
Article Figures & Data
Figures
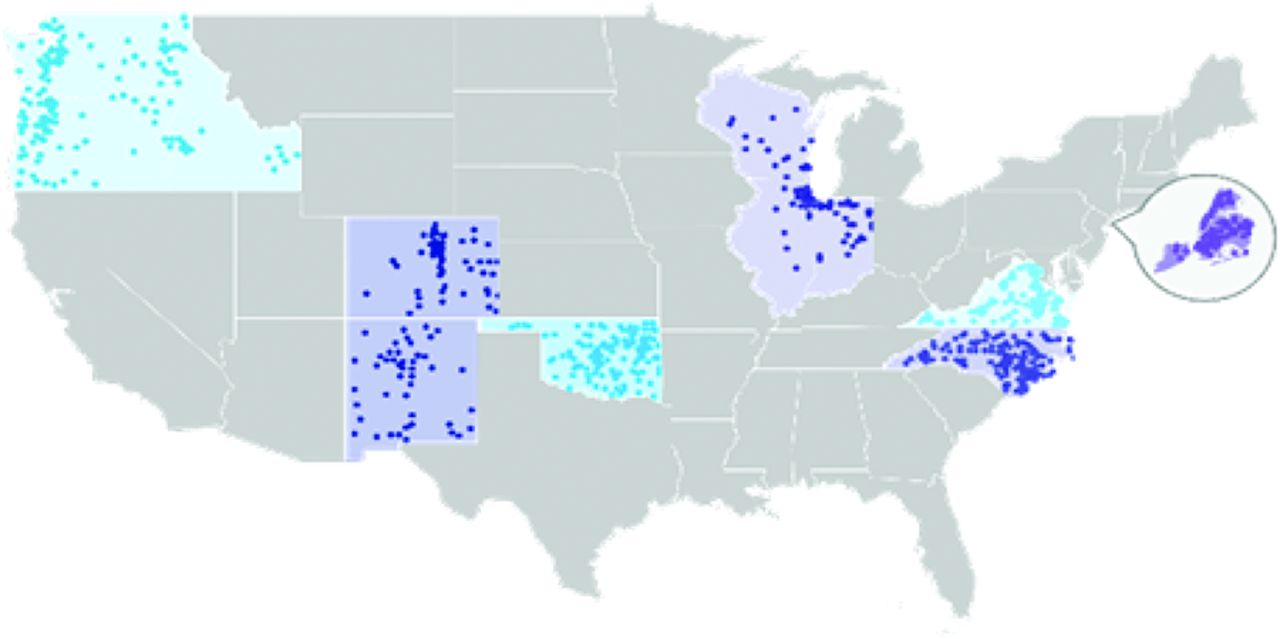
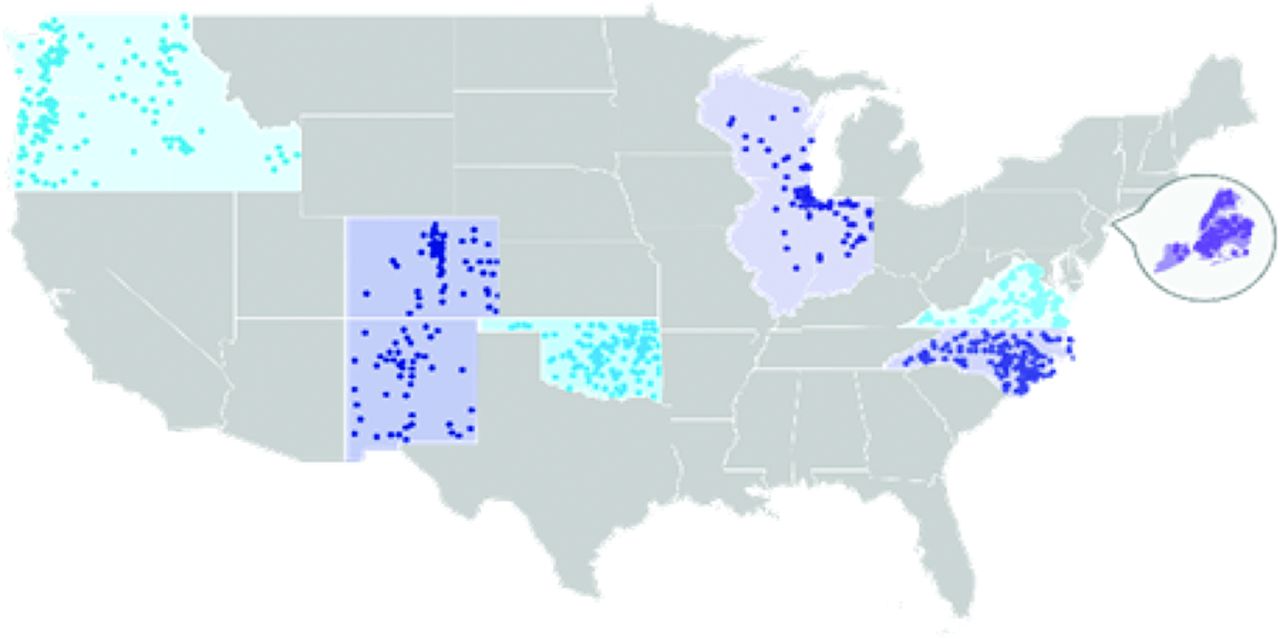
- Appendix Figure 1.
