
Abstract
Introduction: Social drivers of health (SDH) strongly influence health outcomes and disparities. Although systemic level change is vital to address the disparities driven by SDH, it is also crucial that health care organizations develop the ability to care for patients in a manner that accounts for social factors and their influence on patient health. Although primary care is a natural fit for health-related social needs (HRSN) screening and intervention, significant barriers can impede primary care’s effectiveness in this area.
Methods: We conducted 3 focus groups with family medicine clinicians, clinical staff, and social care workers in an academic medical center using a semistructured discussion guide to explore current practices, perceived benefits, barriers, and potential opportunities and approaches for integrating routine HRSN screening in primary care.
Results: 3 primary themes emerged from the focus groups. They included 1) the barriers to routine screening in primary care, including time, workload, emotional burden, patient factors, and team members’ fear of inadequacy of resources or their own ability; 2) the importance and benefit of HRSN screening, including the opportunity to improve patient care through increased care team awareness of the patient’s context, interventions to address HRSN, and improved relationships between the care team and the patient; and 3) recommendations for implementing routine screening in primary care, including opportunities to optimize workflow and technology, the importance of an electronic medical record (EMR)-integrated resource database, and the centrality of teamwork.
Discussion: Family medicine health care teams embrace the importance of HRSN screening and the potential for positive impact. However, there are vital barriers and considerations to address for HRSN screening to be effectively integrated into primary care visits.
- California Health Interview Survey
- Chronic Disease
- Community Medicine
- Family Medicine
- Focus Groups
- Patient Care Team
- Primary Health Care
- Social Determinants of Health
- Social Factors
Introduction
Social drivers of health (SDH) are the circumstances in which people live, play, learn, work, and interact, as well as the structural, political, and economic factors that shape those circumstances.1,2 Increasingly, SDH are recognized as both drivers of and potential targets for reducing health disparities and adverse health outcomes.3⇓–5
Accordingly, health care in the US has begun moving toward a model of care that considers individual patients’ social and behavioral risk factors for disease, known as health-related social needs (HRSN).6⇓⇓–9 For example, the Joint Commission now requires that organizations have a method of screening for HRSN.9⇓–11 Value-based approaches to health care, which have been gaining traction in the US, often seek to address HRSN to reduce health care spending.12,13 Primary care teams are uniquely positioned to identify and respond to HRSN because of their central role in caring for a large portion of the US population,14⇓⇓–17 and their ability to recognize the benefits of addressing HRSN.18 Family medicine clinicians, with their history of caring for patients within family and social contexts, have an orientation particularly compatible with considering social needs alongside medical issues.14,15,17 Correspondingly, the Accreditation Council for Graduate Medical Education now requires that family medicine residency programs provide training in identifying health disparities and addressing SDH.19
Given this increased impetus for screening for HRSN, attention to opportunities and barriers within primary care will be vital to its success. Overwhelmingly, primary care clinicians believe HRSN screening is important; however, primary care faces substantial challenges in delivering the recommended care already allocated to it.20,21 Only a minority of clinicians report routinely screening for HRSN, citing significant barriers including insufficient time and resources, lack of confidence in addressing needs, fears of patient discomfort, and clinician burnout.20,22,23 Therefore, we sought the experiences and perspectives of various family medicine health care team members on HRSN screening through focus groups.
Materials and Methods
Focus groups occurred in September and October 2022 at a large urban academic medical center in early preparation for HRSN screening. Recruitment was conducted through e-mail invitations. The recruitment target was 5 to 10 participants per group. When the cap was exceeded, the first 10 volunteers were chosen. The first focus group (n = 10) consisted of 4 medical assistants (MAs), 1 registered nurse, 2 licensed vocational nurses, 1 manager, and 2 patient service specialists (PSS). The second focus group (n = 8) consisted of 4 faculty, 3 residents, and 1 behavioralist. The third focus group (n = 5) consisted of 4 social workers (SW) and 1 community health worker (CHW).
