
Article Figures & Data
Figures
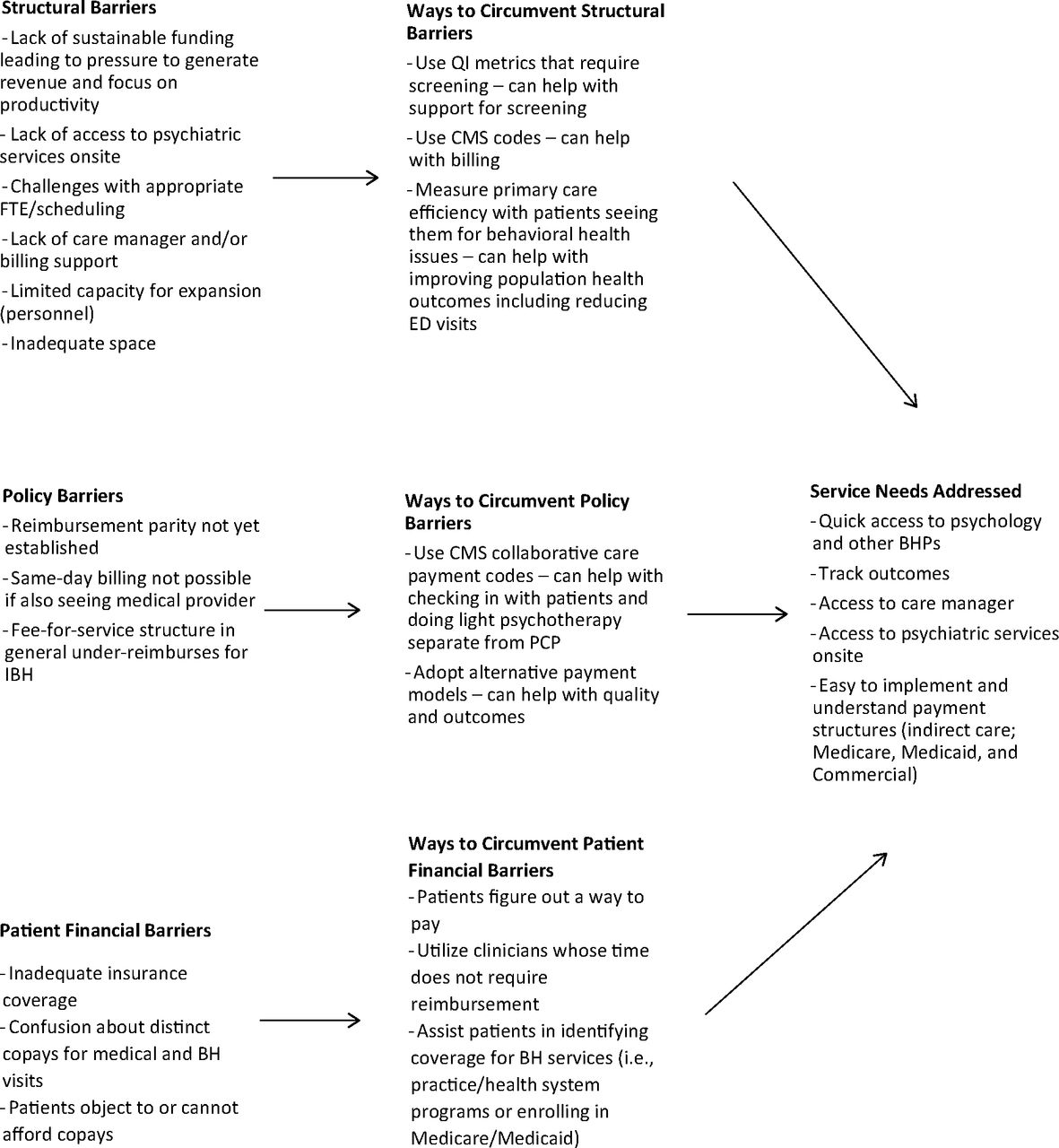
- Figure 1.
Structural and policy barriers to IBH in residency programs and potential ways to serve needs. Abbreviations: IBH, integrated behavioral health; FTE, full-time equivalent; QI, quality Improvement; CMS, centers for medicare & medicaid services; ED, emergency department; PCP, primary care physicians.

