
Abstract
Background: Primary care practices can help patients address obesity through weight loss; however, there are many barriers to doing so. This study examined weight management services provided and factors associated with higher reported provision of services.
Methods: A survey was given to practice members in 18 primary care practices in a Colorado-based health system. The survey assessed weight management services to determine the amount and type of weight loss assistance provided and other factors that may be important. We used descriptive statistics to summarize responses and linear regression with generalized estimating equations to assess the association between the practice and practice member characteristics and the amount of weight management services provided.
Results: The overall response rate was 64% (254/399). On average, clinicians reported performing 73% of the services, and when grouped into minimal, basic, and extensive, the clinicians on average performed 87%, 68%, and 69% of them, respectively. In a multivariable model adjusted for demographics, factors associated with performing more services included perception of overall better practice culture and perception of weight management implementation climate.
Conclusions: Practice-associated factors such as culture and implementation climate may be worth examining to understand how to implement weight management in primary care.
Introduction
Obesity is a critical public health issue contributing to the leading causes of death in the United States.1 Primary care serves as a common setting for addressing prevention and treatment of disorders caused by obesity, such as diabetes and hypertension, and many patients note weight management as a top priority.2⇓⇓⇓–6 There are many evidence-based treatments available for patients with obesity, including medications, diet and nutrition counseling, behavior change support, and surgery; however, these treatments are often not implemented in primary care.7⇓⇓–10 Although clinicians note the high importance of treating patients’ obesity as a standard of care,11 barriers include insufficient clinician training/familiarity with obesity treatment; challenges with access for/prioritization of obesity treatment; lack of workable structures, workflows, and resources; and low/no reimbursement for direct provision of obesity care without other comorbidities.12⇓⇓–15 Patients also face many barriers including stigma, lack of motivation, ability to successfully lose weight, and cost and lack of access to services.16⇓⇓–19 However, recent research reveals that practices can, in fact, deliver obesity care if the barriers are identified and addressed.12,20 With structures and supports in place, patients are achieving weight loss outcomes that have potential to slow the public health trends toward increasing obesity and the resulting comorbid conditions.21⇓⇓⇓⇓–26
Understanding more about what motivates primary care practice members toward providing obesity care and what steps could be taken to overcome perceived barriers is needed. This study reports on a survey completed by practice members at 18 diverse primary care practices in Colorado regarding their perceptions of the importance of obesity care in their practice, what services are currently provided, satisfaction with the care provided, challenges with providing obesity care, and interests in overcoming these challenges. These data add to the growing knowledge base about overcoming implementation challenges to address this public health problem.
Methods
PATHWEIGH Study
The data for this report were gathered as part of a National Institutes of Health–funded clinical trial on implementation of PATHWEIGH. PATHWEIGH strives to be a comprehensive approach including electronic medical record tool sets, weight management training for clinicians, and specialist consultation support. This study uses a type 1 hybrid effectiveness-implementation stepped-wedge cluster randomized design to compare adult patient-specific and implementation outcomes of a weight management intervention to standard of care in adult-serving primary care clinics in Colorado (n = 57).27 This article reports on an analysis of the baseline surveys given to practice members at the primary care practices before the start of the intervention for the first cohort of 20 clinics. Two surveys were used: (1) a practice survey completed for each practice, and (2) a practice member survey that was administered to clinicians (ie, physicians and advanced practice providers including physician assistants and nurse practitioners), other providers, and staff within each practice.
Survey Instruments
The practice survey (Appendix 1) was developed to identify practice-level characteristics and behaviors. The purpose of the survey was to provide basic information on the characteristics of the practice including the patient population, location and type, quality improvement efforts, and current weight management services. It assessed the capacity of the clinic for implementation of a weight loss intervention by identifying the number of staff and clinicians, the current treatment and billing practices regarding weight management, and whether the practice was actively engaged in quality improvement practices. No standardized scales were used in this survey.
The practice member survey (Appendix 2) was developed to assess individual practice members’ backgrounds and demographics, current perceptions of weight management importance and climate for implementation, current weight management activities provided for patients, and clinicians’ background and experience with providing weight management and interest in learning more about providing weight management. Several scales were used to assess overall practice culture at the individual and practice level as well as burnout and work satisfaction of practice members. These scales were not related to weight management in the practice but intended to assess the overall milieu of the practice.
