screening for negative scans, positive scans worked-up outside of study but research called to make sure at 4 and 8 weeks to make sure participants were being evaluated.
• Rationale: Study personnel made a maximum of two phone calls to follow-up on individuals with positive results.
Follow-up 1 • Annual study visits with pulmonary function tests and additional data collection.
• Rationale: Annual pulmonary function tests and data collection viewed as much more extensive compared to an annual LDCT.
3 • Results were mailed to participants within 3 weeks of scan. Positive results were referred to primary care for diagnostic follow-up although study teams made calls at 4 and 8 weeks to urge participants to receive follow-up. Study evaluated work-ups from medical record abstraction.
• Rationale: Minimum follow-up on positive results as work-up was completed outside study. Additional data collection from medical record abstraction may require extra time and training for abstractors.
Primary outcome 3 • Primary outcome included a reduction of lung cancer specific mortality by 25% in the LDCT arm.
• Rationale: While mortality reduction is easily understandable by participants and policy makers, this outcome is population health focused and hard to assess in usual care.
3 • Feasibility trial for the National Lung Screening Trial with primary goal of determining feasibility for accrual for larger LDCT trials.
• Rationale: Primary outcome as a feasibility trial not completely understandable by LCS participants/society, however, is very relevant as this trial led to the much larger National Lung Screening Trial.
Analysis 3 • Study procedures appeared to include all data from all participants in the analysis, but it remained unclear how data from participants that were lost to follow-up was handled.
• Rationale: Analysis rigor reduced slightly due to lack of clarity around how participants lost to follow-up were treated in analysis.
4 • NCI responsible for scientific oversight and data analysis. Ran analyses with and without individuals that were later found to be ineligible (many due to participation in the PLCO trial).
• Rationale: Primary analyses excluded individuals that were found to be ineligible after study enrollment and randomization, but included a secondary analysis with all enrolled participants and did not find any differences in results.
PRECIS-2 Domain Second Most Pragmatic Trial (ITALUNG Study) PRECIS-2 Rating Description and Rationale for Domain Rating Eligibility criteria 3 • Age/Smoking History Inclusion: 55–69 and minimum of 20 pack year smoking history, currently smoke or quit within past 10 years.
• Important Exclusion: Quit smoking >10 years prior (if formerly smoked), prior cancer history (except non-melanoma skin), general conditions precluding thoracic surgery.
• Rationale: Eligibility is less inclusive of current LCS-eligible individuals by CMS guidelines, but includes most typical LCS eligible individuals.
Recruitment path 3 • Participants recruited through letters sent to residents aged 55–69 and lived in three regions where the screening centers were located and were registered with general practitioners involved with the trial.
• Rationale: Recruitment matched age eligibility and linked with primary care, however, was completed by mass mailing that required extra personnel time.
Setting 3 • Study completed at three screening centers in the Tuscany region of Italy with a single coordinating center.
• Rationale: Study sites affiliated with a Cancer Prevention Research center and not completely representative of usual care.
Organization 3 • Primary care counseled and enrolled participants in study and supported them to follow the study protocol. Tobacco cessation incorporated in study.
• Rationale: Primary care involved through direct contact with study participants and required some additional staff time beyond usual care.
Flexibility (staff) 2 Although primary care was involved for support, LDCT diagnostic follow-up was protocol-driven.
Rationale: Explanatory because follow-up of positive and negative LDCT results was protocol driven with minimum discretion for primary care.
Flexibility (adherence) 4 Study participants with negative results “invited” to three additional rounds of screening and participants with positive results followed work-up protocol with assumed support from primary care.
Rationale: “Inviting” participants to follow-up rounds and procedures with support from primary care was considered as encouragement for participants to comply.
Follow-up 3 Negative results were mailed to participants within 3 weeks of LDCT. Positive results conveyed by phone call from screening center with follow-up from a pulmonologist. Sputum collected at baseline and after positive result. Information on control arm collected with annual interviews of participant/primary care clinician and cancer registry matches.
