
Article Figures & Data
Figures
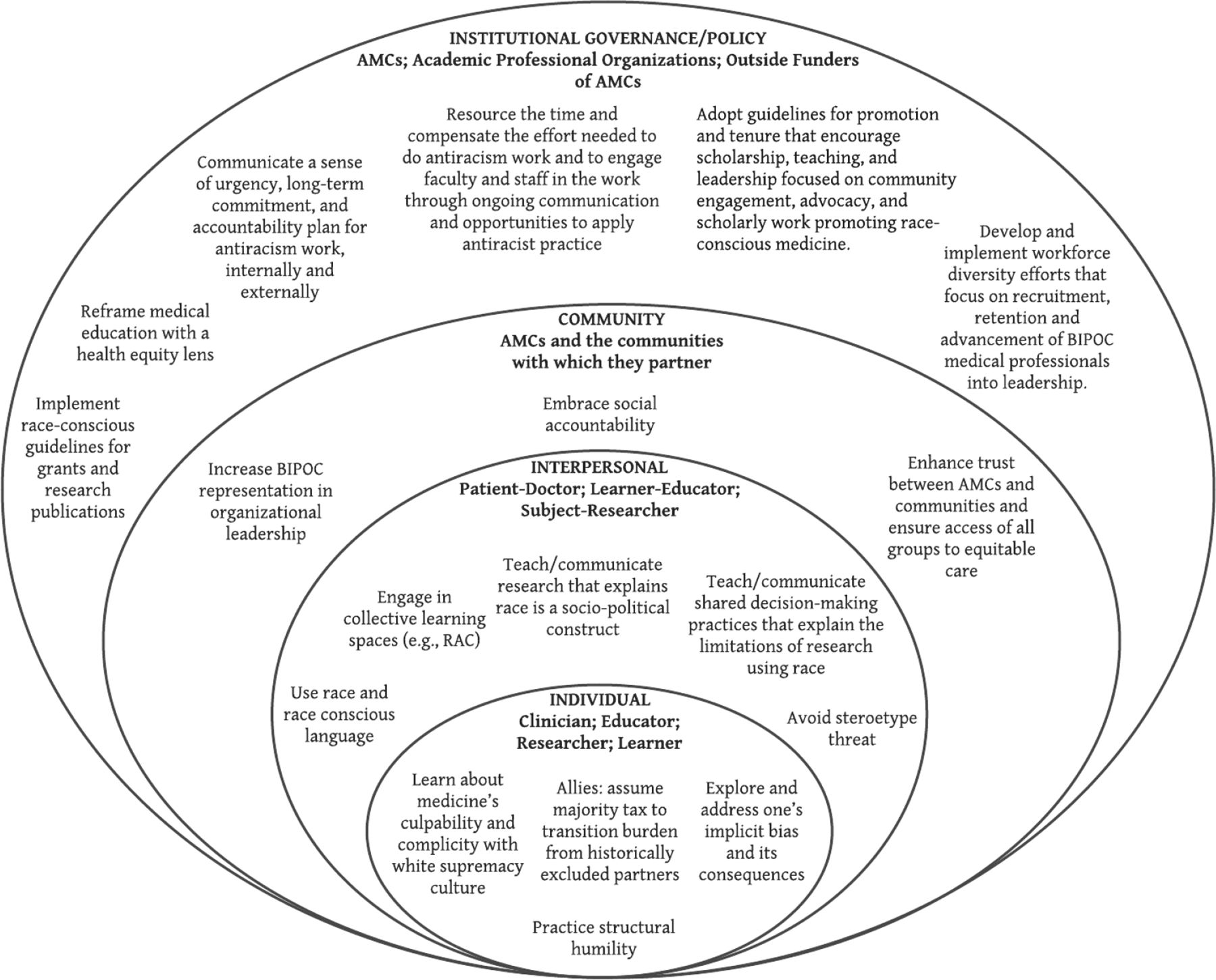
- Figure 1.
A Socioecological model for addressing race in academic medicine. Abbreviations: AMC, academic medical centers; RAC, racial-affinity caucusing.

Tables
Core Concepts Examples INDIVIDUAL
(Clinician; Educator; Researcher; Learner)Learn and unlearn medicine’s culpability and complicity with white supremacy culture22,23,24 Individuals should educate themselves on the historical injustices that have occurred in medicine and seek opportunities to dismantle policies and practices rooted in white supremacy. Center learning from BIPOC scholars using a transdisciplinary context (e.g., law, sociology, history). Explore, confront, and seek tools to begin addressing one’s implicit bias and the inequitable consequences associated with it25 Take an implicit bias test, such as the Harvard Implicit Association Test, to increase one’s awareness of implicit bias and do the requisite work to prevent causing harm. Use race- and racism-conscious language26 Learn not to describe and ascribe people to a single identity such as “minorities” or “disabled”, but rather “people from historically marginalized racial and ethnic groups” or “people with disabilities.”
