
Article Figures & Data
Figures
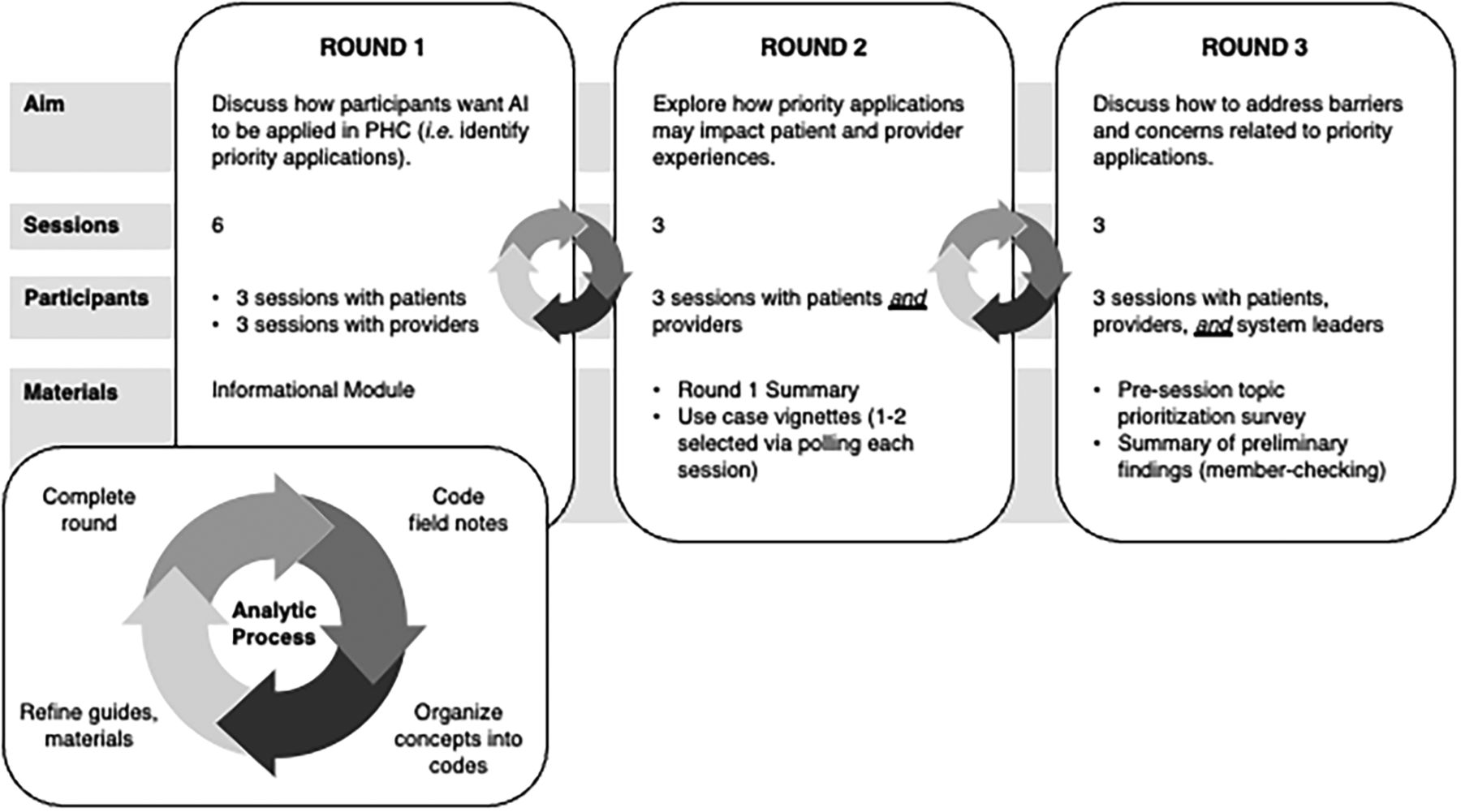
- Figure 1.
Deliberative dialogue process. Abbreviations: AI, artificial intelligence; PHC, primary health care.
