
Abstract
Background: Limited studies are available on patients' perspectives regarding opioid-related awareness, beliefs, and pain management in primary care settings in the US. Pain catastrophizing (PC) is a cascade of negative thoughts and emotions in response to actual or anticipated pain. High PC is 1 of the strongest predictors of negative pain outcomes.
Method: A cross-sectional survey was administered at Family Medicine clinics in the Pacific Northwest, November 2018-January 2019. Logistic regression was used to model the adjusted odds of participants' awareness and beliefs on opioid epidemic issues, side effects/risks, and general beliefs by opioid prescription expectations and PC.
Results: 108 participants completed the survey. Compared with participants with low PC, high PC participants were 74% less likely to be aware of opioid epidemic issues (OR = 0.26, P = .005, 95% CI:0.10-0.67), 62% less likely to be aware of opioid side effects/risks (OR = 0.38 P = .040, 95% CI: 0.15-0.96) and had 2.4 times increased odds of holding more positive beliefs about opioids and/or stronger beliefs regarding pain control, yet the latter did not reach statistical significance (OR = 2.40 P = .083, 95% CI: 0.89-6.47).
Conclusion: Significant gaps existed among our participants with high PC in their awareness of opioid epidemic issues and side effects/risks compared with their low PC counterparts. They may also carry positive beliefs regarding opioids and pain-control in general. In any pain care, it seems important to identify patients with high pain catastrophizing. Doing so may facilitates exploration of their beliefs and expectations regarding pain management and aids in tailoring individualized treatment and prevent adverse side effects.
- Catastrophization
- Cross-Sectional Studies
- Family Medicine
- Logistic Regression
- Motivation
- Opioids
- Pain
- Patient Education
Introduction
As the US continues to cope with overdose deaths due to heroin, synthetic opioids, and prescription drugs,1 pain control for acute and chronic pain remains challenging.2 There is strong evidence recently that opioid therapy seems to be associated with decreased or similar effectiveness as NSAIDs for some acute conditions, and with increased adverse events.3 There has already been a significant decline in opioid prescribing over the past several years, partially from increased opioid prescribing regulations and rules.4,5 While there has been a dramatic decline in opioid prescribing in recent years due to increased policies and regulations,6 patients' perspectives regarding pain management have not been sufficiently explored.7 Literature has examined patients' perspectives and experiences regarding acute pain management in emergency departments and7,8 postoperative care,9⇓–11 as well as patients' perspectives and experiences on cancer pain12 and chronic pain.13,14 However, there are limited studies examining patients' perspectives, general awareness, and beliefs regarding opioids, their risks and side effects, and their use for pain management in outpatient clinic settings in the US.15 This setting is important to study as acute pain complaints are most often encountered by primary care practices,16 and primary care clinicians alone account for a third of opioid prescriptions in the US.17⇓–19
In our previously published study, we examined patients' expectations of receipt of an opioid prescription for acute pain control and patient characteristics associated with these expectations in an ambulatory clinic setting.20 The majority of patients indicated that they would expect an opioid prescription in at least 1 of 4 dispositional ambulatory acute pain setting scenarios. High pain catastrophizing was significantly associated with higher opioid expectations.20
Pain catastrophizing is described as a cascade of negative thoughts and emotions (helplessness, rumination, and magnification) in response to actual or anticipated pain,21⇓–23 occurring in up to 30% of chronic pain patients.22,24,25 In chronic pain patients, pain catastrophizing has been associated with opioid misuse26 and opioid craving,27 as well as increased pain intensity, especially in women.21 Furthermore, it can be predictive of delayed opioid cessation after surgery,28 acute postoperative pain, and chronic postsurgical pain.29⇓⇓⇓–33 Opioid use disorder and mental illness often co-occur,34 and opioid misuse26 and mental illness25 are often associated with pain catastrophizing. Dependence, depression, and worsening of underling mental illnesses are all known potential opioid side effects.35,36
In 2000, the Joint Commission introduced standards for addressing pain, using systematic quantitative assessments (eg, 11-point pain score).37 These standards led to an increase in opioid prescriptions in the US,5,37 likely resulting in patients expecting prescribed opioids for any type of pain.20 Outcomes of acute pain involving musculoskeletal pain may be influenced by patients' expectation of treatment, rather than the specific treatment itself.38,39 A systematic review of studies of patients with chronic pain revealed that health care clinicians' awareness of patient expectations is important and that for shared decision-making, physicians should discuss these expectations with patients.40 Assessing and exploring patients' pain treatment expectations should be an essential part of any pain management regimen.40,41
In this study, we explored how pain catastrophizing and opioid expectations in acute pain scenarios are associated with an individual's 1) awareness of the opioid epidemic, 2) awareness of opioid side effects and risks, and 3) general beliefs about opioids and pain control. Considering the complexity of pain catastrophizing and based on findings from our prior study,20 we hypothesize below that individuals with high pain catastrophizing, and those who expect more opioids, are 1) less likely to be aware of opioid epidemic issues, 2) less likely to be aware of opioid side effects and risks, and 3) more likely to hold positive beliefs regarding opioids and/or stronger beliefs regarding pain control. A better understanding of these relationships could foster the individualized education and management needed to reduce unnecessary opioid exposure, toward the goals of reducing opioid-abuse risks7,42 and improving pain care experiences.
