
Abstract
Introduction: Comprehensiveness is a defining principle of primary care and Family Medicine but is declining in some settings. This study explores the relationship between practice setting and comprehensiveness among family physicians (FPs).
Methods: Using 2014 to 2016 American Board of Family Medicine survey data to generate scope of practice (SOP) scores (0 to 30) for FPs. We ran univariate and bivariate analyses for services by practice organization type. Our principal independent variable was practice organization type and dependent variable, the SOP score.
Results: Among 25,117 total respondents, FPs at rural health centers (RHC) had the widest scope of practice (SOP score of 17.7) whereas FPs in federal, urgent care and other safety net clinics had the narrowest with mean SOP score of 14.0 or less. Higher rates of FPs practicing in Federally Qualified Health Centers and academic health centers were providing a women’s health service, except for deliveries, whereas FPs in rural health centers were providing obstetric services (24%). The proportion of FPs providing newborn care was highest in RHCs and lowest in the urgent care setting (85%, vs 26%). A higher proportion of FPs in RHCs provided joint injections and skin procedures than FPs in other practice organizations.
Conclusions: Significant variation in FP comprehensiveness exists across different practice types. FPs in practice types commonly associated with large health systems had narrower breadth of practice, concerning amid increasing practice consolidation. Given associations between comprehensiveness and desirable health care outcomes, policy makers should encourage payment/accountability models that incentivize broader SOP.
- Career Choice
- Family Medicine
- Practice Management
- Primary Health Care
- Rural Health Services
- Scope of Practice
- Urgent Care
- Workforce
Introduction
Family physicians (FPs) deliver medical care in a variety of settings, clinics and practices. Residency training in Family Medicine prepares graduates for a wide scope of practice. All residents in Family Medicine must deliver babies, take care of patients in both ambulatory and inpatient settings, and learn procedural skills. Having a broad scope of practice (SOP) can enhance access and reduce costs, particularly among underserved populations or rural communities that have more difficulty in obtaining specialty services.1 Maintaining a wide scope and using the broad range of skill sets within 1 practice type allows clinicians to build continuity and important therapeutic relationships with their patients.2 Furthermore, a wide SOP is important to achieve parts of the quadruple aim including the patient experience, which is positively rated when patients can receive many services at 1 practice location. One study found that SOP, along with wait times and cost, were important attributes of patient satisfaction within primary care.3 Just as important as the patient experience is the physician experience, which SOP has been shown to influence. A broader SOP has been associated with lower rates of burnout. Specifically, practicing inpatient medicine and providing obstetric care were found to have a 30% and 36% lower odds of reporting feeling burned out, respectively.4
Family medicine residents receive wide training but that does not necessarily predict how they apply those skills in future patient care. One study of 2016 Family Medicine graduates found that a majority of respondents felt being prepared to provide 14 of 25 services, however in actual practice, a majority only provided 4 of those services.5 Recent graduates of Family Medicine residences report an intention to provide a broad SOP, which is significantly higher than current practitioners, suggesting that barriers exist to providing care to the maximal extent of training.6 Multiple studies in 2019 found that graduates that wanted to provide obstetric care found that those jobs were not available.7,8 These findings suggest that employers and practice setting might influence the services that FPs are able to provide, and that limited support from employers or practices can inhibit FPs abilities to practice to their fullest extent and depth of care.9
Residents who have graduated from rural residency programs exhibit a broader SOP than their urban counterparts.10 Previous studies found that the size of a practice can influence the breadth of services offered by physicians. One study in particular, demonstrated that FPs in small and medium-sized practices (between 2 and 20 providers) have a broader SOP when compared with solo or large practices.11 One Canadian study found that academic and private offices were positively associated with increasing scope, whereas community clinics were negatively associated with SOP.12 Yet, to our knowledge, this has not been examined for FPs in the United States, where practice environments and market pressures are different from those in Canada. There have not been any other studies that specifically look at the effect of different practice types on the breadth of SOP among physicians, especially FPs. Therefore, the aim of this study was to compare the SOP of FPs by practice type.