Rationale: LDCT follow-up was completed by protocol that was considered standard of care. Sputum collection and control arm interviews require additional time.
Primary outcome 4 Primary outcome was to contribute to the evaluation of LDCT efficacy to lower lung cancer specific and all-cause mortality as part of the larger European Initiative.
Rationale: Primary outcome is relevant for participants and policy makers and was intended to be pooled with additional European studies for a population health level mortality reduction.
Analysis 5 All analyses performed with intention-to-treat principle, study ‘drop-outs’ were included in the active (LDCT) arm.
Rationale: Data from all individuals were included in all analyses and manuscripts included information about how exclusions were included.
Abbreviations: CMS, Centers for medicare and medicaid services; LCS, lung cancer screening; LDCT, low-dose computed tomography; NCI, National Cancer Institute; PRECIS, PRagmatic Explanatory Continuum Indicator Summary.
- Table 4.
Mean Scores, Number of un-Ratable Domains, Number of Domains Requiring Consensus and Arbitration*
PRECIS-2 Domain Mean Score* (± SD) Number of Studies with Domains Not Ratable Number of Studies Where Scoring Required a Consensus between an Explanatory (<3) or Pragmatic (>3) or If un-Ratable† Number of Studies Where Scoring Required Arbitration by a Third Reviewer (EAH) Eligibility criteria 2.91 (±0.83) 0/12 (0%) 2/12 (17%) 1/12 (8%) Recruitment path 2.54 (±0.69) 0/12 (0%) 1/12 (8%) 0/12 (0%) Setting 2.50 (±0.97) 1/12 (8%) 2/12 (17%) 0/11 (0%) Organization 2.86 (±0.69) 4/12 (33%) 4/12 (33%) 0/12 (0%) Flexibility (staff) 2.62 (±0.92) 3/12 (25%) 4/12 (33%) 2/12 (17%) Flexibility (adherence) 3.18 (±0.40) 0/12 (0%) 4/12 (33%) 0/12 (0%) Follow-up 2.73 (±0.65) 1/12 (8%) 3/12 (25%) 1/12 (8%) Primary outcome 3.27 (±0.79) 0/12 (0%) 4/12 (33%) 0/12 (0%) Analysis 3.54 (±0.93) 0/12 (0%) 1/12 (8%) 1/12 (8%) Abbreviation: PRECIS, PRagmatic Explanatory Continuum Indicator Summary.
*Mean ratings were calculated by averaging the domain score for each randomized controlled trial. If a domain was un-ratable the score was averaged over the number of studies with available rating data.
*PRECIS-2 ratings are presented as mean (±standard deviation).
†Consensus was reached between two primary raters (SZ and MM).
Study Manuscripts Provided for PRECIS-2 Ratings AME Thoracic Surgery Collaborative Group (AME) 1) Yang W, Qian F, Teng J, et al. Community-based lung cancer screening with low-dose CT in China: Results of the baseline screening. Lung Cancer. 2018;117:20 to 26. doi:10.1016/j.lungcan.2018.01.003
DANTE 1) Infante M, Lutman FR, Cavuto S, et al. Lung cancer screening with spiral CT: baseline results of the randomized DANTE trial. Lung Cancer. 2008;59(3):355 to 363. doi:10.1016/j.lungcan.2007.08.040.
2) Infante M, Cavuto S, Lutman FR, et al. A randomized study of lung cancer screening with spiral computed tomography: three-year results from the DANTE trial. Am J Respir Crit Care Med. 2009;180(5):445 to 453. doi:10.1164/rccm.200901-0076°C.
3) Infante M, Cavuto S, Lutman FR, et al. Long-Term Follow-up Results of the DANTE Trial, a Randomized Study of Lung Cancer Screening with Spiral Computed Tomography. Am J Respir Crit Care Med. 2015;191(10):1166 to 1175. doi:10.1164/rccm.201408-1475°C.