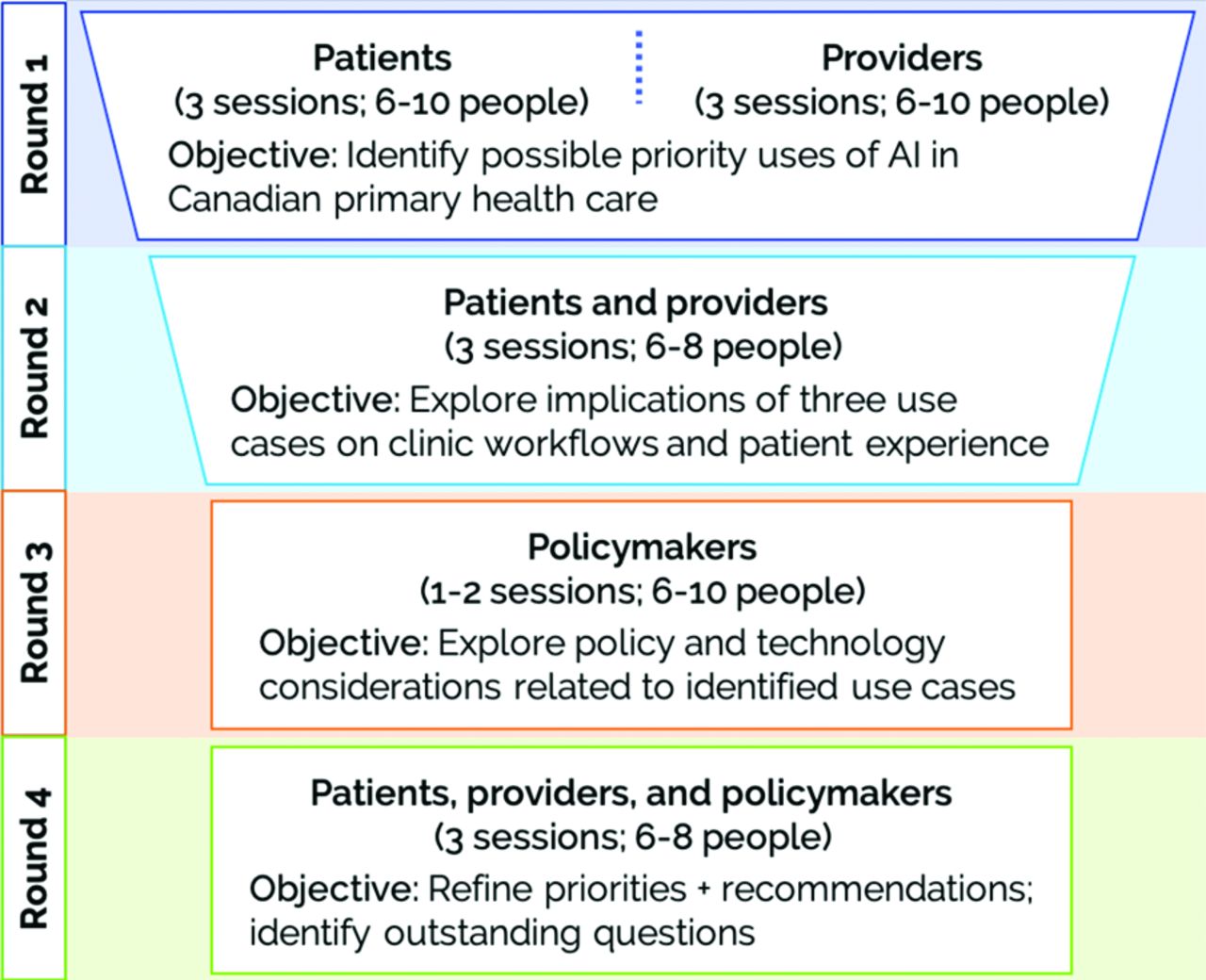
- Appendix 2 Figure 1.
Session topics for Future Perspectives on AI in Canadian Primary Care dialogue series.
- Appendix 2 Figure 2.
Artificial intelligence, machine learning, and Big Data (adapted from Jillian Macklin).
- Appendix 2 Figure 3.
