
Abstract
Background: Non-prescription antibiotic use includes taking an antibiotic without medical guidance (e.g., leftovers, from friends/relatives, or purchased without a prescription). Non-prescription use contributes to antimicrobial resistance, adverse drug reactions, interactions, superinfection, and microbiome imbalance. Qualitative studies exploring perspectives regarding non-prescription use among Hispanic patients are lacking. We used the Kilbourne Framework for Advancing Health Disparities Research to identify factors influencing patients’ non-prescription use and organize our findings.
Methods: Our study includes Hispanic primary care clinic patients with different types of health insurance coverage in the Houston metroplex who endorsed non-prescription use in a previous survey. Semistructured interviews explored the factors promoting non-prescription use in Hispanic adults. Interviews were conducted remotely, in English or Spanish, between May 2020 and October 2021. Inductive coding and thematic analysis identified motives for non-prescription use.
Results: Participants (n = 35) were primarily female (68.6%) and aged 27 to 66. Participants reported obtaining antibiotics through trusted persons, sold under-the-counter in US markets, and purchased without a prescription abroad. Factors contributing to non-prescription use included beliefs that the doctor visit was unnecessary, limited access to healthcare (due to insurance constraints, costs, and clinic wait times), and communication difficulties (e.g., language barriers with clinicians and perceived staff rudeness). Participants expressed confidence in medical recommendations from pharmacists and trusted community members.
Conclusions: Patient, healthcare system, and clinical encounter factors contribute to non-prescription use in Hispanic communities. Antibiotic stewardship interventions that involve pharmacists and trusted persons, improve access to care, and address communication barriers and cultural competency in the clinic may help reduce non-prescription use in these communities.
- Access to Health Care
- Antibacterial Drug Resistance
- Antimicrobial Stewardship
- Behavioral Science
- Community-based Research
- Culturally Sensitive Research
- Family Medicine
- Health Behavior
- Health Care Seeking Strategies of Patients
- Health Communication
- Health Disparities
- Health Literacy
- Hispanics
- Minority Health
- Patient-Oriented Research
- Primary Health Care
- Public Health
- Qualitative Research
Introduction
Non-prescription antibiotic use (non-prescription use) is the use of antibiotics without a prescription obtained from another person, a leftover from a previously prescribed course, or purchased in a flea market or store in the United States (US) or abroad.1 Non-prescription use is a safety threat to individuals and global health. At the individual level, it can lead to taking unnecessary or inappropriate antibiotics that increase the risks of adverse drug reactions or interactions, superinfection, and disruption of the microbiome.2,3 At the global health level, non-prescription use can promote the development of antimicrobial resistance (AMR).4,5
Non-prescription use is prevalent in all World Health Organization regions, including Europe.6⇓–8 In the US, studies have identified certain population groups that use non-prescription antibiotics, including patients or patient parents/caregivers outside healthcare settings, patients or patient parents/caregivers within healthcare settings, Hispanic populations, and injection drug users.1 The highest prevalence rates in the US have been reported in Hispanic communities, ranging from 19% to 66% compared with other groups (1% to 48%).1,9⇓⇓–12 Therefore, it is critical to understand the factors contributing to this unsafe practice in Hispanic populations.
A few qualitative studies have examined the factors influencing non-prescription use in Hispanic communities in the US.11,13⇓–15 These studies focused on predominantly Spanish-speaking migrant individuals with low income and education.11,13⇓–15 In some studies, a lack of health insurance, access to a primary care provider, monetary constraints, and long clinic waiting periods were among the barriers to a doctor’s appointment.11,13,14 Most of these studies focused on Hispanic migrant populations with no healthcare coverage and who face extremely constrained financial situations that make doctor’s visits and receiving prescription antibiotics very challenging. We recruited a socioeconomically and linguistically diverse sample of Hispanic patients to explore factors contributing to non-prescription use. Despite our study participants being patients with healthcare coverage from Medicare/private insurance or unique payer sources (Medicaid or county financial assistance program), all reported using antibiotics without a prescription, triggering the question, Why do patients with seeming healthcare access use antibiotics without a prescription?