The study was approved by the first author’s Institutional Review Board. Focus groups were conducted in-person by L.D. and L.P. and audio-recorded after written consent and verbal permission were granted. Participants were compensated for their time and received $25 merchandise cards and lunch. Focus groups were conducted in a semistructured format using a discussion guide developed by the authors after a review of the literature, followed by questions and probes based on participant responses.
Qualitative analyses were guided by an inductive approach to identify key themes that emerged from the data.24 First, 4 study team members (L.P., Q.J., F.J, and T.C.) read and reread the transcripts to become familiar with participants' perspectives and decrease analyst bias. Team members used reflexivity throughout the process to identify personal, interpersonal, and contextual factors affecting analysis. The study team undertook a thematic coding of the transcripts, using open coding to identify themes derived from the participants' own words. The team compared codes identified after reading 3 transcripts and came to a consensus on 15 codes that captured the focus group themes. Each transcript was subsequently coded by L.P. and 1 other author (Q.J., F.J, or T.C.). Each author highlighted quotes representative of the 15 codes. Discrepancies in coding were resolved through discussion and consensus.
Results
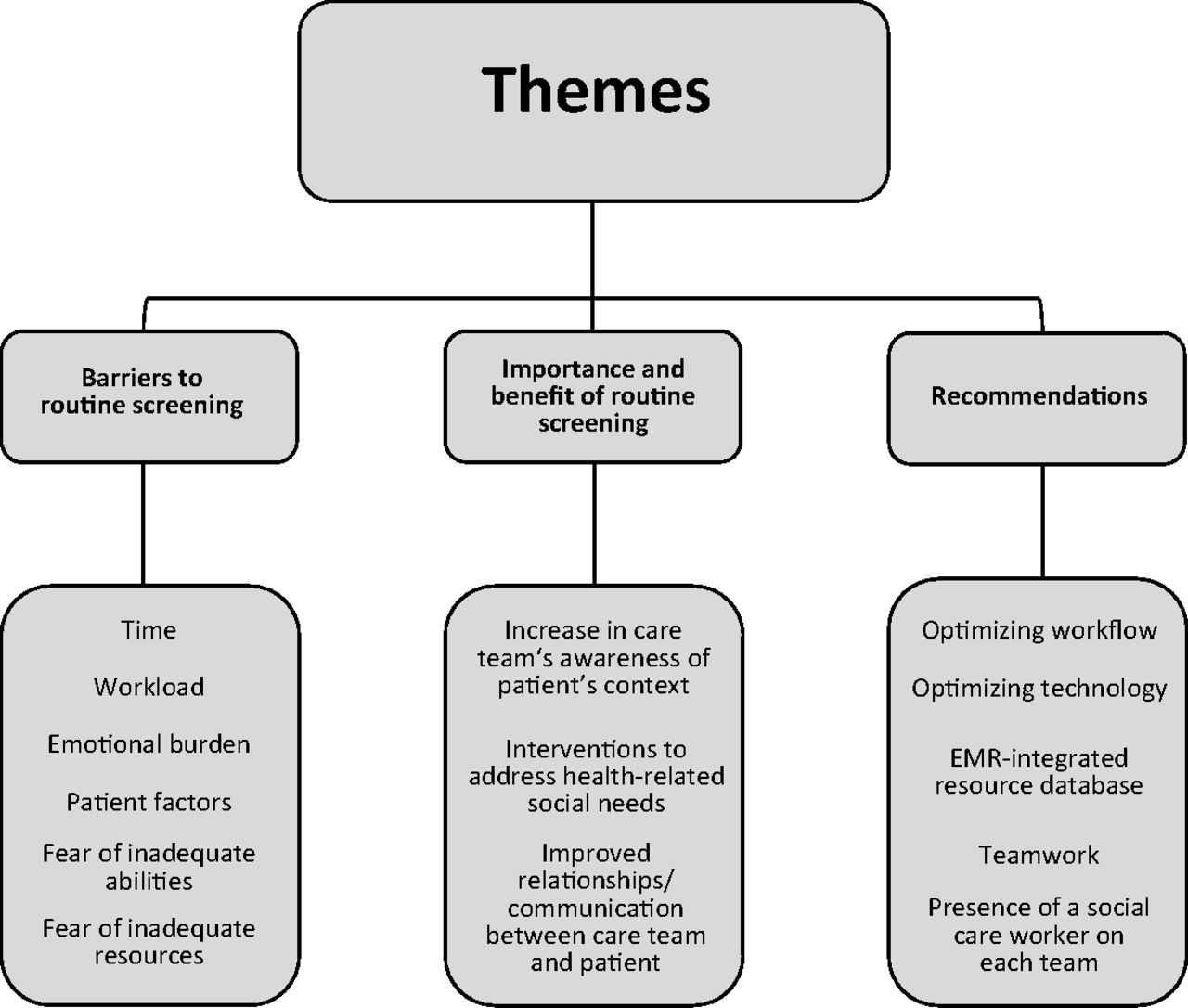
Three overriding themes emerged from the focus groups, each of which can be divided into subthemes (Figure 1): (1) Barriers to routine screening of HRSN in primary care; (2) Benefits of screening for HRSN; and (3) Recommended approaches for screening and addressing HRSN.