Passport photograph of Alan Turing, the father of artificial intelligence, at age 16, by unknown author/CC BY 4.0.
- Appendix 2 Figure 4.
Layers of a supervised deep learning algorithm, by unknown author.
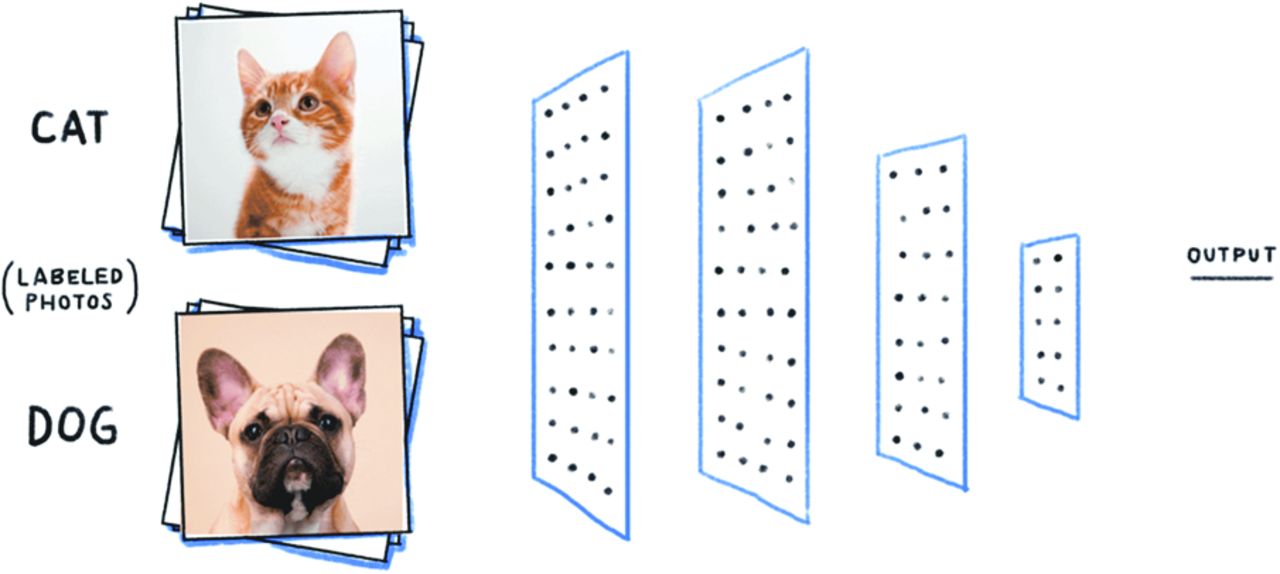
- Appendix 2 Figure 5.
Example photographs of cats and dogs that can be used to train a deep learning image classification algorithm, by unknown author.
- Appendix 2 Figure 6.
Facebook CEO Mark Zuckerberg demonstrates Facebook's facial filtering technology by Mark Zuckerberg.