Our study seeks to identify the situations, reasons, and motivations influencing Hispanic patients’ non-prescription use. We chose the Kilbourne Theoretical Framework for Advancing Health Disparities Research16 because it detects the multidimensional factors across the patient, healthcare system, and clinical encounter underlying health disparities. We used this framework to organize cross-cutting themes surrounding non-prescription antibiotic use in a Hispanic patient primary care population.
Methods
Participants
This qualitative study includes self-identified Hispanic adults living in Harris County, Texas, who endorsed using non-prescription antibiotics in a larger quantitative survey (i.e., answered yes to the question In general, would you use antibiotics without contacting a doctor/nurse/dentist/clinic?).17 Patients were recruited from 5 public clinics (2 same-day and 3 continuity) serving low-income Houston residents and 1 private emergency department (ED).
Ethical Consideration
This study was approved by the Institutional Review Board for Baylor College of Medicine and Affiliated Hospitals (protocol H-45709).
Data Collection
Recruitment of Participants
This study was part of the second phase of a mixed methods research project.17 The first phase included a large quantitative survey and the second phase included in-depth qualitative interviews with users of non-prescription antibiotics. We used purposive sampling18 to recruit participants who reported using non-prescription antibiotics from a previous survey published elsewhere.17 The previous survey queried participants on their demographics, overall health status,19 and health literacy.20,21 See Appendix 1 for detailed description of these variables. On completing the previous survey, participants who identified as non-prescription users were invited to participate in a follow-up semistructured interview.
Qualitative Interviews
The interview guide was pretested with educationally diverse individuals and revised for reading level, clarity, and cultural appropriateness (see Appendix 2 for Interview Guide). All interviews were conducted remotely via a teleconferencing platform and audio recorded between May 2020 and October 2021 by 2 trained bilingual research assistants (OA and JS). Interviews were conducted in English or Spanish, according to language preference. All interviews were transcribed using local transcription companies. The bilingual research assistants translated Spanish transcripts into English for analysis and coding.
Interviews were semistructured and designed to explore the factors and situations that promote non-prescription use. Interviews captured elements from the Kilbourne theoretical framework, including patient attitudes and beliefs, resources, and various health-system factors that could impact non-prescription use.
Analysis
Qualitative coding occurred from June to December 2021 using a team-based approach with 5 qualitative analysts (LL, PC, OA, JS, KO). Coding and transcript management was conducted using ATLAS.ti Web (Version 22.1.5.0),22 allowing synchronous coding in real time and for analysts to view others' transcripts and make changes as needed. An inductive coding approach was utilized, drawing from interview participants' words to create code names and allowing themes to emerge naturally.23 The researchers used constant and iterative comparison techniques to associate information across transcripts, grouping similar codes together to create a codebook.24 To understand patterns among Hispanic participants, LL conducted a focused analysis to explore how, when, and why patients would endorse non-prescription use.
Results
Participant Characteristics
Table 1 shows the sociodemographic characteristics of Spanish- (n = 21) and English-speaking (n = 14) Hispanic participants interviewed. Of the 63 Hispanic participants that qualified for an individual scheduled interview, 47 agreed to participate. Of these, 35 completed the interview (response rate 74.5%). All 35 participants, were similar in age, gender, and insurance status. Most participants (71.4%) were high school graduates or above. More than half (54.3%) of participants reported household incomes below $20,000/y. Most participants (71.4%) were born outside the US, with a median of 25 years lived in the US. On average, participants rated their overall health status as “fair” (median = 4). Overall, 31.4% of participants had inadequate health literacy.