Methods
We used 2014 to 2016 American Board of Family Medicine (ABFM) Family Medicine Certification (FMC) examination demographic registration questionnaire data from FPs seeking to continue their certification. The questionnaire is a required component of registration and is completed 3 to 4 months before examination date.13 We first geocoded addresses of the FPs’ practices for each of the survey years and then linked it with the United States Department of Agriculture Rural Urban Commuter Area Codes (RUCA) using zip code. We then combined 5-Year 2012 to 2016 American Community Survey (ACS) Summary File data on the percent of the population earning less than 200% poverty level with the ABFM data using county Federal Information Processing System (FIPS) codes. We only included FPs who reported providing direct patient care.
The ABFM questionnaire asks FPs a series of questions on demographics (race, ethnicity, and number of years in practice), practice characteristics (practice location, practice ownership), Patient-Centered Medical Home (PCMH) status, clinician specialty mix and provision of services (prenatal care, newborn care, obstetric deliveries), and scope of services provided.
The primary outcome was individual SOP score, described by O’Neil et al in 2014.14 The scale was designed to balance the time demands of FPs related to individual services provided and to compare cohorts of physicians. The SOP score is a scaled score based on the following 22 items of each individual FPs provision of services and procedures: care of children, adolescent medicine, geriatric medicine, adult medicine, school health, emergency care, urgent care, women’s health, hospital medicine, occupational medicine, major surgery, office surgery, orthopedics, postop care, preop care, pain management, palliative care, mental health, sports medicine, deliveries, newborn care, and prenatal care. The score ranges from 0 to 30, with higher scores reflecting a broader SOP. In addition, individual components of the SOP were also examined separately, specifically we included binary measures for the provision of care of children [newborn care, children (≤12 years) and adolescents (13 to 18)], women’s health services [long acting reversible contraception (LARC) insertion or removal, endometrial biopsy, prenatal care and women’s health (yes/no)] select office procedures (casting/splint, joint injection/aspiration, and skin procedures) and other services (pain management, inpatient care and palliative care; provision of acute care, and same day appointments, and extended hours).
Our independent variable was practice setting as reported by respondents to the survey who had to choose among (1) Rural health center (RHC), (2) Academic health center, (3) Federally Qualified Health Center (FQHC), (4) Group practice, (5) Solo practice, (6) Hospital-owned, (7) Managed care, (8) Urgent care center (freestanding urgent care center), (9) Federal (Military, Veteran Administration, Department of Defense and Indian Health Service), (10) Other safety net (Institutional setting (School-based clinic, nursing home, prison and nonfederal government clinic (eg, state, county, city, maternal and child health, etc.), and (11) Other (ambulatory surgical center, public health service, industrial outpatient facility and mental health center).
Covariates included gender, years in practice (1 to 10 years, 11 to 20 years, 21 to 30 years, 31 years or more), race/ethnicity (non-Hispanic White, non-Hispanic Black, non-Hispanic Asian, and Hispanic), region (South, Northeast, Midwest, and West), and rurality of practice location (urban and rural), practice size (solo, small practices with 2 to 5 clinicians, medium practices with 6 to 20 clinicians, large practices with greater than or equal to 20 clinicians), and other practices that did not fit this description), PCMH status (Yes, No, Applying), primary specialty mix (multispecialty yes/no), and proportion of the county population living under 200% Federal Poverty Level (FPL).
Our data set, as mentioned above, is limited to board certified family medicine physicians in the United States, we did not have access to data regarding advanced practice providers such as physician assistants or nurse practitioners.
We used Stata 16.0 for all the analyses (StataCorp). First, we ran descriptive statistics to examine demographic and practice characteristics of the FPs meeting criteria. We then conducted bivariate analysis for the services or procedures provided by type of practice organization. We used c2 test to examine the significant differences in services or procedures across the practice types. Finally, we performed linear regression to identify the factors associated with SOP and calculated mean SOP scores using Stata margins command.