The Practice Culture Assessment Scale included 22 Likert scale items (1 = Strongly disagree to 5 = Strongly agree) that were used to compute scores for the subscales of Change Culture, Work Culture, and Chaos.28⇓⇓⇓–32 Subscale scores ranged from 0 to 100, and higher scores represented more of the concept. An Overall Culture score was also computed by averaging the scores of the 3 subscales (reverse coding the Chaos subscale), where a higher score indicated stronger practice culture. Change Culture items focus on how the practice approaches collaborative quality improvement, problem resolution, and change management. Work Culture items assess how practice members work together for a pleasant and productive practice environment and high-quality care, and Chaos items assess instability, disruption, and disorganization in the practice.33 Practice culture is often found to be related to the ability of the practice to implement new initiatives and may be useful in understanding implementation of weight management efforts.34,35
Burnout and work satisfaction was assessed by asking practice members 3 questions about their level of burnout (1 = No burnout to 5 = Complete burnout),36,37 if they felt personally rewarded by their work (1 = Not rewarded to 5 = Fully rewarded), and if they were satisfied in their current practice (1 = No satisfaction to 5 = Complete satisfaction).38 These attributes of employees can have an impact on their interest and ability to take on new initiatives such as a weight management intervention.39⇓–41 An overall Work Satisfaction score was computed by averaging the scores across the domains (reverse coding burnout), where a higher score indicated that respondents had greater satisfaction from their work.
Additional measures were used to determine current practices and readiness for weight management as an intervention, specifically. To assess current practices in the provision of weight management, clinicians were presented with 19 weight management services or tasks and were asked to indicate the frequency with which they provided the services (not at all, sometimes, very often), which were then dichotomized (not at all vs at least sometimes) for analysis. Based on divisions within how weight management is likely to be categorized in primary care practice, 3 groupings were created a priori based on what level of support for weight management they provided. Group 1 was minimal and included essentially identification of weight as an issue and brief one-time advising to patients. Group 2 was basic weight management treatment that was short term and limited in options. Group 3 was comprehensive support characterized by more use, more in-depth treatment options, and ongoing care over time including repeated visits and tracking. Questions related to direct provision of weight management services were only asked for respondents who had indicated that they were medical providers.
An Implementation Climate Scale for interventions was used to address the ability of a practice to effectively implement a weight management intervention in the primary care practice setting.42 It included 6 questions within 3 constructs (Expected, Supported, Rewarded) with Likert scale responses from 1 = Not at all to 5 = To a great extent. An average score was computed for each individual and then averaged within a practice to present a practice-level climate score ranging from 1 to 5. Higher values indicate a better organizational climate for weight management, with a range from 1 to 5. Intraclass correlation coefficient (ICC) was estimated, where values closer to 1 indicate that climate perception is more strongly shared among practice members.
Data Collection
The practice survey was completed by a single practice administrator at each of 20 clinics. The practice member survey was administered to all clinicians and staff at each of the practices. The surveys were implemented in REDCap and were pretested with nonstudy practice clinicians and research team members to ensure that the survey questions were concordant with the study team’s research questions. A personalized link was distributed by e-mail to all practice members at the 20 practices. To increase response to the survey, respondents were compensated with a $10 gift card, and 2 reminders were sent 3 weeks apart. Practice members also received compensation for participation in interviews (not reported here) and a lump sum amount to the practice for assistance with other data collection efforts such as observation and identification of patients for interviews.
Data Analysis
Descriptive statistics (means, medians, frequencies, percentages) were used to summarize responses. Spearman correlations were used to study relationships between the scale scores. We used linear regression to assess the association between the clinician characteristics and the amount of weight management provided. To account for potential correlation between survey respondents within the same practice, we used a generalized estimating equation approach with an independence covariance structure. Respondent demographics (age, gender, years of experience) and variables that had P < 0.1 in univariable analyses were included in a multivariable model. All analyses were performed using R version 4.0.4.
Results
Although all practices completed some surveys, 2 practices were omitted from the analysis because they declined to participate in the study. Among the remaining 18 clinics, the overall response rate was 64% (254/399), with an average response rate within practice of 68% among all practice members and 66% among clinicians, specifically. Of the respondents, 70 (28%) were clinicians, 8 (3%) were other providers (eg, behavioral health, pharmacy), 120 (47%) were clinical support staff, and 54 (21%) were administrative staff. Compared with the other practice member roles, clinicians had the highest proportion of males (47%), those aged over 45 (58%), and those with a part-time position (37%) (Table 1). Clinicians also had the highest median years of experience (20; interquartile range [IQR]: 10 to 25). A large proportion of respondents (85%) indicated that they had personally wanted to or had tried to lose weight.