Sociodemographic Characteristics of Participants
Thematic Analysis
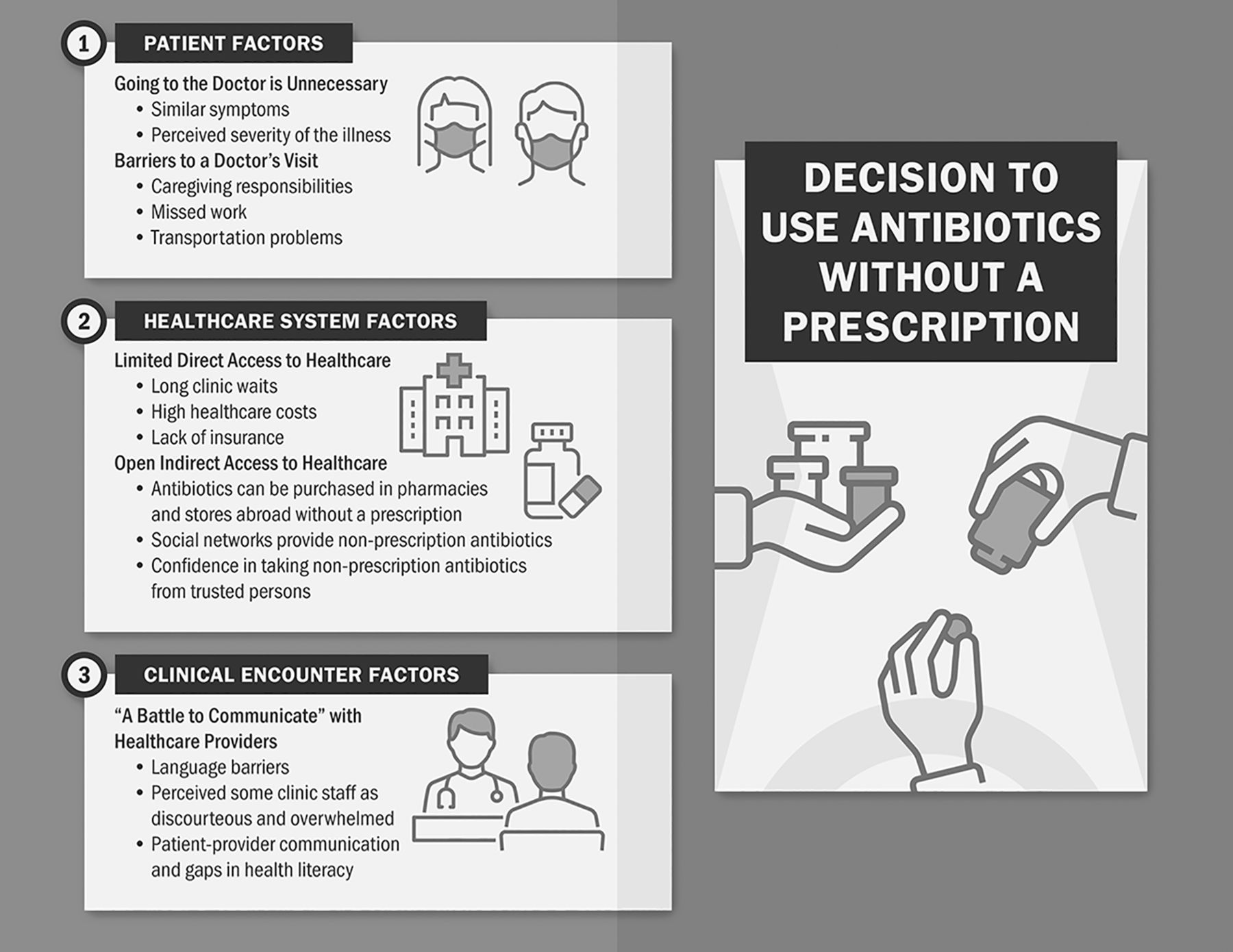
We organize our qualitative findings to align with the Kilbourne theoretical framework domains: patient, healthcare system, and clinical encounter (Figure 1). For each domain, salient themes emerged from the qualitative analysis shedding light on the reasons and motives why participants would consider using non-prescription antibiotics, illuminating the complexity of this unsafe practice in Hispanic communities. Appendix 3 depicts a frequency table for each theme and subtheme mentioned.

Overview of themes and subthemes across the patient, healthcare system, and clinical encounter domains that influence Hispanic patients' decisions to use antibiotics without a prescription.
Domain 1: Patient Factors
At the patient level, participants discussed their knowledge, attitudes, beliefs, and practices concerning non-prescription use.
Theme 1: Patients Consider Going to the Doctor as an Unnecessary Step
Many participants felt that going to the doctor to receive a prescription for their antibiotics was unnecessary and that they already knew how to treat their health problems. Patients felt they already knew when and how to take non-prescription antibiotics, often because they were alleviating symptoms similar to those of a prior illness (treated with antibiotics) or reducing illness severity. For instance, one participant said, “If you know that you are sick and you have got those particular symptoms…and you know that [leftover] antibiotics will help you. You might as well take them” (P14-Male-English). Another participant stated that she would consider using a leftover antibiotic “if it is the same symptoms…and the appointment is 5 weeks away, I would take the antibiotic” (P8-Female-English). Others believed that the antibiotics would reduce the symptoms severity: “I can take these [non-prescription antibiotics], and maybe [the symptom] will go away. I think it helped. The pain lessened and everything. That is why I took them” (P8-Female-Spanish).