Tables

Category Exemplary Quotations Delivery of IBH Screening “Each patient who comes in for a visit gets a PHQ-2. If they screen positive on the PHQ-2, they get the PHQ-9 and the GAD-7. The medical assistants also [ask] questions of safety … Those are the baseline screeners that everybody who walks in the door gets.” Tracking “As far as ACEs [Adverse Childhood Experiences] and depression, there’s the ability to look at depression screening over time. [It] is to the individual patient, not something that’s population-based at this time.” Treatment Decision- Making Algorithms “No. It’s very provider dependent. We work at a residency practice, so I try to talk about the STAR*D trial [a National Institute of Mental Health funded study on depression treatment], but we have nine full faculty here, so our residents may get a different take on how to augment treatment.” Communication and Information Sharing “I'm now program director for our residency. Half of my clinical time is spent precepting residents. So when I precept residents, … I'm there with our board-certified psychologist precepting, and whether she's in and out seeing her own panel patients, or she's there dedicated to the precepting for the residents, she’s right there … [She] really participates in the conversation and the precepting for the care of all the resident patients for that session, and if there's direct behavioral health needs, she will take it away and handle the precepting. And if there are other medical needs, she'll still participate. [She’ll] give her feedback about other areas that the resident and the attending may not have considered. It's a great resource to have, and [she] also stays consistently engaged and involved. For the majority of patients, there's something that she can help with.” Providing Therapy in Clinic “I would like to see… options for patients to have the short-term intervention provider, as well as more of a specialty long-term option here. I think we lose a lot of people when we try to transition to community providers … ” Perspectives on IBH Benefits and Essential Elements for Successful Delivery “Definitely having a provider for the warm handoffs while we’re in clinic, but also having capacity or capability for the individual or group therapy sessions would be I think ideal. Also, having … an advanced care provider under a psychiatrist or a psychiatrist assist more with complicated medication management. A tough one for us. . . is to have easy and regular access to a psychiatrist for assistance with prescriptions.” “I mean, obviously, staffing would be remarkably helpful. What I would add is the billing support and that process. I would add the tracking piece through the EHR, which would be much less difficult to find. It'd be much more user friendly. Probably a new EHR completely would be needed to facilitate [efficient IBH delivery].” Destigmatizing Behavioral Health and Providing Holistic Care “Oh, man. After doing this job, I can’t imagine doing it any other way. I feel like for the patients, having access to mental health services where they see their provider, I think, takes away a lot of barriers to them actually following through [in getting care and treatment]. There’s just a level of comfort with coming to the doctor. It’s socially appropriate and acceptable to go to your doctor’s office. [Others] don’t need to know you’re coming to see your therapist versus the doctor or the dietician or whoever you’re coming to see. I think there’s just this natural level of acceptance to go and get your mental healthcare. Then being part of a multidisciplinary team, I feel like, [it] allows us to really make sure that our patients are being well cared for with all of their needs.” Benefits of Behavioral Health Services in Clinic Keeps Behavioral Health Services in Clinic “ … our patients have a lot of trauma and a lot of psychiatric needs. There's extremely poor access for psychiatric prescribing and also for mental health therapy services where we practice. It's really hard to get patients into an outside therapy or prescribing situation, unless they have the financial means. Where I practice, it's really diverse. We have a spectrum of socioeconomic diversity, but we really care for patients who are very underserved. [There’s] a lot of spillover from federally qualified health centers for people who don't have $150 to spend on a private therapy session. For a lot of our patients, given their comorbid addiction or trauma and mental health issues, having someone onsite who can do interventions and do some brief therapy and counseling and even prescribing is really crucial to them.” Managing Serious Mental Illness and Crisis “If they’re seeing a patient who has active suicidal ideation… or severe mental illness, let’s say, either in the clinic or on a telemedicine visit, we have an on-call warm handoff schedule. The provider can go and contact [the BHP], whether in clinic or via remote means, and then, after a brief consultation, can connect [the BHP] with the patient who can then take over while the provider continues their clinic day. And then, [the provider and BHP] connect again afterwards …[to] plan for further management.” “On the rare occasion that we have somebody who maybe is presenting with a … new onset severe mental illness or an acute flair up that needs a psychiatrist to help weigh in, often we can handle that within our clinic. We have a psychiatrist who oversees residents who are there once a month, and they assess the patient. They don’t actually prescribe to the patient. They