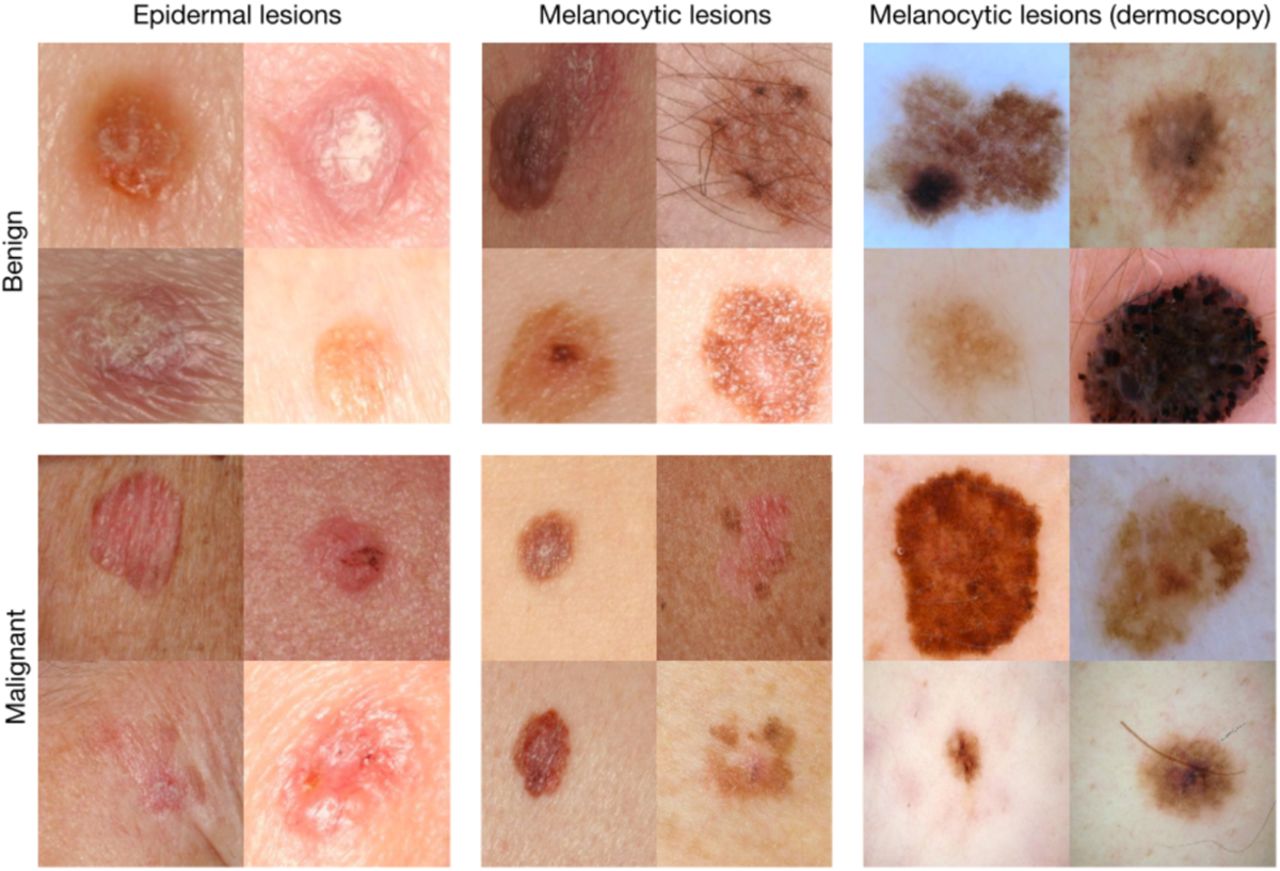
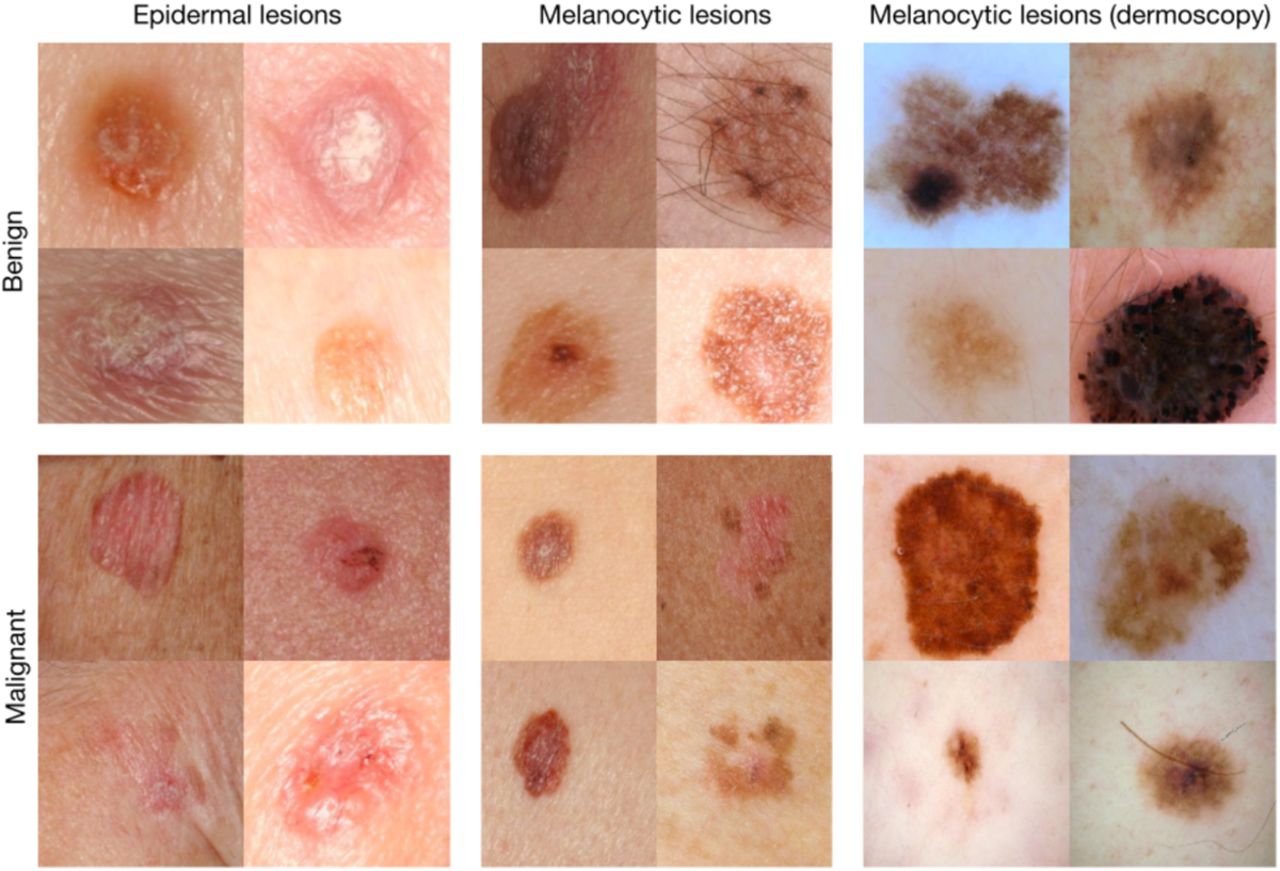
- Appendix 2 Figure 7.
Example images from a test dataset used to assess the performance of a deep learning algorithm by Esteva et al.12





Tables
Patients Providers Health System Leader Province n (%) British Columbia 1 (4.5%) 1 (4.8%) 1 (20%) Alberta 4 (18%) 2 (9.5%) Saskatchewan - - 1 (20%) Manitoba - 5 (24%) New Brunswick 1 (4.5%) - Nova Scotia 3 (14%) 1 (4.8%)* Ontario 12 (55%) 11 (52%) 3 (60%) Quebec 1 (4.5%) 1 (4.8%) Age in years Range, mean (SD) 23 to 73, 40 (16) 28 to 64, 42 (8.7) Gender n (%) Women† 12 (55%) 9 (43%) Men 9 (41%) 12 (57%) Nonbinary 1 (5%) - Race or ethnicity n (%) Black 2 (9%) 1 (4.8%) East/Southeast Asian 1 (5%) 2 (9.5%) South Asian 6 (27%) 5 (24%) White 13 (59%) 10 (48%) Mixed - 3 (14%) Self-rated artificial intelligence knowledge‡ 2.7 (1.1) 3.3 (1.2) Mean (SD) Provider type n (%) Chiropractor - 1 (4.8%) - Clerical staff - 1 (4.8%) - Family physician - 14 (67%) - Family medicine resident - 2 (9.5%) - Nurse practitioner - 2 (9.5%) - Social worker - 1 (4.8%) - Years in practice Mean (SD)§ - 12 (10) - Practice size‖ <250 patients - 6 (30%) - 250 to 750 patients - 6 (30%) - >750 to 1250 patients - 5 (25%) - Full-time equivalent clinical hours per week Mean (SD)¶ - 0.67 (0.30%) - Notes: Due to rounding, some totals may not perfectly sum to 100.
↵* Canadian province in which Denmark-licensed family physician studied health information technology in primary care settings.