Participants often drew on practices handed down from trusted family members, obviating the need for professional medical advice: “I think it is fine because…my mom did not give us…cold medicine…she gave us penicillin for the cold, and it went away” (P17-Female-Spanish). One participant believed antibiotics “worked better” than over-the-counter medicines, and therefore preferred to take a nonprescribed antibiotic instead of taking cold medicines or going to the doctor: “I usually take them when I feel like I am going to get a cold… I'd rather take antibiotics than Tylenol and stuff like that” (P11-Male-English).
In addition, the sense that these participants were “their own best doctor” was coupled with the logistic difficulties of going and seeing a doctor, making a doctor’s prescription for antibiotics even less desirable to participants: “[I do not want to] waste time going to the doctor…[or] make an appointment” (P1-Female-Spanish). Another participant said, “If it is something that I've had before… I am not going to go to the doctor…it is too much of a hassle”…“If I have an antibiotic [leftover], I will take it and be done with it” (P14-Male-English).
Theme 2: Barriers to a Doctor’s Visit
Participants also acknowledged barriers to a doctor visit, including caregiving or work commitments and lack of transportation. For instance, 1 participant states that childcare made going to the doctor’s appointment inconvenient, “I do have 2 little kids. It is quite difficult…it is an inconvenience because I would have to pay someone to watch them” (P18-Female-Spanish). Others feared losing work or being fired from a job, “I do not want to go to the doctor [because] I’ve got to lose work” (P11-Male-English) or “I have friends who have been laid off or fired because they kept taking time off to go help family members [with doctors’ appointments]” (P12-Male-English). Lacking transportation also hindered patient access to the doctor, “We only have 1 car…and my husband usually goes to work in it, so, I have to look to the option of a Metro. It can be a challenge” (P21-Female-Spanish).
Domain 2: HealthCare System Factors
Barriers within the healthcare system also influenced decisions to take non-prescription antibiotics. Many patients described how they experience limited access to healthcare in the US yet obtain nonprescribed antibiotics through informal networks, in their home countries, or across the border, in Mexico.
Theme 2A: Limited (Direct) Access in the US
Patients described several barriers to receiving formal healthcare in the US, such as long clinic wait times, high costs associated with doctor visits and medications, and lack of insurance. Participants described how “it is very time-consuming and very stressful to be waiting” at the clinic and that sometimes the appointments are too far away, encouraging non-prescription use, “If I make an appointment, the first available will be in a month…I can take these [leftover antibiotics], and maybe it will go away” (P8-Female-Spanish).
The high cost burden of going to the doctor and purchasing prescription medications further drove the use of non-prescription antibiotics, as patients felt they had no other choice: “I've been in a situation where there is no money…no resources. There is no way” (P12-Male-English). Another participant recounted, “People do things depending on their situation…let us be real, antibiotics are expensive” (P8-Female-English). For some participants, the knowledge that antibiotics across the border were much more affordable underscored the high cost burden of drugs in the US: “Here, I pay $50 for [antibiotics], and over there [Mexico], I pay $5” (P12-Male-English).
Finally, participants lacking insurance found the doctor’s visit too costly and directly linked their lack of insurance to the use of non-prescription antibiotics: “I did not have health insurance…It would be much more expensive for me to go to a doctor than to buy them [elsewhere] at that time” (P18-Female-Spanish). One participant reflected on how a lack of health insurance contributed to non-prescription antibiotic use among his friends and family, “I have used antibiotics here [US] prescribed by my doctor, but I have health insurance. That is the key; I have health insurance…some [family and friends] still do [take non-prescription antibiotics from Mexico] because [of a] lack of healthcare [because] it is so expensive here [US]” (P12-Male-English).
A lack of access to healthcare forces patients to rely on indirect means to survive. As 1 participant reflected, “When there is no access to medicines…to money, to a doctor, to all those things like that…then yes… you survive with the medicine that is not prescribed” (P12-Male-Spanish).