tell the PCP what to do and work collaboratively with the PCP.” Potential Cost Reduction “If you're thinking about cost savings, we know that having integrated care or having a psychologist, social worker, or somebody who's actually doing therapeutic modalities is going to help reduce the burden on your primary care providers. It's going to save the system some costs in reducing visits to the emergency room. If you can coach somebody on how to manage their panic attacks, then they're probably going to visit the ED less, which saves the whole system money.” Learning to Collaborate and Instilling an IBH Culture “… it’s a great benefit for the community for one thing, but because our [psychiatry] resources are fairly limited in our area … trying to get a patient into a psychiatrist, even trying to get psychiatry in the hospital, is difficult. Having [psychiatry services] available for the community is huge. We have a lot of mental health issues in our area, but it’s also great for learners… Our behavioral med fellows do their own therapy sessions, and our residents actually rotate with them to see what they do, what they’re talking about, what they’re discussing, what they’re counseling [patients] on … [Residents] do a lot of behavioral med didactics, readings, and discussions [with them]. And then, having the extra [behavioral health practice opportunities] like the lifestyle clinic and the ADHD clinic for kids, also provides a whole other learning perspective for the resident that they’re not going to get elsewhere. When they’re an attending, if they’re in an office [without BHP access], at least they have had the education, and they have the base to move on with.” Structural and Policy Barriers to Successful Delivery “For us, it would probably be more like insurance coverage, co-pays. So if a lot of people don’t want top pay co-pays, they feel like they’re paying for their medical visit. Why would they have to pay for their mental health visit? That’s also a little bit of a sticking point with having them at your office. They feel like, well, if I’m here at the office, why am I paying twice? Even though it’s two different people seeing them for two different reasons and two very different visits, patients don’t always understand why they would be paying for different services in the same building.” “Space as well. I really required at least a private office to be able to meet with people. I do meet in exam rooms too, but even that can sometimes be difficult because the medical providers need that space often. I do some groups, and so sometimes in order to do groups, I need some larger … meeting spaces. So that's definitely been something to balance and juggle.” “I am fortunate enough to be employed by an institution. So for me, the financial cost is rolled into my budget and not so much my own cost. I was in private practice before I went into academics. In private practice, I don’t think there would be any way I could have afforded to be able to have a behavioral medicine side …It does cost money [laughter].” Abbreviations: IBH, integrated behavioral health; PHQ-2, patient health questionnaire-2; EHR, electronic health record; BHP, behavioral health professional; ED, emergency department; ADHD, attention-deficit/hyperactivity disorder.
Learner Type Role and Collaboration Description Residents Involved care team/BHP in behavioral health change interventions (e.g., smoking cessation, weight loss management, etc.).
Used counseling techniques, listening skills, and motivational interviewing (MI); and observed cognitive behavioral therapy (CBT) in patient care.
Learned when and how to incorporate care team/BHP in providing care.
Received targeted training for integration of BHPs and identification of processes (who needs help, how to reach out for assistance, and understand patient treatment needs).
Exposed to other experiences beyond traditional primary care clinic, e.g., addiction treatment centers, lifestyle clinics (i.e., chronic disease management), ADHD clinics, and resident-run clinics (i.e., non-emergency and preventative care).
Psychology Fellows Conducted own therapy sessions.
Participated in huddles, warm handoffs, curbside consults, etc.
Saw both resident and non-resident patients, communicated via a HIPAA compliant app or EHR, and made recommendations.
Participated in warm handoffs and consults.
Psychology/Counseling Interns Provided observation and direct care services under BHP supervision.
Performed individual or group counseling.
Supported case management.
Helped with referral process for more complex care for patients.
Followed up with patients by calling and touching base with them.
Helped with care coordination.
Participated in warm handoffs and brief consults.
Medical Students Observed in clinic.
Shadowed licensed professionals.
Conducted patient interviews.
Worked with residents in clinics.
Performed workup/intake.
Participated in group sessions (e.g., pregnant women and medication-assisted treatment).
Dedicated time with behavioral health and psychiatry team (if applicable) during rotations.
Exposed to caring for patients on a panel within a multidisciplinary team approach.
Pharmacy Students Helped with psychopharmacological questions.
Located in precepting room where they overheard behavioral health input.
Abbreviations: BHP, behavioral health professional; ADHD, attention-deficit/hyperactivity disorder; EHR, electronic health record; HIPAA, health insurance portability and accountability act of 1996.

In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.