The American Academy of Family Physicians Institutional Review Board deemed the study exempt from full review.
Results
Of the total 25,117 FPs in the analysis sample, 39% were female and 61% were males. Nearly 75% of the FPs were in practice for 11 years or more (Table 1). Almost 40% of them were in group practices, 16.3% in hospital-owned practices and 11.5% practiced independently. Unadjusted linear regression results (Table 2) showed that the widest SOP for FPs was seen in RHCs (SOP score 17.7, 95% Confidence Interval [CI] 17.5 to 17.9), followed by academic health centers (16.6, 95% CI 16.4 to 16.7), FQHCs (15.9, 95% CI 15.8 to 16.1), and group practices (15.8, 95% CI 15.8 to 15.9). The FPs in urgent care clinics, Federal clinics, other safety net clinics and “Other” had the narrowest SOP with mean SOP score of 14.0 or less. Even after adjusting for the demographic and practice characteristics, FPs in rural health centers had the highest SOP scores, followed by academic health centers.
Distribution of Demographic and Practice Characteristics of Family Physicians in the Analysis
Unadjusted and Adjusted Mean Individual Scope of Practice (SOP) by Practice Organization*
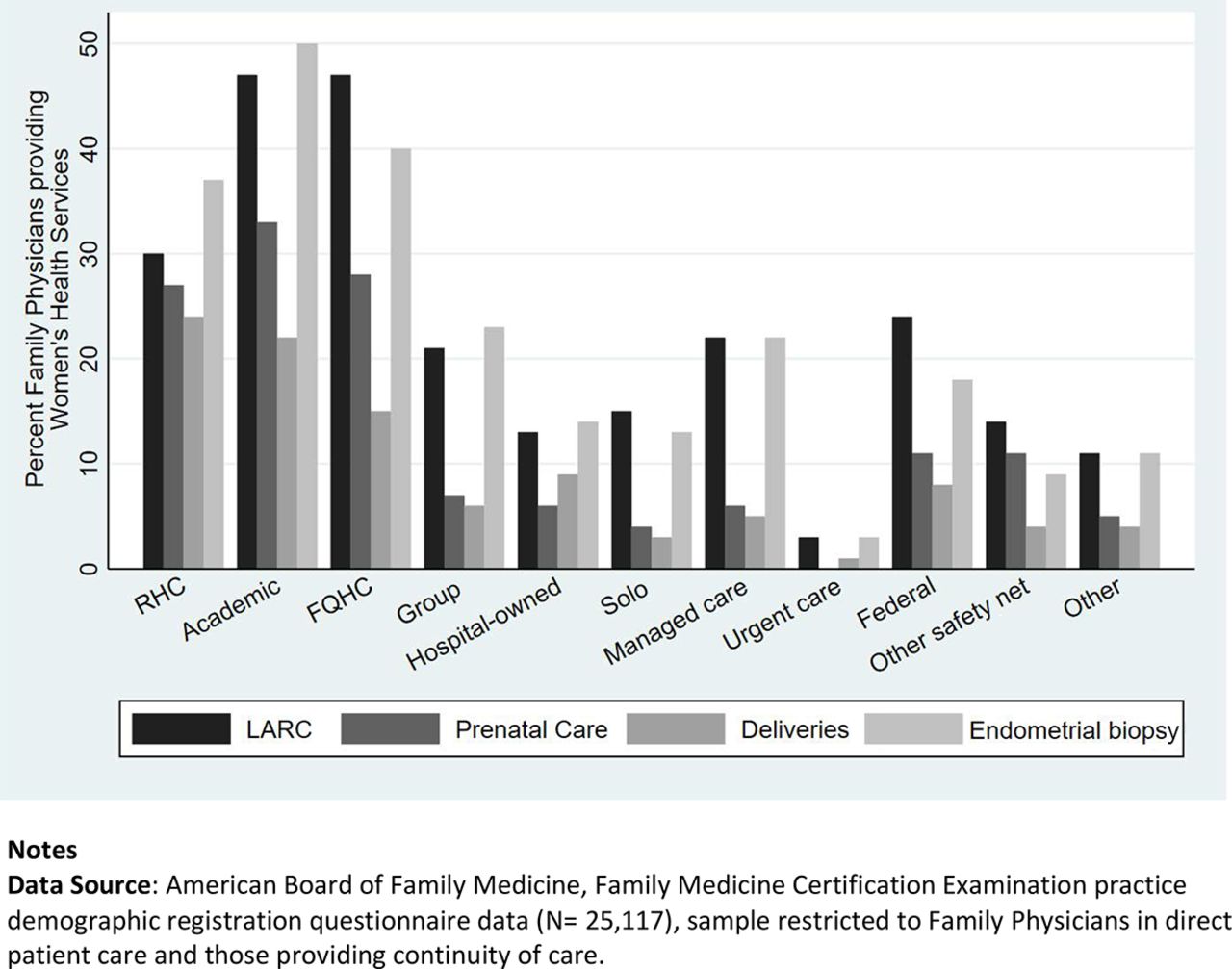
When looking specifically at the individual service components that compose the SOP score, higher rates of FPs in FQHC’s and academic practices were providing a women’s health service except for deliveries, whereas more FPs in rural health centers were providing obstetric services (24%). Almost 50% of FPs at the FQHCs and academic practices were providing some aspects of women’s health care including long-acting reversible contraception (47%), prenatal care (28% and 33%, respectively) and endometrial biopsies (40% and 50%, respectively). (Figure 1).

Proportion of family physicians reporting provision of women’s health services. Abbreviations: RHC, Rural Health Center; AHC, Academic Health Center; FQHC, Federally Qualified Health Center.