Methods
Study Design and Settings
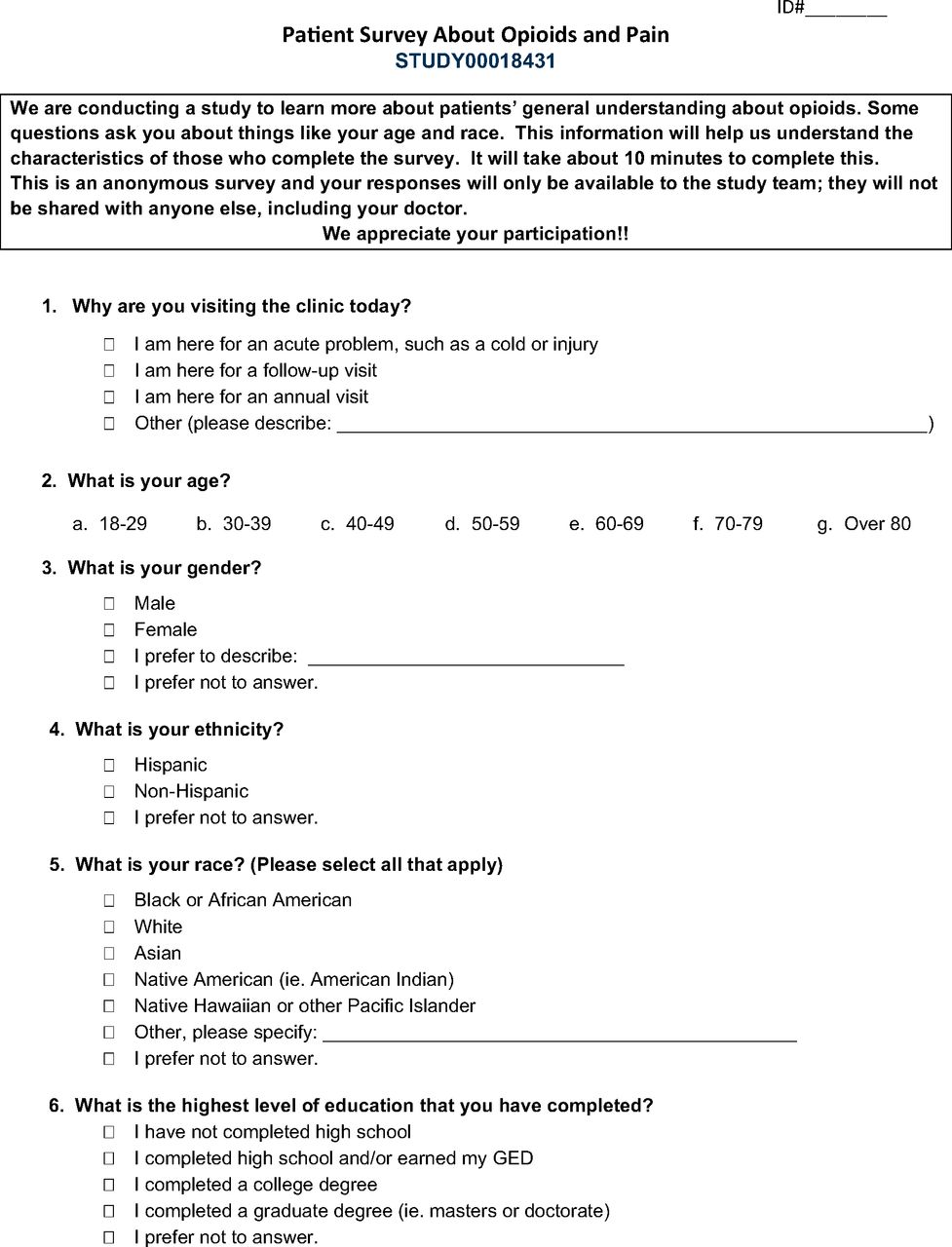
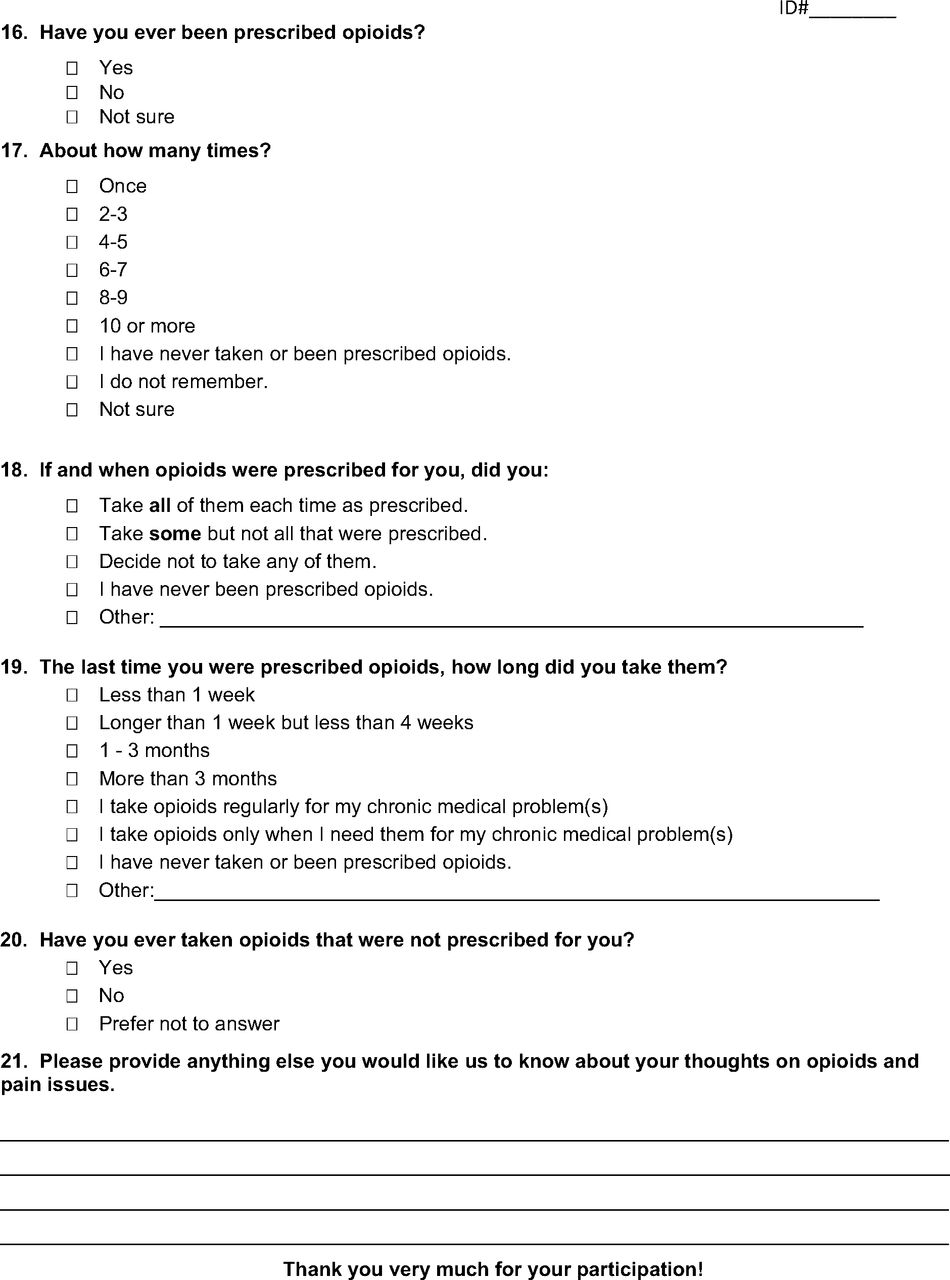
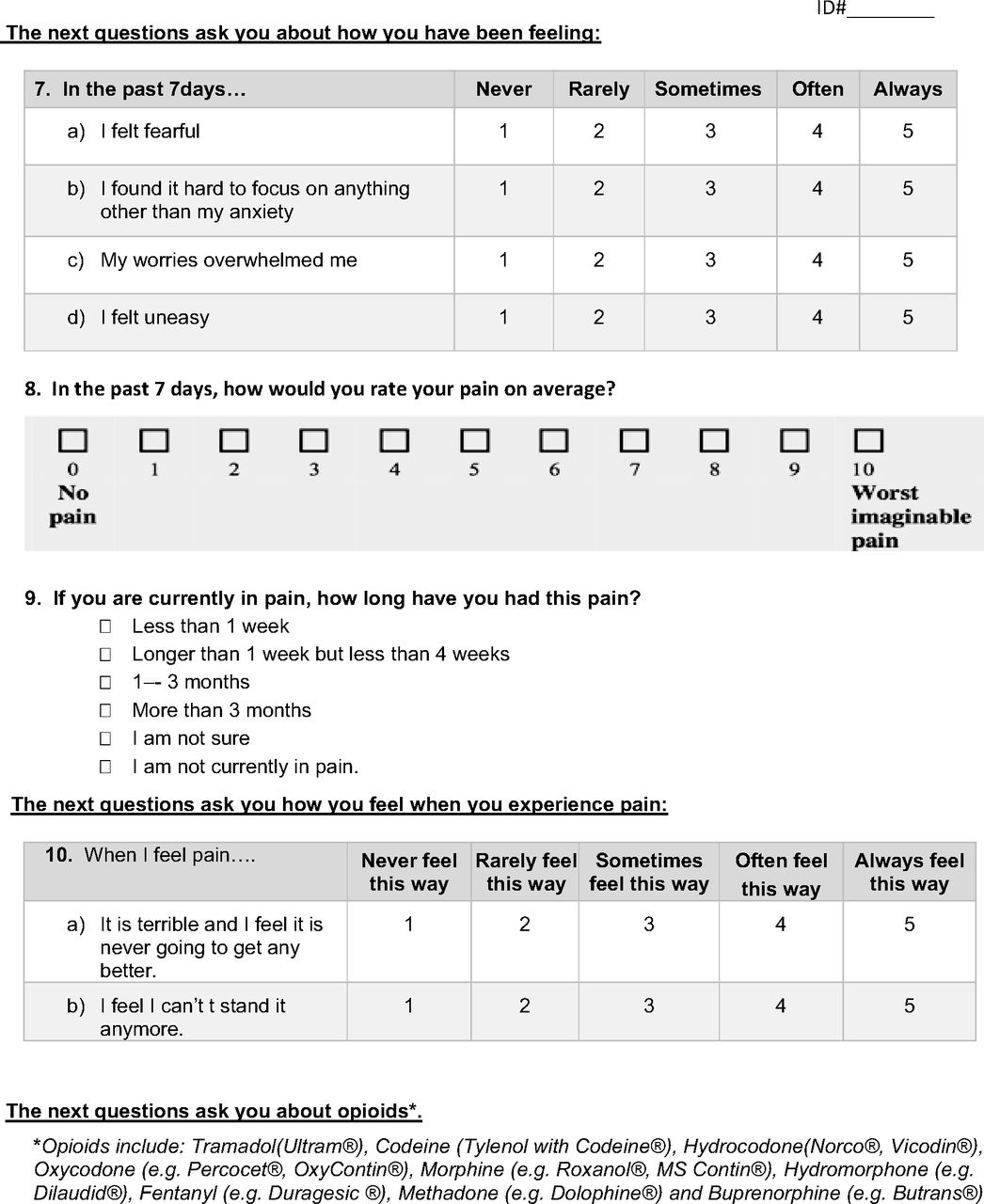
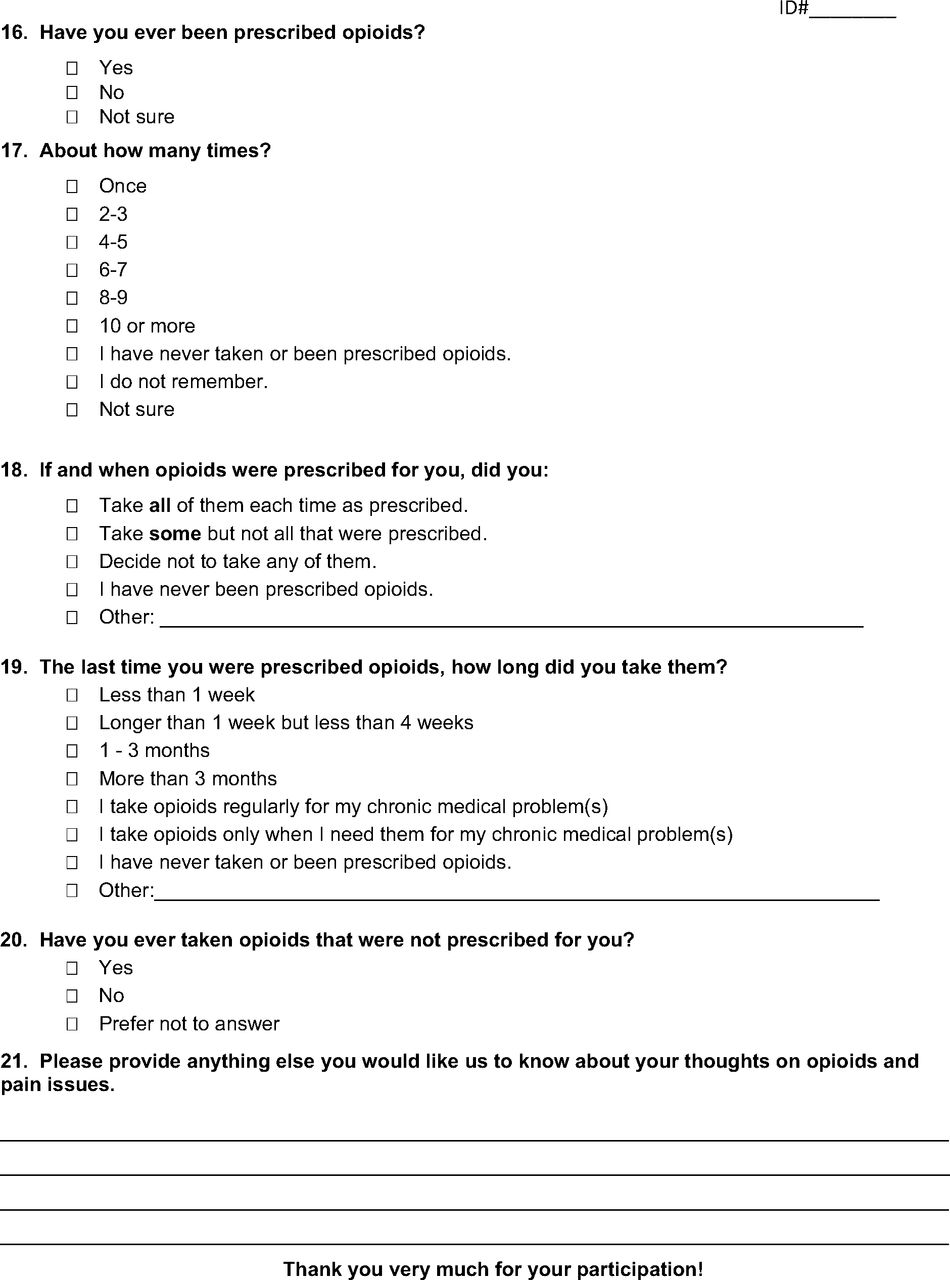
This cross-sectional study utilized a 1-time survey with a convenience sample of patients in clinic waiting rooms at 2 family medicine clinics in Portland, Oregon. After providing verbal consent, participants completed a 21-question written survey (Appendix). Details of the recruitment methods, inclusion criteria, and survey creation process can be referenced in the published article.20 Briefly, English-speaking adult patients were recruited in the study clinic waiting rooms during random visits by the principal investigator. A survey was created by the study team and piloted with 10 randomly recruited individuals (not necessarily patients) who were in the lobby of the health center where 1 of the study clinics was located. The final version of the survey was developed after verbal feedback was obtained and reviewed by the study team. The study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement for cross-sectional studies.43 This research was approved by the Institutional Review Board of the participating institution.