DEPISCAN 1) Blanchon T, Bréchot JM, Grenier PA, et al. Baseline results of the Depiscan study: a French randomized pilot trial of lung cancer screening comparing low dose CT scan (LDCT) and chest Radiograph (CXR). Lung Cancer. 2007;58(1):50 to 58. doi:10.1016/j.lungcan.2007.05.009.
Danish Lung Cancer Screening Trial (DLCST) 1) Pedersen JH, Ashraf H, Dirksen A, et al. The Danish randomized lung cancer CT screening trial--overall design and results of the prevalence round. J Thorac Oncol. 2009;4(5):608 to 614. doi:10.1097/JTO.0b013e3181a0d98f.
2) Saghir Z, Dirksen A, Ashraf H, et al. CT screening for lung cancer brings forward early disease. The randomized Danish Lung Cancer Screening Trial: status after five annual screening rounds with low-dose CT. Thorax. 2012;67(4):296 to 301. doi:10.1136/thoraxjnl-2011 to 200736.
3) Wille MM, Dirksen A, Ashraf H, et al. Results of the Randomized Danish Lung Cancer Screening Trial with Focus on High-Risk Profiling. Am J Respir Crit Care Med. 2016;193(5):542 to 551. doi:10.1164/rccm.201505-1040°C
ITALUNG 1) Wille MM, Dirksen A, Ashraf H, et al. Results of the Randomized Danish Lung Cancer Screening Trial with Focus on High-Risk Profiling. Am J Respir Crit Care Med. 2016;193(5):542 to 551. doi:10.1164/rccm.201505-1040°C.
2) Lopes Pegna A, Picozzi G, Falaschi F, et al. Four-year results of low-dose CT screening and nodule management in the ITALUNG trial. J Thorac Oncol. 2013;8(7):866 to 875. doi:10.1097/JTO.0b013e31828f68d6.
3) Paci E, Puliti D, Lopes Pegna A, et al. Mortality, survival and incidence rates in the ITALUNG randomized lung cancer screening trial. Thorax. 2017;72(9):825 to 831. doi:10.1136/thoraxjnl-2016 to 209825.
Lung Screening Study (LSS) 1) Gohagan J, Marcus P, Fagerstrom R, et al. Baseline findings of a randomized feasibility trial of lung cancer screening with spiral CT scan vs chest radiograph: the Lung Screening Study of the National Cancer Institute. Chest. 2004;126(1):114 to 121. doi:10.1378/chest.126.1.114.
2) Gohagan JK, Marcus PM, Fagerstrom RM, et al. Final results of the Lung Screening Study, a randomized feasibility study of spiral CT versus chest Radiograph screening for lung cancer. Lung Cancer. 2005;47(1):9 to 15. doi:10.1016/j.lungcan.2004.06.007.
3) Doroudi M, Pinsky PF, Marcus PM. Lung Cancer Mortality in the Lung Screening Study Feasibility Trial. JNCI Cancer Spectr. 2018;2(3):pky042. Published 2018 Sep 18. doi:10.1093/jncics/pky042.
German Lung Cancer Screening Intervention Trial (LUSI) 1) Becker N, Motsch E, Gross ML, et al. Randomized study on early detection of lung cancer with MSCT in Germany: study design and results of the first screening round. J Cancer Res Clin Oncol. 2012;138(9):1475 to 1486. doi:10.1007/s00432-012-1228-9.
2) Becker N, Motsch E, Gross ML, et al. Randomized Study on Early Detection of Lung Cancer with MSCT in Germany: Results of the First 3 Years of Follow-up After Randomization. J Thorac Oncol. 2015;10(6):890 to 896. doi:10.1097/JTO.0000000000000530.
3) Becker N, Motsch E, Trotter A, et al. Lung cancer mortality reduction by LDCT screening-Results from the randomized German LUSI trial. Int J Cancer. 2020;146(6):1503 to 1513. doi:10.1002/ijc.32486.
Multicentric Italian Lung Detection (MILD) 1) Pastorino U, Rossi M, Rosato V, et al. Annual or biennial CT screening versus observation in heavy smokers: 5-year results of the MILD trial. Eur J Cancer Prev. 2012;21(3):308 to 315. doi:10.1097/CEJ.0b013e328351e1b6.