Broaden your understanding of and appreciate the intersectionality of multiple identities that people hold.Practice structural humility27 Appreciate and acknowledge the wisdom and teachings from historically marginalized and systemically excluded communities. Center the voices of, listen to, and learn from BIPOC communities. Allies, accomplices and co-conspirators should assume a “majority tax”28 to shoulder and transition some of the burden off of historically marginalized and systemically excluded stakeholders Paying the “majority tax” requires accepting the discomfort, energy, and socioeconomic capital required to acknowledge and leverage white privilege.
Examples include:relinquish power/leadership roles so that minoritized populations may advance.
leverage bestowed power to highlight racist practices and ideology in medicine.
approach decision-making (medical and policy) with an antiracist equity lens.
INTERPERSONAL
(Patient-Doctor; Learner-Educator; Subject-Researcher)Do the critical work by engaging in collective learning spaces such as caucusing29 Facilitate and support caucusing within affinity groups to help with collective healing, learning/unlearning, and knowledge and skills building within one’s own identity group. Avoid teaching or communicating research that includes racial/ethnic descriptive health inequities without explicit explanation that race is a socio-political construct30, 31 Discuss the implications of race versus racism when teaching about racial ethnic health differences and discussing research findings. Avoid stereotype threata: i.e., Consider the context in which people will be “threatened” by being reminded of a disadvantaged identity32 Remove portraits of leadership that showcase all white deans and chairs lining medical school hallways. Cultivate spaces of belonging by sharing photos of BIPOC leaders, staff, educators, learners, and community members. Engage and teach shared decision-making practices that explain the limitations of research using race. Instead amplify race as a sociopolitical construct and proxy for socioeconomic status or racism33 Openly discuss race-based calculators with patients and learners; specifically discuss how they may affect patients’ diagnoses, treatment options and management plans. COMMUNITY/POPULATION
(AMCs and the communities they partner with)Embrace social accountability33 Cultivate and deepen relationships with the community. Amplify strengths of the community and address their collective needs. Center community voice in meetings where decision-making occurs. Community advisory boards should hold research and workforce development accountable to the community’s needs. Honor the wisdom and work of community members through funding/honorariums. Enhance trust and assure access Hire community health workers to elevate community voice in clinical care, education, and research.
Invest in and advocate for community organizations doing antiracism work.
Support leaders of and advocates for marginalized communities with tangible resources that include not only money, but also AMC’s time, expertise, connections/networks, and power.
Increase BIPOC representation in organizational leadership28 Establishing leadership term limits may allow BIPOC voices to shape curricula, prioritize issues that impact minoritized communities, allocate funding and resource priorities, and determine inclusive policies. INSTITUTIONAL/GOVERNANCE/POLICIES
(AMCs; Academic Professional Organizations; Outside Funders of AMCs)Implement race-conscious guidelines for grants and research publications6,30,31 Assure there is: explicit criteria for why race and ethnicity are being used as variables in research34
collection of biological and socioeconomic variables
examination and discourse when whiteness is used as a reference value
intention and deliberate action to not use whiteness as reference value
application of an equity lens to research design and clinical implications35,36
opportunity for research subjects to self-identify their demographic information to include qualitative descriptions of their known genetic ancestry
Reframe medical education with a health equity lens Assure there is: standardized language to appropriately describe race/ethnicity
avoidance of language and content that pathologizes race explication of structural determinants of health and health equity, including racism when discussing disproportionate disease prevalence among different populations, rather than attributing to race29
elimination of the use of race-corrected algorithms and replace with more equitable alternatives5
Leadership communicates a sense of urgency, long-term commitment, and accountability plan for antiracism work, internally and externally Disseminate antiracism messaging in regular newsletters/communications from leadership, including opportunities for antiracism engagement and training; highlight both short and long-term antiracism goals/achievements; and elevate BIPOC voices. Provide metrics of accountability. Resource time and compensate effort needed to do antiracism work. Engage faculty and staff in antiracism work through ongoing communication and opportunities to apply antiracist practice Provide FTE allocation and compensation for those engaged in antiracism work. Revise guidelines for promotion and tenure to encourage scholarship, teaching, and leadership focused on community engagement, advocacy, and scholarly work promoting race-conscious medicine38, 39 Adjust and clearly define requirements for promotion and tenure to include scholarship, teaching, community engagement, institutional service, and mentorship focused on diversity, equity, inclusion, antiracism, advocacy for all faculty, not just BIPOC faculty. Develop and implement workforce diversity efforts by academic institutions that focus on recruitment, retention and advancement and promotion of BIPOC medical professionals into leadership positions, especially those underrepresented in medicine40, 41,42, 43 Set metric goals for clinician and faculty representation to reflect the demographics of the patients they work with and for, and the AMC’s surrounding geographic community. Focus on advancing and promoting BIPOC faculty into leadership positions that confer both voice and power to implement and sustain change. Abbreviations: BIPOC, Black, Indigenous, and People of Color; AMC, academic medical centers; FTE, full-time equivalent.
↵a Stereotype threat refers to the risk of confirming negative stereotypes about an person’s racial, ethnic, gender, or cultural group which can create high cognitive load and reduce academic focus and performance. The term was coined by the researchers Claude Steele and Joshua Aronson.44




{kind=link}