Theme 2B: Open (Indirect) Access
In contrast to the difficulties of receiving and affording healthcare in the US, patients described the ease of obtaining non-prescription antibiotics in pharmacies abroad and through informal social networks in the US, including friends and relatives, markets or yerberias (i.e., herbalist shops), or purchasing from individuals that were perceived as trustworthy. One participant described a 1-stop system for purchasing antibiotics in a Mexican pharmacy:
“I remember…I got sick, and [family] told me, 'Oh, go to the pharmacy and ask for this'… I [went to] the pharmacist and [told] him my symptoms. The pharmacist [said], 'Oh, [you need] an ampicillin'… [The pharmacist] prescribed it for me” (P9-Female-Spanish).
Another explained: “In Mexico…we self-medicate. No, you do not need to go to the doctor that much. You just go to the pharmacy…and they sell [nonprescribed antibiotics] to you very easily.” He expressed frustration with the differences between the US medical system’s prescribing of antibiotics and Mexico, “[It] is not the same here [in the US] because you have to go to the hospital…[and] they do not give [you] [antibiotics]…, only Tylenol” (P6-Male-Spanish). Moreover, many Hispanics found it normative to consult the pharmacist and to purchase antibiotics without a prescription, “We have always used [non-prescription antibiotics] in my country…you do not need a prescription…[to] buy…ampicillin, tetracycline, those antibiotics” (P5-Male-Spanish).
In addition, patients described US-based, informal networks where they could obtain non-prescription antibiotics. This network included friends and family, as well as yerberia staff. As a source for antibiotics, many participants considered these networks their first choice over US medical doctors: “I went to the pharmacy first, then the woman [yerberia], then…2 to 3 weeks [later], I went to the doctor” (P10-Female-Spanish). Others said their social networks help them procure non-prescription antibiotics, including injectables. For instance, “My family members and friends…don't go to the doctor here…they go to Mexico and bring [back] antibiotics, such as amoxicillin…Sometimes they bring [back] penicillin, and then they find somebody up here [US] to give them a shot” (P12-Male-English).
Others expressed confidence in antibiotic recommendations from other individuals that appeared acceptable—“the person that recommended [the antibiotic to me] looked good and fine”(P13-Female-English)—especially if the non-prescription antibiotic purchased is a “known antibiotic” (P21-Female-Spanish) or “the same drug [in the US but bought] in Mexico” (P8-Female-Spanish).
Domain 3: Clinical Encounter Factors
Theme 3: “a Battle to Communicate” with Healthcare Providers
Participants felt that communication difficulties, including language barriers, impeded their ability to communicate and receive proper healthcare. One participant revealed, “It is a battle to try to communicate with the doctor…but you have to make an effort because of the pain or discomfort that you have. [Because of this], you say to yourself, ‘Let’s see if this [non-prescribed antibiotic will] work well for me’” (P14-Male-Spanish).
Another participant reflected on his experience translating for his parent so she could receive the proper diagnosis and care. “I used to translate for my stepmom, and [she] would get so embarrassed that I had to ask to translate for her…she didn’t know how to talk to the doctor because she didn’t know English… that is the only way she would get treated and get her right medicine” (P12-Male-English).
Some Spanish-speaking participants perceived some clinic staff as discourteous and implied that some nurses seemed overwhelmed or overburdened. For instance, 1 participant stated, “It makes me very upset because of the way certain people treat you…they are rude. They speak to you very harshly” (P14-Male-Spanish). Another expressed, “The nurses have an attitude. They are frustrated…and they are mad. They are having a bad day” (P5-Female-English). These negative experiences made patients less inclined to visit a doctor for their problems.
In addition, disconnects in patient-provider communication and health literacy gaps prevented patients from understanding their illnesses and the reasons for their prescriptions (or lack of). For instance, 1 Spanish-speaking participant stated, “I’ve been told a few times, ‘[You can take] an ibuprofen [or]…Theraflu. You don’t need [antibiotics] to alleviate your common cold.’ To [clinicians], it is a cold…but to me, it is an infection. I never understood the system in this country” (P9-Female-Spanish).