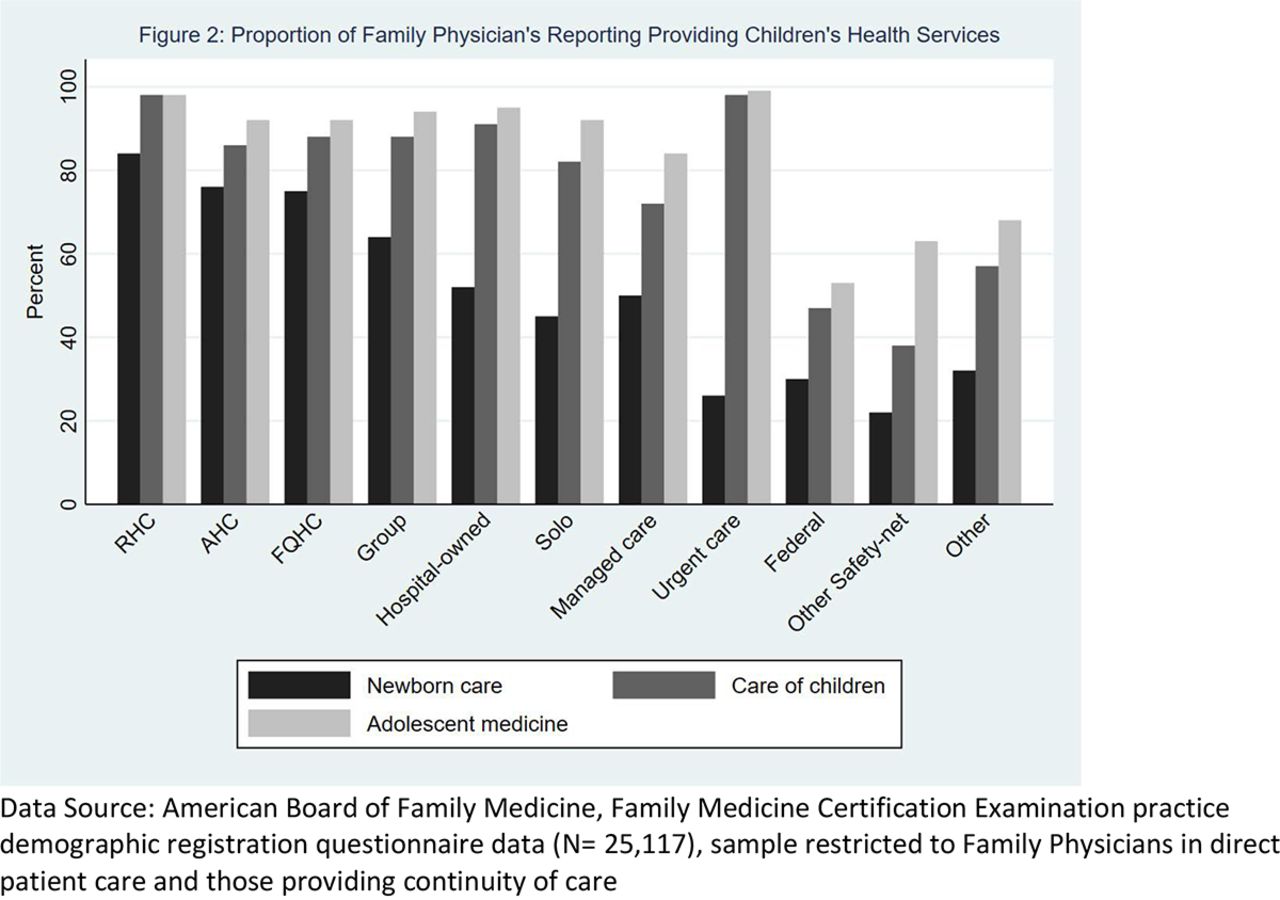
The proportion of FPs providing newborn care was highest in RHCs and lowest in the urgent care setting (85%, vs 26%), (Figure 2) The proportion of FPs taking care of children was highest in RHCs and lowest in the other safety net category (98% vs 38%).

Proportion of family physicians reporting providing children’s health services. Abbreviations: RHC, Rural Health Center; AHC, Academic Health Center; FQHC, Federally Qualified Health Center.
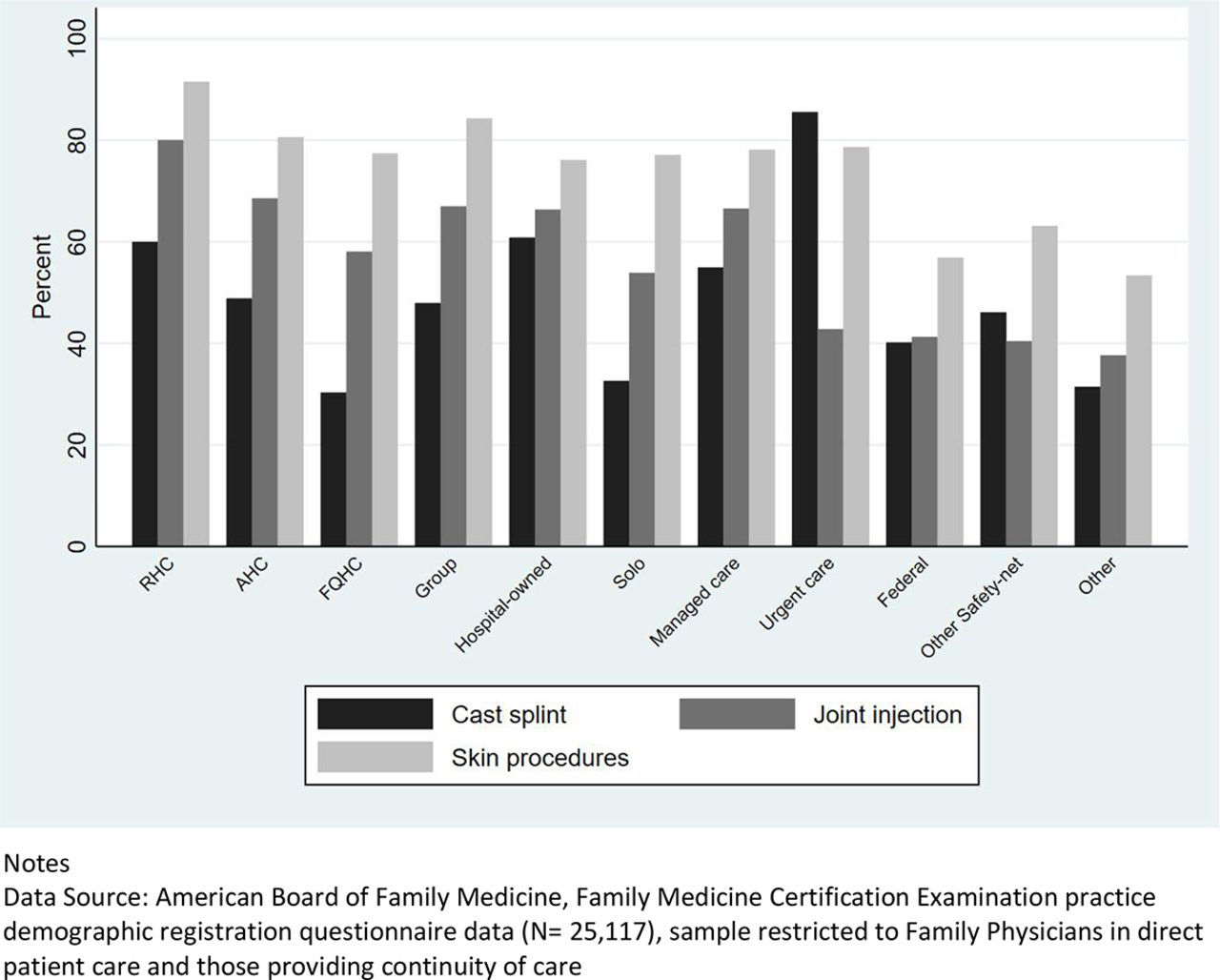
Office-based procedures, such as casting, was highest among FPs practicing in urgent care clinics, followed by FPs practicing in RHCs, and academic health centers, and group practices. A higher proportion of FPs in RHCs provided joint injections or aspiration and skin procedures than FPs in other practice organizations (Figure 3). More FPs in RHCs also provided other services such as pain management, hospital medicine, and palliative care (Appendix Table 1). Most FPs reported working in practice types with same day appointments and extended hours (Appendix Table 2).

Proportion of family physicians reporting performing select procedures. Abbreviations: RHC, Rural Health Center; AHC, Academic Health Center; FQHC, Federally Qualified Health Center.
Discussion
This study demonstrated that there is an association between practice type and SOP of FPs. Those who worked at RHCs and academic clinics were found to have the widest SOP based on overall SOP score, whereas those who worked in managed care, Federal or “other” types of practices had the narrowest scope. This is a trend that has been identified in prior studies which found that FPs whose main practice type was part of an academic teaching unit was associated with a broader scope of practice.12 Academic Centers require attendings to have a wide range of skills to provide a full scope of family medicine education.