Focus group themes and subthemes.
Barriers to HRSN Screening
The significant challenges of incorporating HRSN screening and intervention into primary care visits was a large area of focus for all 3 groups (Table 1).
Participant Feedback and Quotations on Theme 1, “Barriers to Routine Screening of Health-Related Social Needs [HRSN] in Primary Care,” from Focus Groups Conducted from September to October 2022 in a Primary Care Setting at a Texas Academic Medical Center
Participants reported that a lack of time to talk with patients often prevents HRSN screening. They cited concerns about how HRSN creates delays for the patient in need as well as subsequent patients scheduled that day. Other factors mentioned were the paucity of financial incentives or reimbursement for addressing HRSN and the concern that needs uncovered by routine screening would overwhelm SW and clinical staff.
The emotional toll of discovering needs and the “burden of wanting to help [patients]” presented another barrier. Some participants described intense emotional responses, particularly when they do not feel they have adequate means of addressing patient needs. Fear of inadequacy also extended to the screening process or the team itself: “If I ask [patients] about [HRSN], I feel like they are going to want an answer from me on what to do about it, and I am not qualified to give them that kind of answer.” Other concerns centered around inadequate community resources or that screening without sufficient time could negatively impact patient-care team relationships.
Another recurrent theme was the role of trust: “You have to have a relationship with the patient before they open up…” SW participants mentioned how stigmas and fears that SW may work against the patient (eg, recommending alternate placement for the patient’s children) often lead to patient mistrust. Other factors included patients’ lack of recognition or admission of their need for assistance, and patients’ lack of awareness that primary care teams can assist with HRSN. Citizenship status and its impact on resource availability and the impact of digital literacy and internet access on electronic screening methods were also mentioned.
Importance and Benefits of Screening
Despite the barriers, participants emphasized the importance of HRSN screening (Table 2).
Participant Feedback and Quotations on Theme 2, “the Benefit of Routine Screening for Health-Related Social Needs in Primary Care,” from Focus Groups Conducted from September to October 2022 in a Primary Care Setting at a Texas Academic Medical Center
One of the most frequently described benefits was that HRSN screening gives “a more complete picture” of patients’ situations, allowing physicians to provide concrete resources such as discounted prescriptions or transportation vouchers, or to appropriately adapt patient care even in the absence of outside resources. An additional benefit mentioned was the ability to prioritize patient safety, particularly regarding intimate partner violence and depression.
Screening for and addressing HRSN can augment the care team’s connection to and communication with the patient. Participants pointed out the way screening “can open up that line of communication instead of [patients] feeling embarrassed about things and not wanting to bring it up.”
Recommendations
The third theme centered around recommended approaches for screening and intervention for HRSN (Table 3).
Participant Feedback and Quotations on Theme 3, “Recommendations for Screening and Interventions for Health-Related Social Needs,” from Focus Groups Conducted from September to October 2022 in a Primary Care Setting at a Texas Academic Medical Center
Participants discussed that screening should be done at new patient visits and Medicare Annual Wellness Visits, that all patients should be screened, and how screening is currently very inconsistent and often patient-initiated. Participants differed in opinion on whether MAs or physicians were best suited for conducting screening.