↵† Including one trans woman.
↵‡ Participants rated their knowledge of AI on a 5-point Likert scale (1 was “Not knowledgeable at all,” 5 was “extremely knowledgeable.”
↵§ Calculation includes years in residency.
↵‖ Excluding residents, clerical participant.
↵¶ Calculation excludes clerical participant.
Abbreviation: SD, standard deviation.
Theme 1 Priority applications of AI in primary care Main idea Highest priority applications of AI are to areas where the current state of technology drives provider burnout, challenges patient-centeredness, or limits access to care. Quotes As a patient, I don't want my doctor spending his time facing the computer. I want him facing me…So in terms of looking at all of those admin tasks that are taking away from the patient care, I think AI has the potential to free up that time so that I have more face time with my doctor. — 39-year-old patient from British Columbia I think that doctors are often overwhelmed and overworked and if AI can be used to help with that, I'm all for that, so that they can be more efficient and more effective in their work. — 34-year-old patient from Alberta I was struck by the overlap in interests between providers and patients…What stood out was creating more time to be able to focus on actual patient and provider interaction… just having more of that time not taken up by all these other nonclinical issues. That…could represent a very safe, low-risk place to start and to sort of build upon AI within the primary care setting. — 42-year-old family physician from Manitoba My sense is that [triage in primary care] is absolutely abysmal…Like, there is no function, currently, of sophisticated pre-visit triage…In [my] clinic, people wait 20 minutes and hang up. They don't even call because it's so hard to get in. That's our triage system. If [there was] a way to…symptom check or…prescreen a little bit, they might be more likely to [come in]. — 48-year-old family physician from Ontario Theme 2 Impact of AI on primary care provider roles Main idea AI is not a substitute for provider expertise. It should be applied in ways that supplement core clinical skills and enhance patient-centered care. Quotes When I'm struggling [to manage my diabetes], sometimes…I'm just tired of being a diabetic. It's not because…I don't know how to take care of myself…It's only when a trust relationship has been built up with the doctor that he can begin to say, “Okay, I know you know how to take care of it. You don't seem to be taking care of it right now. What's going on for you?” I think you have to rely…on the trust relationship between the doctor and the patient to recognize specifically what's going on. It may be more subtle than the things that AI might pick up. — 73-year-old patient from Alberta In my case, I can tell you for sure that an AI would say, “Oh, she needs this prescription.” Meanwhile, that could kill me…There are nuances here that I don't think an AI could know…And look at it this way: in finance, we have controls in place…So, I would want the doctor to review that first. I'm all for them not having to do as much typing. I think it would save time, but there would have to be that review. — 55-year-old patient from Ontario Electronic health records have advantages for sure…But…the one thing I miss so much [is] that I can no longer do a genogram. There's nothing. They were never designed [for EMRs]. So, my family histories are so different than how I was taught with that picture. I did it with patients and we could really understand their family history from so many different angles. I used to love that part of care…We just have to be careful [with AI so] that we don't lose…strengths of [the] older model. — 57-year-old family physician from Ontario How does AI…consider the triad of, you know, what is the evidence? What is my experience that I've had after 35 years in practice? And what are the patient preferences?…I'm not sure how AI could pick up understanding my clinical experience. I don't know how AI can pick up what a patient's preferences [are] either. So, I think [of AI] as a tool…within our evidence-based medicine model. — 64-year-old chiropractor from Ontario Theme 3 Considerations for provider training in AI Main idea Formative and continuing education of primary care and other health professionals should cultivate basic AI literacy, algorithm critical appraisal skills, and safe, effective use within clinical reasoning processes and workflows. Quotes I would like to trust that my provider has a good perspective in AI so that he doesn't just sort of follow it slavishly but considers it as part of his care for me. — 73-year-old patient from Alberta I don't mean to sound like an alarmist about the dependency part. I'm not being reactionary. It's just, I have concerns about that. So, I wonder how [the use of AI] would be monitored, how doctors would be trained, how we would ensure that patients are getting still this benefit of experience and knowledge and not just this dependency. — 55-year-old patient from Ontario I have a 15-year-old who's learning how to drive. We have one car that has sensors and all sorts of safety features, and another car that doesn't….I feel like he needs to understand how to operate a vehicle at its base level before he can really make use of [safety features]…Maybe we need to emphasize the diagnostic reasoning, the history and physical pieces and the test ordering first, and introduce AI to that senior clinical learner…rather than right off the bat, so that they've got those building blocks behind them. — 44-year-old family physician from Alberta I think that part of what can help physicians [manage] our medical legal liability and risk is education and training around what these technologies are and what their purpose is…It's going to take a lot of awareness building among physicians to stay on top of how we can practice safely with the best interests of our patients in mind as these technologies become more widespread. — 42-year-old family physician from Manitoba AI, artificial intelligence.