Respondent Characteristics, Overall and by Role
Current Status of Providing Weight Management
From the practice survey, out of the 18 clinics, only 6 (33%) indicated that their clinicians provided visits specifically for weight management, using brief advice and/or counseling to patients during these visits. Only 4 (22%) additionally had follow-up visits. In contrast, 15 (83%) practices indicated that their clinicians or other providers provide brief advice on weight loss during office visits for other conditions or specified purposes. A higher proportion of practices indicated that they made referrals for bariatric surgery (67%), referrals to weight loss programs (50%), prescribed weight loss medication (44%), and provided patient education material on weight loss (39%). No practices indicated that they provided medical supervision for meal replacement programs, information about insurance coverage of obesity treatments, or group weight loss programs on-site. For 9 practices (50%), the practice administrator was not aware of how weight loss services or visits were billed/paid for in the practice, and most (83%) did not know if their practice had experienced any difficulties with billing for obesity services from any payer.
From the practice member survey, clinicians were surveyed about their use of 19 listed services for weight management. Of the 19 listed services for weight management (Figure 1), on average clinicians indicated that they performed 73% (IQR: 63% to 83%) of the services. Of the services in group 1 (minimal), 2 (basic), 3 (superior), on average clinicians performed 87%, 68%, and 69% of the services, respectively, with 97% of providers indicating that they provide at least 1 service in each group. There were 36 (55%) providers that provided all services in group 1, 3 (5% of total) that provided all services in groups 1 and 2, and the same 3 that provided all 19 of the services. None of the clinicians indicated that they had obesity treatment certification, 40 (58%) had never received additional continuing medical education (CME) on how to provide obesity treatment or weight loss, and 25% said that they had received this CME but that it was not within the past 3 years.
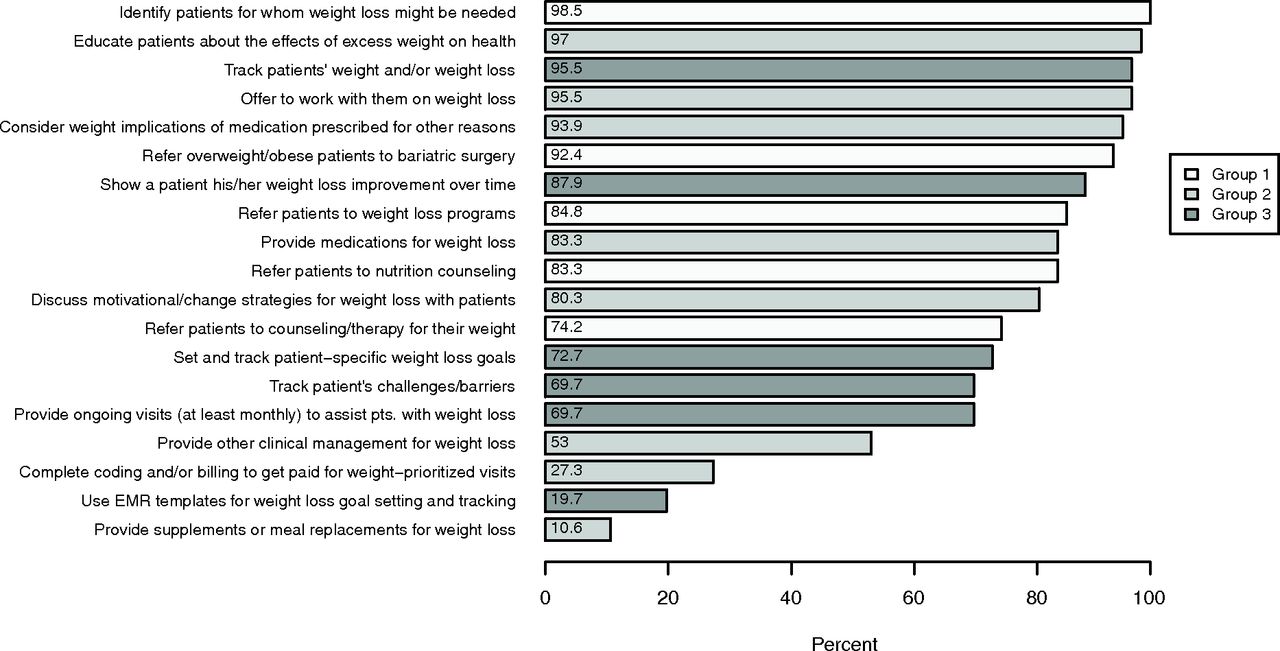
Percentage of clinician respondents that indicated that they provided each of the weight management services. Groups indicate the level of weight loss services conducted (1: minimal, 2: basic, 3: superior). Abbreviation: EMR, electronic medical record.