Discussion
Using the Kilbourne Theoretical Framework for Advancing Health Disparities Research, we explored the pathways influencing non-prescription use in Hispanic communities. At the patient level, we found that many participants endorsed non-prescription antibiotics to self-medicate (e.g., similar symptoms to when an antibiotic was used to treat previously, and if the illness was perceived to be “very bad” or severe) or to avoid the barriers and inconvenience of going to a medical professional. At the healthcare system level, we uncovered the countervailing healthcare access for our Hispanic participants. Lack of insurance, high healthcare costs, and long wait times (to get an appointment or to see a clinician) created limited access to prescription antibiotics for our participants. At the same time, patients found more open access to antibiotics through pharmacies or stores in foreign countries and their social networks. Patients reported using non-prescription antibiotics purchased abroad because they are more readily available and inexpensive compared with the US. Participants will purchase the nonprescribed antibiotics and then bring them back to the US (e.g., for themselves, give to others, or sell). At the clinical encounter level, participants reported frustrations with the clinic visit primarily due to communication difficulties and discourteous staff. Participants elaborated on their challenges in translating guidance due to language barriers and problems understanding specific diagnoses, often stemming from gaps in knowledge and health literacy.
Our results corroborate the findings of other US studies on patient and healthcare system level factors. Our findings confirm that the motives and experiences that drive non-prescription use include using non-prescribed antibiotics to alleviate symptoms,11,13,15,25 reduce the severity of an illness, avoid unnecessary clinic visits, reduce the financial burden, or bypass insurance barriers.25 The preference for medicines and antibiotics from abroad13 compared with medications in the US, along with the convenience of taking leftover prescriptions or purchasing nonprescribed antibiotics under the counter, promotes non-prescription use in Hispanic communities.14,15,25 For instance, Sanchez11 found that participants engaging in non-prescription use in their home countries often increased their use when they moved to the US. Essignmann and colleagues25 revealed that despite the 2010 changes to prescription drug regulations in Mexico, uninsured Hispanics in the US still commonly traveled to acquire non-prescription antibiotics. Similarly, our study participants highlight these situations and practices that can subvert community-based antibiotic stewardship efforts.
Our findings highlight the healthcare system and clinical encounter factors that complement previous literature. Previous studies have focused on primarily Spanish-speaking immigrant populations, uninsured, and socioeconomically disadvantaged Hispanics or Latino(a)s in the US.11,14,15,25 Compared with other studies with primarily uninsured or underinsured participants, the majority of our interviewees had some form of healthcare coverage (e.g., Medicare, Medicaid, or county financial assistance).11,15 In addition, the participants surveyed varied by income and educational attainment. Compared with other studies that capture mostly low-income, impoverished Hispanics with low educational attainment,11,15 our interviews included individuals of middle to high incomes, and the majority of the participants had higher educational attainment, including high school and college (or above) degrees.
Participants perceiving some clinical staff as rude or discourteous was an unanticipated finding. Other studies have found that Hispanics’ trust in US healthcare tapers when the doctor-patient relationship does not feel personal, welcoming, or show concern for the patient.26⇓–28 In a 2022 Pew Research Study,28 more than 50% of Hispanics reported they have had at least 1 of several negative experiences with healthcare providers at some point in their lives, including feeling rushed by clinicians, and feeling that they were treated with less respect compared with non-Hispanic patients. Unfortunately, these results were amplified in female Hispanic patients. Clinicians in the US healthcare setting can seem discourteous to some patient populations when clinicians and staff rush visits, speak tersely, or lack time to establish relationships with patients. Unfortunately, these communication difficulties may lead many Hispanic patients to distrust the clinical encounter and reinforce the perception that the clinician is not compassionate toward them.26⇓–28 Clinicians and clinic staff can benefit from cultural competency education and using more considerate and culturally appropriate strategies while interacting with patients.
Limitations of our study design include that the interview format may have introduced social desirability response bias, despite our best effort to keep questions phrased neutrally. Some participants may have answered questions dishonestly or suppressed opinions due to the topic's sensitivity. In addition, contextual changes driven by the US quarantine and COVID-19 pandemic may have impacted responses and increased inappropriate antibiotic use to treat or prevent COVID-19 symptoms.29 Our findings may not represent the perspectives of all Hispanic communities in the US, but they may apply to other US cities with large Hispanic populations with similar non-prescription use practices.