Outcomes
Opioid epidemic awareness:
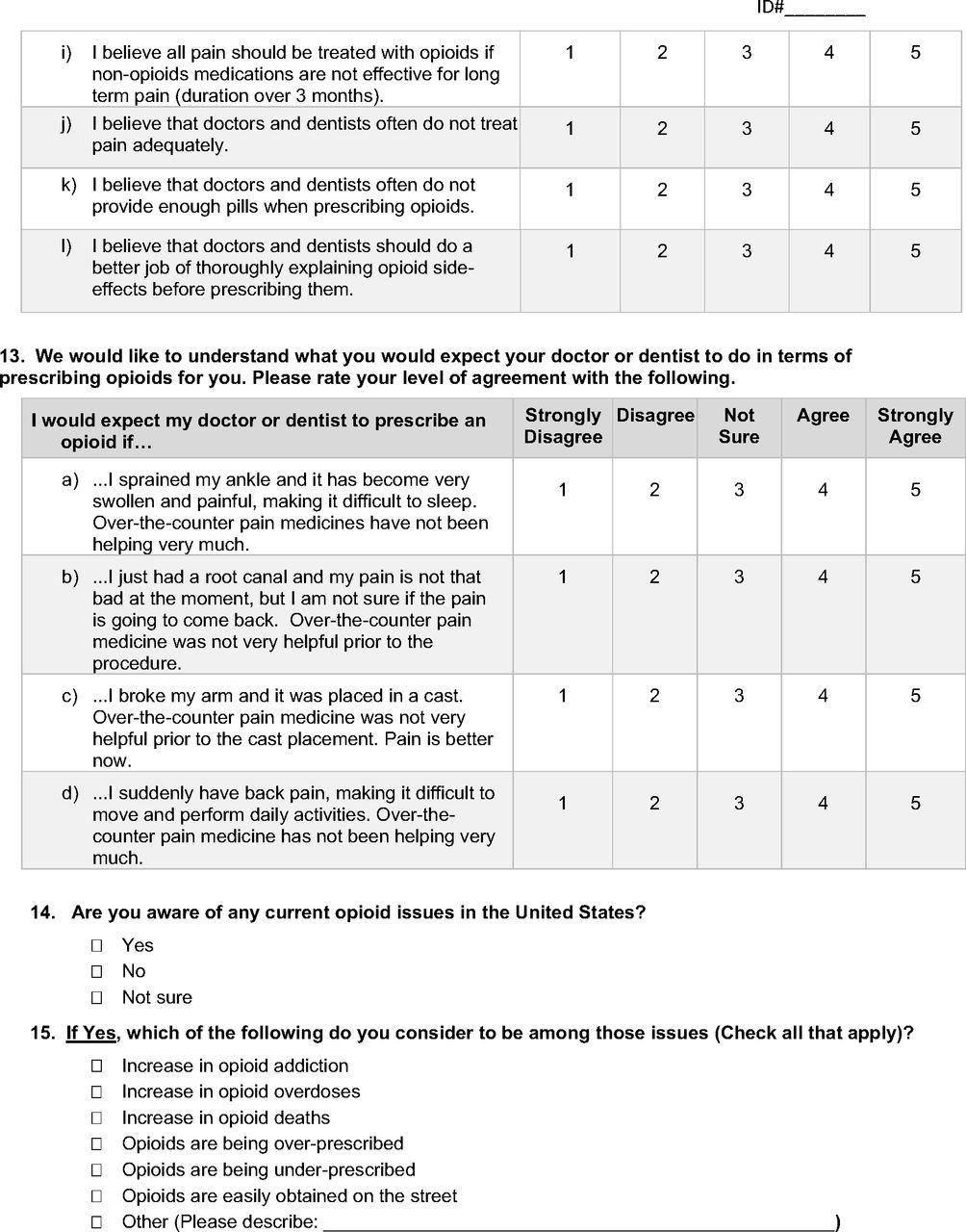
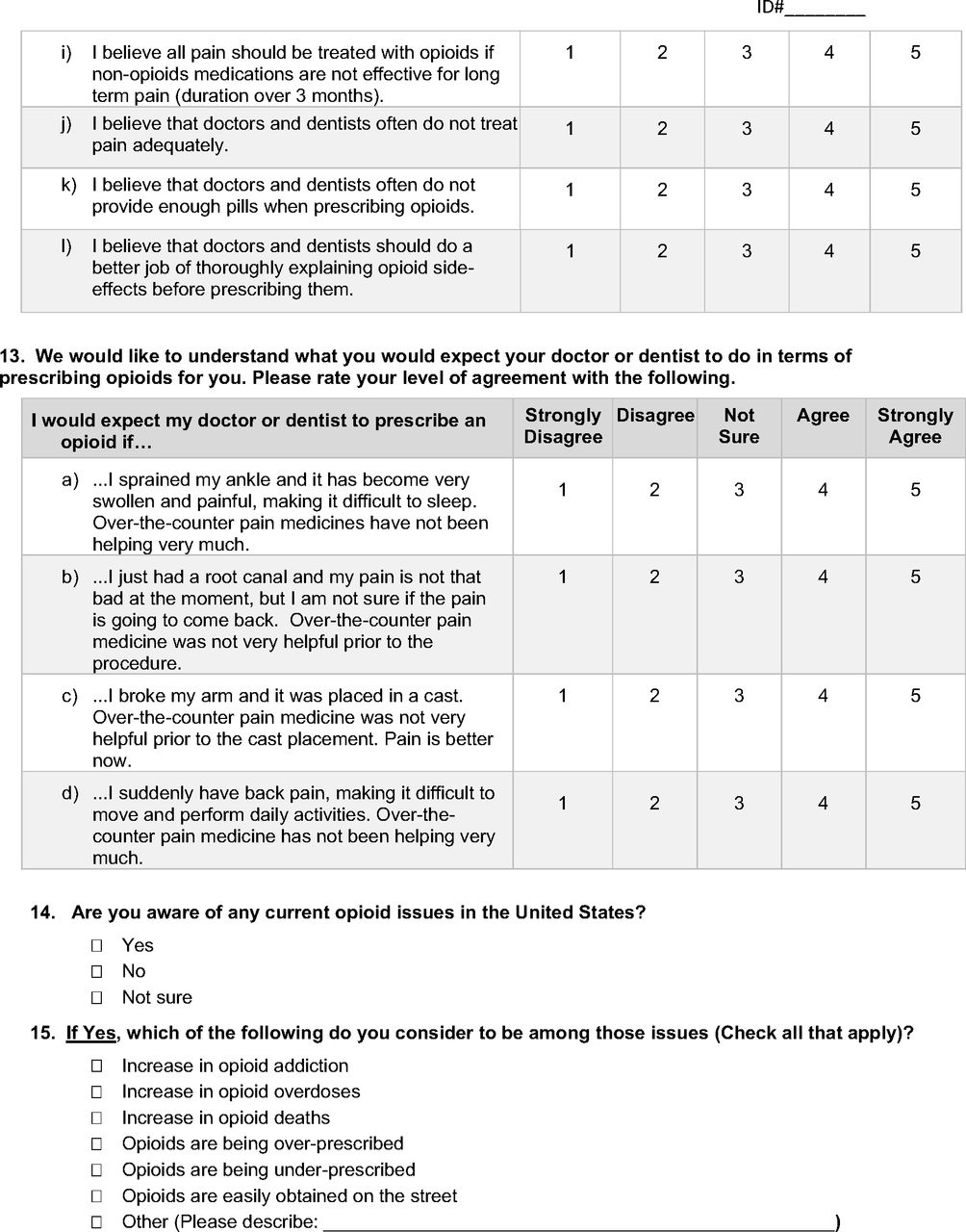
We asked about specific current opioid epidemic issues reported in the media and on official web sites.1,44⇓–46 Participants checked off issues that they were aware of, including increases in opioid addiction, increases in opioid overdoses, increased opioid deaths, opioids being over-/underprescribed, and the ease of obtaining opioids on the street. We then created an Opioid Epidemic Awareness Score, computed by tabulating each checked opioid epidemic issue as 1 point, and each unchecked issue as zero points. A total score of zero was possible if a patient was unaware of any of the opioid epidemic issues presented or if this section was left blank. Scores consisted of a minimum of 0, maximum of 7, and a median score calculated for the sample as 4. We then created a binary variable with a score of 4 and above as the “high” score (vs the “low” score), indicating participants with a higher awareness of epidemic issues.
Opioid side-effect and risk awareness:
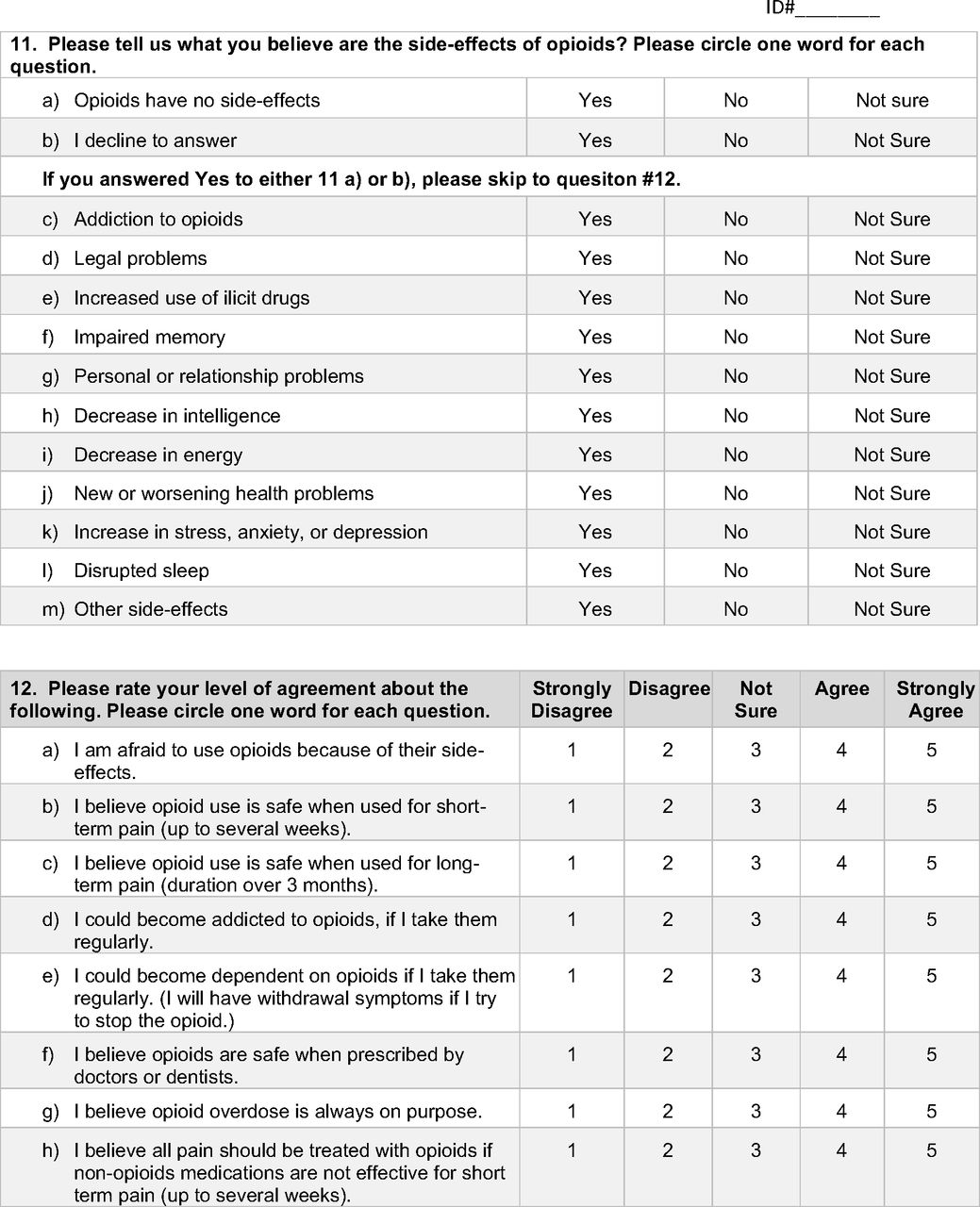
We asked about awareness of potential opioid side effects and risks, with items adapted from a previously published questionnaire on public beliefs (yes, no, or not sure) regarding the risks of marijuana: addiction, legal problems, increased use of illicit drugs, impaired memory, personal or relationship problems, decreased intelligence, decreased energy, new or worsening health problems, increase in stress/anxiety/depression, disrupted sleep, and other side effects.47 We then created our Opioid Side-Effect and Risk Awareness Score, with each side-effect/risk item counted as 1 point if answered “yes” and zero points if answered “no,” “not sure,” or if not answered, summed for a final score. A total score of 0 indicates a participant who was unaware of any side effects/risks, or who did not answer any of these questions. The scores have a maximum of 11, minimum of zero, with a median sample score calculated as 6. We then created a binary variable using a score of 6 and above as the “high” score (vs the “low” score), indicating participants with a greater awareness of potential opioid side effects and risks.