Perceptions about Providing Weight Management
Clinicians and other medical providers were asked about their satisfaction with their practice’s ability to help patients with weight management, for which 38% indicated that they were somewhat satisfied, 29% said they were not satisfied, and 21% responded that it depended on the patient. They had an average score of 4.3 (IQR: 4 to 5) on a Likert scale question (1 = Totally disagree to 5 = Totally agree) asking about agreement with the statement that weight loss for patients with overweight or obesity is something that a primary care practice should provide as part of comprehensive primary care. When provided with a list of concerns about making weight management a priority (Table 2), the most reported concern by clinicians was that they did not have time in their schedule (70%). For clinical support staff, their reasons were that they did not have weight management workflows set up in their practice (46%), which was also indicated as a concern by administrative staff (31%).
Top Concerns for Providing Weight Management, by Role
Climate for Implementing Weight Management
In the practice survey, all of the 18 practices indicated that they had quality improvement activities happening in their practice. Most practices (67%) indicated that they had a practice leader who drives forward quality improvement. Many (61%) also had a process for identifying quality improvement goals and tracking progress toward goals. More than half (56%) of the practices indicated that they had at least some or great success when quality improvement efforts were attempted in their practice, and 33% indicated that it varied by the specific effort.
In the practice member surveys, respondents completed a scale assessing climate for implementing weight management in their practice. The median Implementation Climate Scale for weight management across the sites was 2.4 (IQR: 2.2 to 2.7; range: 1.9 to 3.1), which indicates a moderate climate for performing weight loss management. We assessed the reliability of this practice-level construct in our sample and found that within a practice there was variability in the responses of practice members (ICC = 0.34). There was moderate positive correlation (ρ = 0.27) between the individual and practice-level measures of implementation climate. There was moderate negative correlation (ρ = -0.10) between implementation climate at the practice and the number of quality improvement initiatives occurring in the practice, indicating that practices with more quality improvement activities happening had a lower implementation climate for weight management.
For the practice culture (not specific to weight management), the respondents overall had high Change Culture (median: 75; IQR: 65 to 82.5), moderate Work Culture (median: 59.4; IQR: 50 to 68.8), and low Chaos (median: 31.3; IQR: 18.8 to 50). The Chaos subscale had the greatest variability across the different practices, with median Chaos score within practices ranging from 18.8 to 56.3. The overall Practice Culture was moderate (median: 66.7; IQR: 55.6 to 76.3).
For the 3 domains assessing burnout and work satisfaction, 40% of respondents indicated experiencing at least some burnout, the majority of respondents (83%) agreed/strongly agreed that they felt that their work was personally rewarding, and most respondents (77%) agreed/strongly agreed that they were satisfied in their current practices. Clinicians experienced a greater sense of burnout (59% indicated at least some burnout), felt less rewarded (71% agreed/strongly agreed), and were less satisfied (64% agreed/strongly agreed) than the other roles. There was strong positive correlation (ρ = 0.55) between individual-level perception of overall Practice Culture and their Work Satisfaction score.
Learning about Weight Management
The vast majority of clinicians (96%) indicated that they would be interested in learning more about at least 1 of the presented weight management topics. The highest-ranked topics were recommendations about diet and eating plans and organizing workflows to accommodate weight management. Of the suggested ways to learn about weight management, 69% indicated that they would like to learn using a single 2-hour e-learning module and get CME credit, 53% wanted someone to come to the practice to provide information, 41% wanted resources in a program like UpToDate (a subscription-based online clinical reference), and 33% wanted to be able to call another clinician experienced in weight management to ask questions.
Factors Associated with the Provision of Weight Management
Using regression analyses with a generalized estimating equation framework to account for clustering, we studied what clinician and practice factors contribute to how much weight management is provided. We define this outcome as the total number of weight management services selected from the list of 19 services and a free-text field for “Other” (range: 0 to 20). In bivariable analyses (Table 3), being female, individual-level perception of practice culture, and individual-level perception of implementation climate were associated (P < .05) with providing more services. In a multivariable model adjusted for respondent age, gender, and years of experience (Table 3), the mean number of services provided by clinicians was greater for women (P < .001), those aged 45 years or younger (P = .07), and those with a better perception of their practice’s change culture (P = .004) and better implementation culture (P = .07).