- Table 3.
Desired Functions and Benefits of Priority Applications of Artificial Intelligence in Primary Care
Application Area Desired Functions Desired Benefits Higher priority Documentation Automate charting
Manage prescriptions (generation, refilling, forwarding)
Manage referrals
Mitigate provider burnout
Liberate time and cognitive freedom for:
∘ Direct, face-to-face patient interaction
∘ Discussions during a visit for patient goals, preferences, and circumstances
∘ Managing medical and social complexity
∘ Coordinating access to care for patients who face high barriers
Practice operations Triage Set an agenda before a visit by distilling patient concerns and taking partial histories
Assign concerns to management by virtual or in-person care modalities
Consider quality of life and functional impacts in determination of acuity*
Help patients decide if they can safely self-manage a concern, and if not, what health services they require
Prioritized access to synchronous modality of care delivery for those at risk of decompensation, medical need
Greater convenience for patients who receive virtual care, especially those with mobility challenges or living rurally*
Optimized provision of and access to care across delivery modalities
Decreased wait times*
Lower priority Clinical decision support Synthesize administrative, clinical (eg, patient history, past treatments), biometric data, and other “sources of truth” (eg, evidence, guidelines) to guide diagnosis, treatment, and care planning of rare diseases and common conditions†
Assist with management of medical complexity
Provide a “second opinion”; help providers “think outside the box”; transfer specialist knowledge into primary care
Improve speed and accuracy of diagnosis
Reduce trial-and-error treatments, uninformative or burdensome diagnostic tests, and multiple specialist referrals
Reduce rates of medical error
Proactive and preventative care Optimize contact with the provider to improve
∘ Care access
∘ Health equity
∘ Patient safety
∘ Team-based care†
Participant Group Sampling Frame Eligibility Criteria Recruitment PHC patients Purposive maximum variation (age, gender, race and ethnicity, education level, income, province of residence) English-speaking
Online advertisements (Kijiji, social media channels) in 10 provinces
Aged 18 or older
Patient advisor distribution list*
Visited PHC provider at least once in last year (virtual or in-person)
PHC providers Purposive maximum variation (gender, race and ethnicity, provider type, country of health professions education, years in practice, practice size, and province of practice) Any provider or administrative support person working in a PHC setting
Emailed invitation from Dr. Andrew Pinto (AP) to PHC colleagues interested in digital health or health informatics
Worked at least one clinical day per week
Emailed invitation from AP to practice colleagues†
Online advertisements (social media channels, PHC research network news channels)
System leaders Critical case Involved in digital health, health informatics, or PHC governance Emailed invitation from AP send to individuals within study team members' professional networks and those in relevant roles listed on health ministry public directories in 5 provinces‡ Patients Providers Health System Leader Province British Columbia 1 (4.5%) 1 (4.8%) 1 (20%) Alberta 4 (18%) 2 (9.5%) Saskatchewan - - 1 (20%) Manitoba - 5 (24%) New Brunswick 1 (4.5%) - Nova Scotia 3 (14%) 1 (4.8%)* Ontario 12 (55%) 11 (52%) 3 (60%) Quebec 1 (4.5%) 1 (4.8%) Age in years Range, mean (SD) 23 to 73, 40 (16%) 28 to 64, 42 (8.7%) Gender n (%) Female† 12 (55%) 9 (43%) Male 9 (41%) 12 (57%) Nonbinary 1 (5%) - Race or ethnicity n (%) Black 2 (9%) 1 (4.8%) East/Southeast Asian 1 (5%) 2 (9.5%) South Asian 6 (27%) 5 (24%) White 13 (59%) 10 (48%) Mixed - 3 (14%) Self-rated artificial intelligence knowledge‡ Mean (SD) 2.7 (1.1) 3.3 (1.2) Provider type Chiropractor - 1 (4.8%) - Clerical staff - 1 (4.8%) - Family physician - 14 (67%) - Family medicine resident - 2 (9.5%) - Nurse practitioner - 2 (9.5%) - Social worker - 1 (4.8%) - Years in practice Mean (SD)§ - 12 (10) - Practice size‖ <250 patients - 6 (30%) - 250 to 750 patients - 6 (30%) - 750 to 1250 patients - 5 (25%) - Full-time equivalent clinical hours per week Mean (SD)¶ - 0.67 (0.30%) - Notes: Due to rounding, some totals may not perfectly sum to 100.