Opioids and pain-control beliefs:
These statements were created based on the first author (EO) and other collaborators' (TM, RD) clinical experiences of what patients may believe about opioids and pain-control. Examples of these statements include, “I am afraid to use opioids because of their side effects,” “I believe opioid use is safe when used for short-term pain (up to several weeks).” Level of agreement with each statement were rated on a 5-point Likert scale (“strongly disagree,” “disagree,” “not sure,” “agree,” and “strongly agree).” We then calculated an Opioid and Pain-Control Belief Score using eleven statements (Appendix Table 3). Statements ‘a’, ‘d’, and ‘e’ were reverse-scored, and ‘l’ was removed from the analysis as it was considered to be neutral. The Likert Scale was dichotomized into: “strongly disagree/disagree/not sure” versus “agree/strongly agree,” and each statement received either a 0 or 1 score, depending on the content. Under this approach, higher scores indicate having more positive beliefs about opioids and/or stronger beliefs on pain control. The score ranged from a maximum of eleven and minimum of zero, with a median score of 3. A score of 3 and above was set as the “high” score (vs the “low” score) for a binary variable. We reported opioid and pain-control beliefs descriptively in the trichotomized categories: “agree/strongly agree,” “strongly disagree/disagree” or “not sure.” (Appendix Table 3)
Independent variables:
Independent variables included the pain catastrophizing score and opioid expectations in at least 3 of 4 acute pain scenarios.20
Pain catastrophizing:
The Pain Catastrophizing Scale, a validated scale, consists of thirteen questions.22 To simplify the survey and decrease participant burden, we used a 2-item measure, as had been done in prior literature.48,49 Each item was measured using a Likert scale from 1 (“Never feel this way”) to 5 (“Always feel this way”), averaged by dividing by 2. We used a cutoff of 3 and greater to identify “high pain catastrophizing.”48,49
Opioid expectations in dispositional acute pain situations:
We created dispositional acute pain situations using 4 scenarios often seen in primary care and/or dental care settings (also described in our previous article20): 1) a sprained ankle, 2) a root canal procedure, 3) a cast placement for a broken arm, and 4) acute back pain. We asked participants at what level they would expect to be prescribed opioids for acute pain control in each scenario. A 5-point Likert scale was used to describe the level of agreement, with “strongly disagree,” “disagree,” “not sure,” “agree,” and “strongly agree.” Expectations of opioid prescriptions for each scenario were dichotomized into “strongly disagree/disagree/not sure” versus “agree/strongly agree.” We defined participants with “high” opioid prescription expectations as those who “agree/strongly agree” in at least 3 out of 4 scenarios (compared with “low” expectations).
Covariates:
We included the following survey respondent demographics: age, gender, and education level. Given the small sample size, ethnicity and race were not included in our analyses and categories were collapsed for most variables.
Data Storage
Paper survey data were manually transferred and stored using the Research Electronic Data Capture (REDCap) electronic data capture tools50 hosted at the institution involved. REDCap is a secure, web-based software platform designed to support research data collection and management system.50 The data were then transferred to Stata/IC15.1 for analysis.
Data Analysis
We conducted descriptive statistics for all variables. For each binary outcome, separate multiple logistic regression models were used to estimate covariate-adjusted odds ratios, by both pain catastrophizing and high opioid expectations. Model diagnostics were conducted to ensure that the regression model met assumptions and had acceptable discrimination and fit. All statistical tests were 2-sided and significance was defined as a P value of <0.05. All statistical analyses were performed using StataCorp. 2017 (Stata Statistical Software: Release 15, College Station, TX: StataCorp LLC).
Results
Study Sample Characteristics
A total of 108 surveys were completed between November 2018 and January 2019, from both clinics. Females accounted for 62% of participants and nearly half (48%) of the participant samples were aged 30 to 49. Most survey respondents were non-Hispanic (91%) and/or White (75%) and most either completed high school, or earned their General Educational Development (40%), or completed a college degree (40%) (Table 1).