Generalized Estimating Equation Results for Association of Clinician and Practice Factors with Amount of Weight Care Management Provided (n = 63)
Discussion
In this study of weight management efforts, we found clinicians reported providing many services already such as identifying weight as a health issue, providing education on weight and its effects on health, referring to other services for weight loss, and providing education and support for weight loss efforts. However, few clinicians reported providing ongoing care for weight management such as using ongoing tracking and other clinical management. This sample of clinicians and other practice members did not report a high level of satisfaction with the assistance they are currently providing in this area, although there was a high level of interest in learning more and support for providing weight management as a standard of care.
These results also make clear the importance of contextual factors in association with services provided by clinicians for weight management. Practice culture and gender were significant factors related to the total number of weight management services. Higher implementation climate for weight management and younger age (≤45 years old) were marginally associated (P = .07) with providing additional weight management services. This indicates that practices could improve in the culture for implementation of weight management by receiving more recognition and support (elements of implementation climate) for providing weight management services. Support could be in the form of removal of common barriers noted such as not having enough time or not having workflows set up for weight management. Creating a supportive culture for weight management could also look like offering recognition and encouragement of clinicians learning the most effective approaches for treatment of obesity or offering visits prioritized on weight. In addition, having dedicated staff who champion the use of services that promote weight management could also contribute to improving the practice environment with support for weight management.43 Supportive culture as an element of implementation is consistent with the abundant literature on other practice improvements in primary care such as medical home transformation.34,44,45
These results are consistent with other previous research on the existence of barriers to implementation of weight management services but extends understanding to why these barriers exist. The practice survey found that, even though all of these practices had support for quality improvement, this support varied. Lack of support for quality improvement could thwart efforts for any type of quality improvement effort.46 However, we also found that practices with a larger number of ongoing quality improvement projects were more likely to have a less positive implementation climate for weight management and fewer weight management services provided by its clinicians. This suggests that in these practices their priorities were already aligned elsewhere and/or that they lack capacity to take on new initiatives. This is consistent with previous research that priority and capacity are both important factors to implementation.47 Realigning priorities at the practice level could overcome this challenge by becoming informed on the benefits that weight loss could have for many patient metrics such as Health care Effectiveness Data and Information Set (HEDIS).
One area where our results differed from others was the financial impact of weight management services. Lack of reimbursement is a common barrier; however, this was not stated as such in our study. “We will not get paid/will lose money” was selected as a barrier by only 20% of clinicians, 0% of other providers, and 4% of staff. We wonder if in these health system practices, practice team members are insulated from the financial aspects of billing and coding by having system-level support for this area rather than being more directly involved themselves. In terms of weight management services in our list, “Complete coding or billing to provide weight prioritized visits” was only answered by 27.3% of clinicians. Perhaps many clinicians provide one-time advice and assistance and simply use billing under other conditions using standard evaluation and management codes. This could have important implications for implementation aspects of getting more adoption of these services in primary care.
Limitations include that these data represent the responses of practice members in 1 health system in 1 state. Although the practices were geographically dispersed and represent different patient populations, they may not represent all primary care practices nationally. The results may have been different if the full sample had completed the survey; results may be biased toward those more interested or available to comment on the topic of weight management. Results may have also been biased by respondents having more favorable impressions of their activity than are actually true. The PATHWEIGH study is a study of weight management provided to adults. The issues with provision of services to children and adolescents may be different, and these results do not reflect those differences. These data were collected during the COVID-19 pandemic (March-June 2021), which may have influenced response rates and results given other priorities at the time and the need to administer the surveys all online.
Conclusions
Providing more assistance with weight loss is needed in primary care to address the rising rates of overweight and obesity in the United States. The study illustrates factors that may make implementation of weight management a challenge and point to solutions for addressing this issue. Recommendations may include providing a more supportive environment for clinicians to practice weight management such as by providing additional help, encouraging enhanced training, and/or recognizing successful weight management efforts and outcomes. Realigning priorities at the practice level could help motivate practice clinicians and staff to participate more in providing these services, perhaps by highlighting the benefits that weight loss could have for many patient metrics such as HEDIS. Further research should investigate if interventions that address these challenges directly result in greater attention to weight management and better results for patients’ health status in terms of prevention of obesity-related comorbidities.
AppendixAppendix 1. PATHWEIGH weight management study practice survey
Appendix 2. PATHWEIGH weight management study practice member survey


Notes
This article was externally peer reviewed.
This is the Ahead of Print version of the article
Funding: National Institutes of Diabetes, Digestive and Kidney Diseases (NIDDK; grant #1R18DK127003).
Conflict of interest: None.
To see this article online, please go to: http://jabfm.org/content/36/1/000.full.
- Received for publication June 24, 2022.
- Revision received August 12, 2022.
- Accepted for publication August 17, 2022.




{kind=link}