↵* Canadian province in which Denmark-licensed family physician studied health information technology in primary care settings.
↵†Including one trans woman.
↵‡Participants rated their knowledge of AI on 5 five-point Likert scale (1 was “Not knowledgeable at all,” 5 was “extremely knowledgeable.”
↵§ Calculation includes years in residency.
↵‖ Excluding residents, clerical participant.
↵¶ Calculation excludes clerical participant.
Abbreviation: SD, standard deviation.
Category Definition Example Self-care, illness prevention, and wellness Tools that support people in living healthier lives A machine learning algorithm analyzes vital sign data from a patient's smartwatch in real time, documenting trends in their primary care electronic medical record (EMR). They receive personalized reminders to exercise, eat well, and get enough sleep. Their physician is alerted when trends show a decline in heart health. Triage and early diagnosis Tools that help triage patients and identify the need for additional health resources A machine learning-based symptom checker informs a patient with a gradual development of severe foot pain to book an appointment with their primary care provider as early as possible. Diagnostics Tools that assist providers with point-of-care diagnosis A primary care provider uploads a cell phone photo taken of a patient's retina to an app that uses deep learning to predict the risk of complications from diabetes. He refers the patient to an ophthalmologist.19 Clinical decision support Tools that structure relevant information to help physicians determine treatment course or need for referral to specialist or acute care services An EMR-integrated machine learning algorithm predicts which patients are at high risk for becoming infected with HIV within a 3-year timeframe. Risk profiles can help primary care providers who would most benefit from pre-exposure prophylaxis medications.20 Care delivery Tools that support direct interactions between patients and providers A natural language processing tool automatically converts the conversation between a patient and provider into chart notes, orders laboratory tests, and writes referrals to specialists during a clinic visit. This tool can also reach out to patients in advance of the appointment to gather necessary information.21 Chronic care management Tools that help patients and providers manage chronic diseases like diabetes or heart disease A patient with diabetes has a blood glucose monitor that syncs with an AI-based app on their phone. The algorithm learns the patient's dietary and insulin delivery schedule over time. It begins to send helpful reminders to eat, check blood glucose, and inject insulin. The app is integrated with the patient's primary care EMR. It notifies the provider when the patient's insulin needs appear to change significantly. Population health management Tools that analyze large datasets to identify trends in population health to inform shifts in clinical programs and intervention targeting A deep learning algorithm analyzes a clinic's raw EMR data. It identifies the patients at the highest risk for hospital admission within the next 30 days. Providers in the clinic schedule appointments with these patients to discuss their health and preventative interventions.14 Health care operations Tools that decrease time spent on routine administrative tasks that occur in the background of patient care A classical machine learning algorithm learns that times and days of the week where appointments are in highest demand, and helps clinic clerical staff optimize the staffing schedule
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Artificial intelligence in primary care practice: Qualitative study to understand perspectives on using AI to derive patient social data
- Developing an AI Tool to Derive Social Determinants of Health for Primary Care Patients: Qualitative Findings From a Codesign Workshop
- Research Representing the Changing Landscape of Family Medicine