Patient Demographics (n = 108)
Opioid Epidemic Awareness (Appendix Table 1)
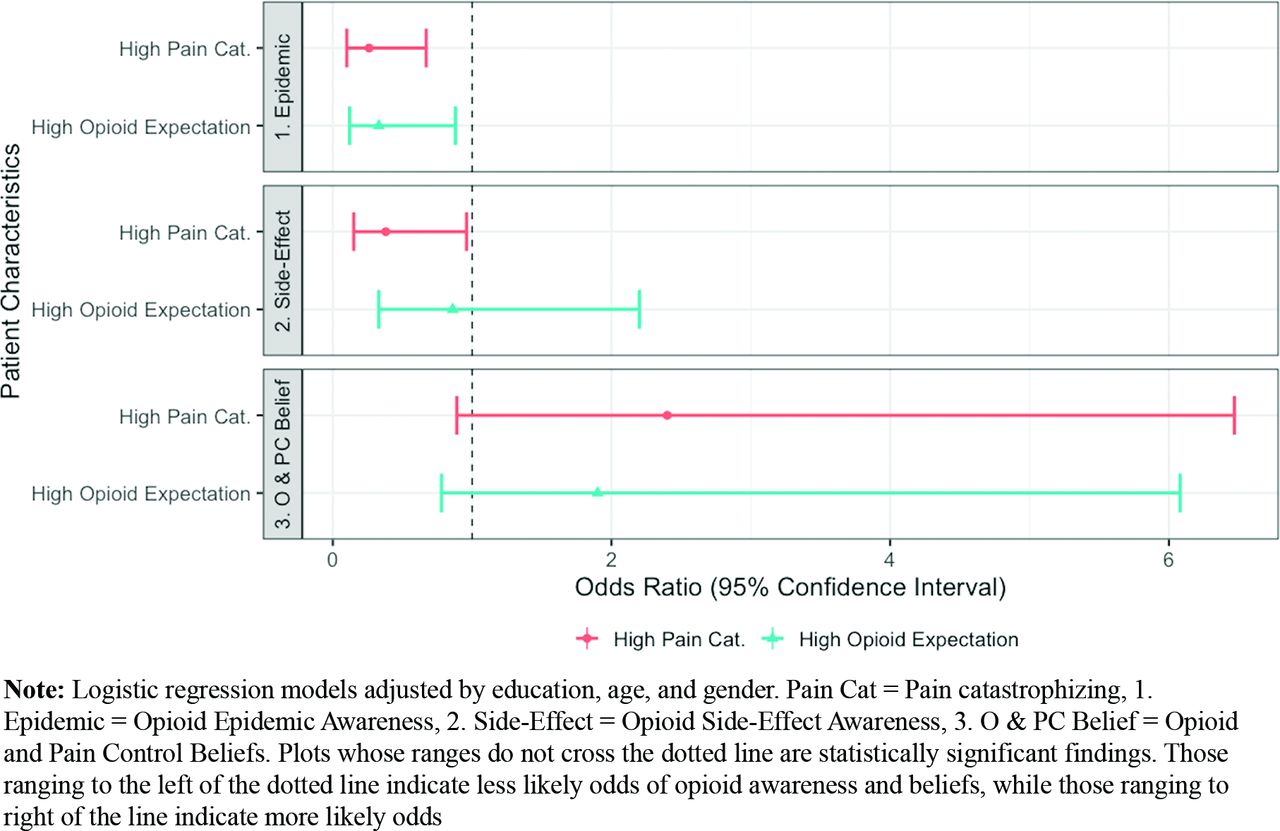
The top 3 epidemic issues of which participants were aware were increase in opioid addiction (n = 80, 74.1%), increase in opioid overdoses (n = 75, 69.4%), and increase in opioid deaths (n = 72, 66.7%). Eighteen (16.7%) of the study participants were not aware of or did not check off any issues related to the US opioid epidemic. High pain catastrophizing participants were 74% less likely to be aware of opioid epidemic issues, compared with low pain-catastrophizing participants (OR 0.26, P = .005, 95% CI:0.10-0.67). Participants who expected opioids in most dispositional scenarios were 67% less likely to be aware of opioid epidemic issues, compared with participants with low opioid prescription expectation (OR 0.33 P = .027, 95% CI: 0.12-0.88) (Table 2).
Adjusted Odds of Opioid Epidemic Awareness Scores/Opioid Side effect and Risk Awareness Scores/Opioid and Pain-Control Belief Scores by Patient Characteristics (n = 107)
Opioid Side-Effect and Risk Awareness (Appendix Table 2)
The 3 side effects/risks of which participants were most aware were addiction (n = 64, 79.0%); decreased energy (n = 57, 70.4%); and an increase in stress, anxiety, or depression (n = 56, 69.1%). Thirty-five participants (32.4%) either believed that opioids have no side effects/risks, or were unaware of any of the included side effects/risks, or did not answer the question. High pain catastrophizing participants were 62% less likely to be aware of opioid side-effect/risk items, compared with low pain catastrophizing participants (OR = 0.38 P = .040, 95% CI: 0.15-0.96). No other covariates were significantly associated with side-effect/risk awareness (Table 2).
Opioids and Pain-Control Beliefs (Appendix Table 3)
A majority (n = 70, 67.3%) of participants believed that opioids for pain control are safe when used short term (several weeks). Nearly half of the participants (n = 47, 45.6%) believed that opioids are safe when prescribed by doctors or dentists. Many believed that there is a potential risk of addiction (n = 58, 56.9%) and dependence (n = 56, 54.4%) when opioids are used regularly, and a majority did not believe that opioid overdose was always intentional (n = 70, 67.3%). Many agreed that doctors and dentists should do a better job of thoroughly explaining potential opioid side effects (n = 67, 64.4%). High pain catastrophizing (vs low; OR = 2.40 P = .083, 95% CI: 0.89-6.47) and high opioid expecting participants (vs low; OR = 2.18 P = .136, 95% CI: 0.78-6.08) had increased odds of holding more positive beliefs about opioids and/or stronger beliefs regarding pain control, though these did not reach statistical significance (Table 2). Figure 1 describes the odds ratios between high pain catastrophizing/high opioid expectation and opioid related awareness and beliefs.

Odds ratios between high pain catastrophizing/high opioid expectation and opioid related awareness and beliefs.
Discussion
In our study population, participants with high pain catastrophizing and high opioid prescription expectations for acute pain were less likely to be aware of current opioid epidemic issues. They may be more likely to hold positive beliefs regarding opioids and/or stronger beliefs regarding pain control; however, these scores were not statistically significant. High pain catastrophizing participants also were less likely to be aware of opioid side effects/risks.
Pain catastrophizing is one of the strongest psychological predictors of pain outcomes and is associated with adverse health outcomes, including greater disability, work absenteeism, and health-care utilization.22,23,51 Our previous study revealed an association between high pain catastrophizing and high opioid prescribing expectations in acute pain ambulatory settings.20 In our current analysis, high pain catastrophizing participants were less aware of opioid epidemic issues, potential opioid side effects, and opioid-related risks overall. This gap in awareness may explain why high pain catastrophizing patients crave and/or expect more opioids.27 They also might be more likely to hold positive beliefs regarding opioids. Although this association was not statistically significant in our analyses, likely due to our small sample size, the odds were higher among those who had high pain catastrophizing, as well as those with high opioid prescription expectations.