Our study has illuminated how healthcare access barriers and clinical encounter difficulties have encouraged non-prescription use among Hispanic patients. We gained important insights about whom our patients trust to provide antibiotics and healthcare recommendations, including community pharmacists and trusted community members (e.g., yerberia staff, relatives, friends, and others). Community health workers in Hispanic communities (i.e., promotoras)30⇓–32 and also local pharmacists33⇓–35 may be well situated to deliver components of antibiotic stewardship programs aimed at reducing non-prescription antibiotic use. Patient education about appropriate antibiotic use is critical to improve health knowledge and outcomes in Hispanic communities.36,37
In conclusion, a complex interplay between patient, healthcare system, and clinical encounter level factors contributes to non-prescription use among Hispanic communities. Designing antibiotic stewardship interventions that involve community pharmacists and health workers may help to reduce barriers to healthcare access and patient-provider communication, thus minimizing inappropriate antibiotic use, under-the-counter antibiotic acquisition, and antimicrobial resistance.
Acknowledgments
The authors thank the patients and the Harris Healthcare System staff, Osvaldo Alquicira, Juanita Salinas, Kiara Olmeda, and Fara Abordaje.
Appendices.
Appendix 1: Variable Descriptions

Appendix 2: Phase 2 Interview.

Appendix 3: Frequencies of Mention by Participants for Each Theme and Subtheme.
| Domain | Theme/Subtheme | Frequency of mentions |
|---|---|---|
| Patient factors | Caregiving responsibilities | 5 |
| Work commitments | 11 | |
| Lack of transportation | 28 | |
| Doctor visit is unnecessary | 27 | |
| Alleviating symptoms similar to those of a prior illness | 81 | |
| Reducing illness severity | 6 | |
| Healthcare system factors | Long clinic waits | 11 |
| High costs of the doctor (visit and medications) | 30 | |
| Lack of insurance | 12 | |
| Ease of obtaining non-prescription antibiotics in: | ||
| Informal social networks in the US, including friends/relatives | 35 | |
| Markets or yerberias | 10 | |
| Pharmacies abroad | 22 | |
| Purchasing from perceived trusted individuals | 50 | |
| Clinical encounter factors | Communication difficulties with healthcare providers | 13 |
| Language barriers | 4 | |
| Discourteous staff | 3 | |
| Disconnects in patient-provider communication | 4 | |
| Health literacy gaps | 2 |
Notes
This article was externally peer reviewed.
This is the Ahead of Print version of the article.
Funding: This research is supported by grant number R01HS026901 from the Agency for Healthcare Research and Quality (AHRQ) and the Ruth L. Kirschstein National Research Service Award (NRSA) T-32 (6T32HC10031). Barbara Trautner’s work was supported in part by the United States Department of Veterans’ Affairs, Health Services Research and Development Service (grant no. CIN 13-413) at the Center for Innovations in Quality, Effectiveness, and Safety. The contents presented herein do not represent the views of the U.S. Department of Veterans Affairs or the United States Government.
Conflict of interest: None.
To see this article online, please go to: http://jabfm.org/content/00/00/000.full.
- Received for publication December 8, 2022.
- Revision received February 5, 2023.
- Accepted for publication February 10, 2023.
References
In this issue




{kind=link}
Jump to section
- Article
- Abstract
- Introduction
- Methods
- Data Collection
- Analysis
- Results
- Domain 1: Patient Factors
- Domain 2: HealthCare System Factors
- Domain 3: Clinical Encounter Factors
- Discussion
- Acknowledgments
- Appendices.
- Appendix 2: Phase 2 Interview.
- Appendix 3: Frequencies of Mention by Participants for Each Theme and Subtheme.
- Notes
- References
- Figures & Data
- References
- Info & Metrics
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Keywords
- Access to Health Care
- Antibacterial Drug Resistance
- Antimicrobial Stewardship
- Behavioral Science
- Community-Based Research
- Culturally Sensitive Research
- Family Medicine
- Health Behavior
- Health Care Seeking Strategies of Patients
- Health Communication
- Health Disparities
- Health Literacy
- Hispanics
- Minority Health
- Patient-Oriented Research
- Primary Health Care
- Public Health
- Qualitative Research