Physicians mentioned the importance of incorporating screening into electronic medical record (EMR) templates and that using patient portal questionnaires could help improve screening rates without overburdening care teams. Other suggestions included incorporating resources in patient after-visit summaries, building smart sets for resources, using electronic flags to indicate safety concerns, and using electronic devices or kiosks in clinics for patients to complete questions. Having a centralized, efficient, and up-to-date resource bank that integrates with the EMR was a strongly felt need.
Participants identified current gaps in resources, including housing, shelters for those experiencing intimate partner violence, and transportation. They highlighted the interconnectedness of HRSN, for example, between accessing food assistance and transportation. SW participants also cautioned about the need to assess eligibility before offering resources to patients.
Participants emphasized the importance of a patient-centered approach. Being mindful of whether patients desire assistance was a recurrent point, as was “being culturally competent when asking [screening] questions.”
Discussions on effective teamwork focused on engaging clinical staff in screening and provision of resources, effective coordination with SW, training all team members on community resources and processes, the need for on-site team members to help address patients’ HRSN, the need to hire additional team members such as resource coordinators and CHWs, and engaging existing team members such as interpreters and learners.
Discussion
Our findings expand on existing literature highlighting both opportunities and barriers in screening for HRSN. A study of clinicians screening for HRSN in low-income communities found screening challenging due to limited resources, but also found screening improved the care of patients.25 In 1 clinician survey, more than 90% thought HRSN screening could improve patient care, but two-thirds of physicians were not confident in their ability to address HRSN.20 A qualitative study of pediatric clinicians identified similar themes, including barriers, recommendations, patient factors, clinician confidence, clinician-patient relationships, and the potential for unintentional negative impact on relationships.26 Other studies have identified similar recommendations, including the need to develop robust community referral networks,27,28 integrate technology, and have onsite social service personnel27 whose presence reduces the stress of screeners.29
Our study is unique because it incorporates the perspectives not only of clinicians but of the entire family medicine health care team. Unique themes that emerged from our study, such as the centrality of teamwork and the importance and approach to engaging learners in screening, likely stem from the inclusion of participants in these additional roles.
Study limitations include a single institution study in an academic setting, which could limit generalizability. However, our findings were consistent with similar studies in other contexts.18,20,25 Focus groups allow exploration of diverse and conflicting perspectives; however, they can be susceptible to influence by dominant participants or moderators.30 The coders’ own experiences in patient care could also influence interpretation of findings. Although sample sizes were small, thematic saturation was reached, with consistency in the codes present across all 3 focus groups. Small numbers of participants in specific roles prevented identification of differing perspectives by specific roles, apart from the SWs, who were unique in highlighting the importance of differentiating patient “venting” from requests for assistance.
Directions for future research include exploring whether perspectives differ after HRSN screening has been implemented more widely. Additional research is needed to explore the cost-effectiveness of integrating resource coordinators into primary care teams and the efficacy of strategies to reduce barriers and improve efficacy of HRSN interventions.
To address the challenges to implementing HRSN screening identified in our study, health systems should ensure that primary care teams are empowered through education, resources, user-friendly referral processes, and team members dedicated to resource coordination.
Conclusions
This study explored perspectives of family medicine health care team members on routine screening for HRSN. Despite identifying many challenges, team members acknowledged the significant impact of social factors on patients’ health, suggesting that primary care is fertile ground for implementing screening.
Acknowledgments
We are grateful to the UTMB Center for Violence Prevention for funding this study and to the participants for generously sharing their time and insights.
Notes
This article was externally peer reviewed.
This is the Ahead of Print version of the article.
Funding: No outside funding was received for this study This study was funded internally by the University of Texas Medical Branch Center for Violence Prevention.
Conflict of interest: The authors have no conflicts of interest to disclose.
To see this article online, please go to: http://jabfm.org/content/00/00/000.full.
- Received for publication April 29, 2023.
- Revision received June 2, 2023.
- Revision received September 7, 2023.
- Revision received September 30, 2023.
- Accepted for publication October 9, 2023.




{kind=link}