Managed care organizations, urgent care, and Federal practices consistently had the narrowest SOP based on SOP scores of 15.0, 14.1, and 13.8, respectively. FPs in managed care practices and federal clinics had some of the lowest rates of providing care to children at 72% and 47%, respectively, whereas those in other safety net clinics had the lowest rates of caring for newborns at 22%. The reasons for these narrower scopes vary, and are worth exploring. Previous studies have cited that increasing rates of insured children would contribute to them being seen less frequently at safety-net clinics.15 It is also possible that there is increased use of nurse practitioners in these clinics to see children, whereas many FPs will see the adult patients.16 Given that a large proportion of clinicians employed by the federal government including the Veterans Administration (VA) and the military, it would make sense that the care of children and therefore total SOP would be lower.17 Similarly, because urgent care clinics by definition are not typically structured to provide chronic care services that factor into the SOP score such as women’s health, mental health, and palliative care, their narrower scores are to be expected. For FPs in managed care organizations (MCO) and hospital owned practice, the reasons may be more elusive. The structure of MCOs could influence the ability for FPs to broaden services via contracts for primary care physicians built around a narrow range of services.18 Specifically, in large MCOs, children and women might be diverted to pediatricians and gynecologists for primary care services that a family medicine physician could provide. Physicians have cited losing pediatric patients when organizational leadership opened a dedicated pediatric clinic.9 Furthermore, payment models within MCOs such as monthly capitation rates might also disincentivize physicians from offering patients wide range of services that consume more time in an already busy schedule.19
Finally, the impact of consolidation on SOP cannot be overlooked. Consolidation of practices and physicians into larger health systems has been increasing in recent years.20 Consolidation has led to an increase in high cost, low quality care, that could be connected to a more narrow SOP that requires more referrals to highly reimbursed specialists within the same systems.21,22 These practice types saw a uniform drop in the care for newborns, highlighting the negative effect of consolidation on services FPs can provide. Consolidation could explain the difference seen between group independent practices, which had a narrower scope compared with solo physicians. Regardless of the reasons, these settings diminish the total availability of primary care services delivered by broadly trained primary care specialists at a time when the primary care workforce to population ratios seem to be in decline.23
When looking specifically at women’s health care, FPs at FQHCs, RHCs, and academic centers are providing more comprehensive women’s health care than FPs at hospital-owned, independently owned, or managed care organizations. FQHCs are known for the wide range of support services for patients, especially being a major source of primary care for women24. Furthermore, it may be that a higher proportion of FPs in FQHCs provide these services for women because their patients, who are typically underinsured or uninsured, have less access to specialists to provide this care.25,26 The finding that there are a higher proportion of FPs who provide deliveries in RHC as compared with all other settings is not surprising and is in line with other studies examining FPs who provide deliveries.27
There are several limitations to discuss. Because this study is based on self-reported survey data, we are unable to know if an FP actually provides the services they reported and what volume of these services is being provided. We were able to differentiate statistically significant differences between scope of practice scales but do not have a good understanding of the practical difference. Research has shown that, in most circumstances, the threshold for a clinically significant difference is approximately half a standard deviation (S.D.)28, which for this study was approximately 1.5 points on the SOP scale with a mean of 15.3 and a S.D. of 2.9. We attempted to control for multiple variables but recognize that there are other variables such as clinic or health system resources that we cannot control for. Financial considerations likely contribute to changes in scope of practice including malpractice insurance, reimbursement models and volume of procedures. In addition, our data set does not include advanced practice professionals, and this would be important research in the future to see if similar trends are seen among physician assistants and nurse practitioners.
Our study demonstrates that a barrier to providing broad scope of practice may be due to practice organization type. More research is needed to better identify why these trends are happening and action is needed to correct any barriers to maintaining the depth and breadth of family medicine. New graduates are and should be positioned for a wide scope of practice because research has shown that a physician’s scope of practice generally narrows as her/his career progresses.29 For policy makers, health systems and practices, this study shows that RHCs and academic centers demonstrate good investments for training and using the full scope of FPs. Maintaining a wide scope of practice could be an important building block in achieving better outcomes at lower costs while improving the patient and provider experience.
Proportion of Family Physicians Providing Other Care Including Pain Management, Hospital Medicine, and Palliative Care
Proportion of Family Physicians Provision of Other Services
Notes
This is the Ahead of Print version of the article.
This article was externally peer reviewed.
Funding: None.
Conflict of interest: None.
To see this article online, please go to: http://jabfm.org/content/36/1/000.full.
- Received for publication May 10, 2022.
- Revision received September 16, 2022.
- Accepted for publication September 20, 2022.




{kind=link}
{kind=link}
{kind=link}