2) Pastorino U, Silva M, Sestini S, et al. Prolonged lung cancer screening reduced 10-year mortality in the MILD trial: new confirmation of lung cancer screening efficacy. Ann Oncol. 2019;30(10):1672. doi:10.1093/annonc/mdz169.
Dutch-Belgian Randomized Lung Cancer Screening Trial (NELSON) 1) van Iersel CA, de Koning HJ, Draisma G, et al. Risk-based selection from the general population in a screening trial: selection criteria, recruitment and power for the Dutch-Belgian randomized lung cancer multi-slice CT screening trial (NELSON). Int J Cancer. 2007;120(4):868 to 874. doi:10.1002/ijc.22134.
2) Ru Zhao Y, Xie X, de Koning HJ, Mali WP, Vliegenthart R, Oudkerk M. NELSON lung cancer screening study. Cancer Imaging. 2011;11 Spec No A(1A):S79-S84. Published 2011 Oct 3. doi:10.1102/1470 to 7330.2011.9020.
3) Yousaf-Khan U, van der Aalst C, de Jong PA, et al. Final screening round of the NELSON lung cancer screening trial: the effect of a 2.5-year screening interval. Thorax. 2017;72(1):48 to 56. doi:10.1136/thoraxjnl-2016 to 208655.
4) de Koning HJ, van der Aalst CM, de Jong PA, et al. Reduced Lung-Cancer Mortality with Volume CT Screening in a Randomized Trial. N Engl J Med. 2020;382(6):503 to 513. doi:10.1056/NEJMoa1911793
National Lung Screening Trial (NLST) 1) National Lung Screening Trial Research Team, Aberle DR, Adams AM, et al. Baseline characteristics of participants in the randomized national lung screening trial [published correction appears in J Natl Cancer Inst. 2011 Oct 19;103(20):1560]. J Natl Cancer Inst. 2010;102(23):1771 to 1779. doi:10.1093/jnci/djq434.
2) National Lung Screening Trial Research Team, Aberle DR, Berg CD, et al. The National Lung Screening Trial: overview and study design. Radiology. 2011;258(1):243 to 253. doi:10.1148/radiol.10091808.
3) National Lung Screening Trial Research Team, Aberle DR, Adams AM, et al. Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med. 2011;365(5):395 to 409. doi:10.1056/NEJMoa1102873.
4) Aberle DR, DeMello S, Berg CD, et al. Results of the two incidence screenings in the National Lung Screening Trial. N Engl J Med. 2013;369(10):920 to 931. doi:10.1056/NEJMoa1208962.
UK Lung Cancer Screening (UKLS) 1) Field JK, Duffy SW, Baldwin DR, et al. UK Lung Cancer RCT Pilot Screening Trial: baseline findings from the screening arm provide evidence for the potential implementation of lung cancer screening. Thorax. 2016;71(2):161 to 170. doi:10.1136/thoraxjnl-2015 to 207140.
2) Field JK, Duffy SW, Baldwin DR, et al. The UK Lung Cancer Screening Trial: a pilot randomized controlled trial of low-dose computed tomography screening for the early detection of lung cancer. Health Technol Assess. 2016;20(40):1 to 146. doi:10.3310/hta20400.
3) Brain K, Lifford KJ, Carter B, et al. Long-term psychosocial outcomes of low-dose CT screening: results of the UK Lung Cancer Screening randomized controlled trial. Thorax. 2016;71(11):996 to 1005. doi:10.1136/thoraxjnl-2016 to 208283.
VA Demonstration Project 1) Kinsinger LS, Anderson C, Kim J, et al. Implementation of Lung Cancer Screening in the Veterans Health Administration. JAMA Intern Med. 2017;177(3):399 to 406. doi:10.1001/jamainternmed.2016.9022.
Abbreviation: PRECIS, PRagmatic Explanatory Continuum Indicator Summary.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}