A study of primary care settings seeing chronic pain patients on opioids and their relationship to side effects showed high pain catastrophizing patients reporting a higher incidence of opioid side effects.52 Our study explored opioid-related awareness regarding epidemic/side effect/risks and found that high pain catastrophizing patients tended to lack this awareness. And yet, high pain catastrophizing patients may be at higher risk of actually experiencing opioid side effects.52 Opioid side effects can include depression and anxiety, conditions from which high pain catastrophizing patients often suffer,53 as compared with patients without high pain catastrophizing. Chronic pain patients with high pain catastrophizing and mental health conditions (depression, anxiety, post-traumatic stress disorder [PTSD], attention deficit/hyperactivity disorder [ADHD]) have also been shown to have more severe pain, poorer outcomes, and lower quality of life than those without mental health conditions.25 Another study of patients with chronic neck pain found high pain intensity, clinical insomnia, and a high level of depression/anxiety to be strongly associated with high pain catastrophizing.54
In acute pain management, similar to chronic pain management, it may be warranted that clinicians begin identifying patients most likely to benefit from being assessed for pain catastrophizing (eg, patients with chronic pain; and/or psychiatric diagnoses and/or insomnia;25,54,55 and/or opioid use disorder26). This is important as it would be almost practically impossible to screen every patient with acute pain for pain catastrophizing in busy outpatient settings. Once identified, high pain catastrophizing patients can be helped to better understand pain management in terms of their specific beliefs and expectations, and engaged in tailored treatment to meet their individual needs.55 If opioids are indeed a part of the treatment plan, information on opioid side effects/risks should be covered thoroughly, as there could be a gap in their awareness and beliefs about them. Considering the potential negative interaction between mental illnesses and opioid use, patients known to suffer from both should be monitored closely for any triggering of opioid misuse.56 A systematic review and meta-analysis on the best methods for reducing pain catastrophizing in adults with chronic noncancer pain found that cognitive-behavioral therapy, multimodal treatment, and acceptance and commitment therapy produced moderate-high quality results.51 In chronic pain patients, addressing pain catastrophizing early in treatment has been shown to have a positive impact on pain intensity, interference, and predictive of a reduction of subsequent catastrophizing.57 If early intervention for pain catastrophizing could improve the pain experience trajectory, it might be incumbent to assess patients for high pain catastrophizing early in the onset of pain symptoms, such as during acute pain care. Identifying risk factors for high pain catastrophizing can lead to early detection, thus early intervention. However, current opioid prescribing guidelines do not include pain catastrophizing screening.58 There are several validated, abbreviated versions of assessing pain catastrophizing scores, which could easily be administered in busy clinical outpatient settings.48,49,59
Participants with high opioid prescription expectations for acute pain were less likely to be aware of current opioid epidemic issues, while their awareness regarding opioid side effects/risks were not as statistically significant as with participants with high pain catastrophizing. However, in our study, high pain catastrophizing was an associated factor for having high opioid prescription expectations.20 One explanation for these observations could be that expectations of opioid prescriptions have become normalized for many patients in the US over the past few decades, during which time opioids have seen increasingly frequent use. Expectations of opioid prescriptions are likely formed by previous experience and shared knowledge. Thus, as opioid exposure declines,4,5 coupled with the availability of clear acute pain management guidelines,3,58 patients overall should begin to become more realistic in their expectations of opioid use in acute pain management, thus decreasing prescribers' need to meet patient expectations of receiving opioids. Individualized pain management will always be essential, such as in assessing pain catastrophizing for appropriate patients as described above.
A majority of our participants believed that doctors and dentists should do a better job of explaining opioid side effects to their patients. Close to one-third of our participants believed that opioids did not have side effects or declined to answer the question. Most also believed that opioids were safe when used short term, and nearly half believed that opioids were safe when prescribed by doctors and dentists. This further reinforces the need to better educate patients regarding opioid side effects and risks.
There are several limitations to this study. First, our survey participants were primarily White and our sample size was not large, thus we did not include race or ethnicity in our analysis. Participants were recruited using convenience sampling within a single academic institution. Thus, our findings might not be generalizable to other populations or settings. However, in our study, 74.1% of participants were aware of increased opioid addiction in the US, which compares closely to the a survey of 1,105 US adults reported by a PBS-Marist poll in 2017 where 80% of participants answered that opioid abuse was a problem in their community.60 While these questions are not identical, they speak to similar trends in opioid abuse awareness, further supporting the validity of our results when compared with a larger sample study. Second, due to limited resources, our survey design did not facilitate conducting conventional psychometric testing. And third, our questions regarding opioid side effects and risks were adapted from a previously published questionnaire regarding public beliefs on the risks of marijuana, rather than being specifically tailored for opioids.47
Future studies among patients with high pain catastrophizing and acute pain are needed to determine whether exploring patient beliefs regarding opioids and pain management can reduce opioid prescribing while also effectively managing pain. We also need to further assess the effectiveness of interventions specifically tailored to address high pain catastrophizing in acute pain care settings. And finally, we need to examine, in detail and in a larger sample, which side effects and risks high pain catastrophizing patients are less aware of, to facilitate further tailoring of specific education for those patients.
Conclusion
Our study shows that significant gaps exist among participants with high pain catastrophizing, regarding their awareness and beliefs concerning opioid epidemic issues and side effects/risks, and likely regarding opioids and pain-control in general, as compared with their low pain catastrophizing counterparts. This may partially explain why participants with high pain catastrophizing tended to expect more opioids. In acute pain care, as well as chronic pain care, it is warranted both to identify patients with high pain catastrophizing, and for clinicians to be aware of the risk factors associated with high pain catastrophizing. This may facilitate better exploring those patients' understandings, beliefs, and expectations regarding pain management, as well as tailoring their pain treatment and education appropriately to prevent adverse side effects.
Acknowledgments
Authors would like to thank Rick Deyo, MD, MPH, and Patty Carney, PhD, for assisting in survey development. Authors also would like to acknowledge the patients who graciously completed surveys for the study.
Appendix.

Distribution of Opioid Epidemic Awareness and Score
Distribution of Potential Opioid Side effects and Risks Awareness and Scores
Opioids and Pain-Control Beliefs and Scores
Notes
This article was externally peer reviewed.
This is the Ahead of Print version of the article.
Funding: none.
Conflict of interest: none.
To see this article online, please go to: http://jabfm.org/content/00/00/000.full.
- Received for publication September 12, 2022.
- Revision received December 5, 2022.
- Revision received December 11, 2022.
- Accepted for publication December 13, 2022.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}