Map of EvidenceNOW cooperatives.
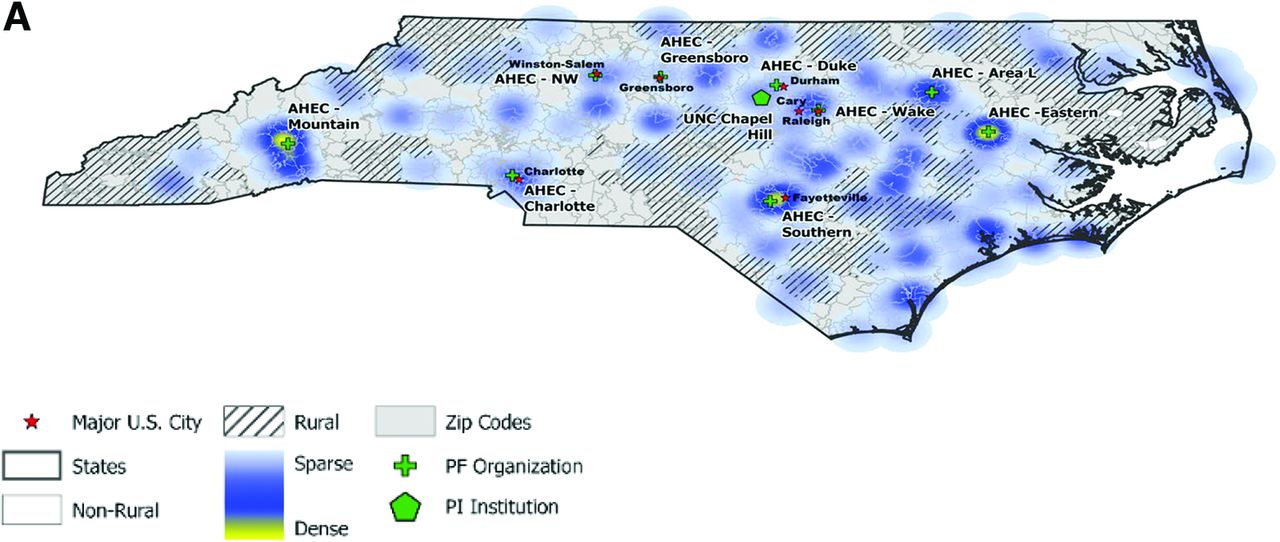
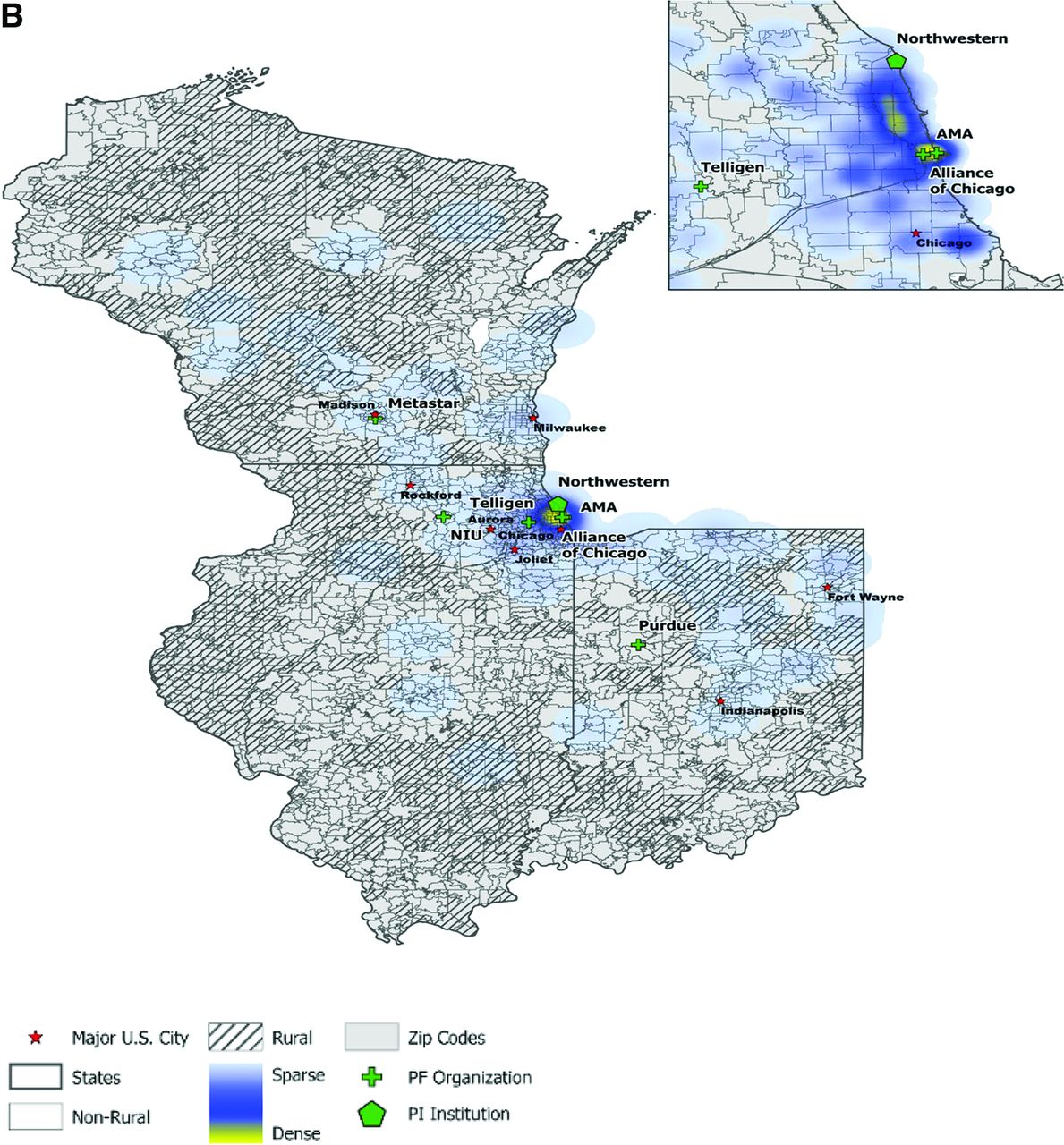
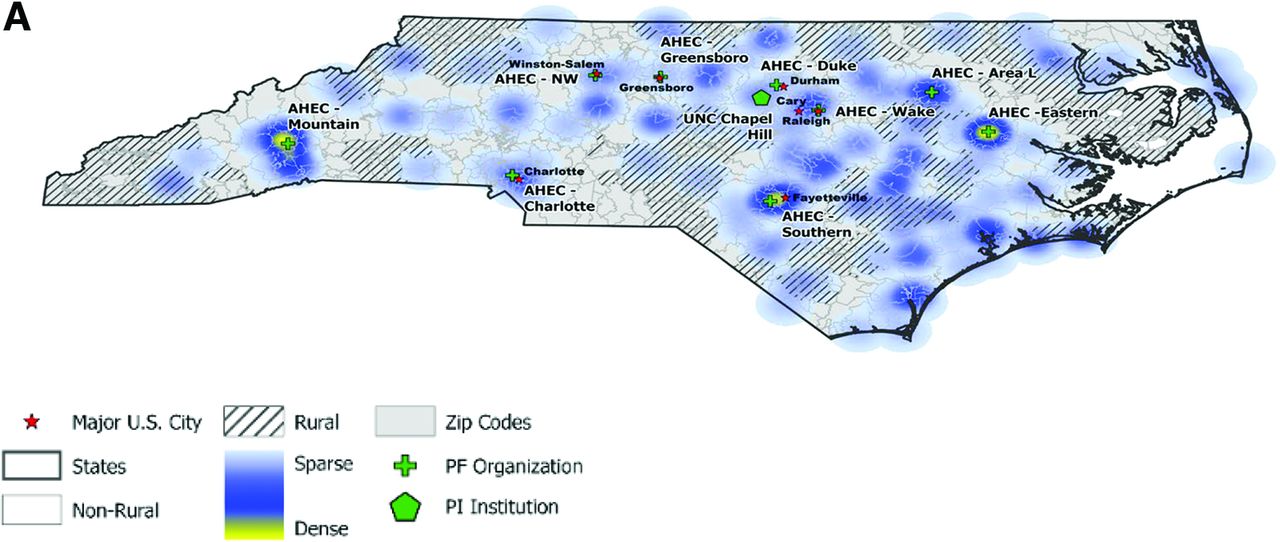
- Appendix Figure 2.
EvidenceNOW recruitment heat maps comparing two cooperatives, (A) One with high and (B) One with low experience and prior infrastructure investment.
The figures below depict two Cooperative regions with major citied marked with a red star. Light grey areas depict regions classified as non-rural; hatched lines depict regions classified as rural. Cooperative organizational locations are also indicated – the home institution of the Principal Investigator is marked with a green hexagon and the location of each Practice Facilitator Organization is marked with a green cross. These maps also overlay the density of practices recruited by each Cooperative – with regions where fewer practices were engaged indicated in light blue and regions where more practices were engaged indicated in yellow.
Tables
- Table 1.
Description and Assignment of Cooperative Level of Prior Experience (Independent Variable)

Abbreviations: AHEC, Area Health Education Centers; EHR, electronic health record.
Concept/Definition Measure / How Scored How and when collected Ability to deliver Facilitation Amount of facilitation delivered Total number of hours and months of facilitation a Cooperative delivered to each practice Collected by each Cooperatives’ facilitators.
Collected from facilitators first contact with practices to their last contact.Clinical Capacity Adaptive Reserve (AR) 14-item measure assessing practice capacity for adapting to change; individual practice members assessed experience of organization’s communication, teamwork, mindfulness, leadership, heedful interaction, sensemaking, work environment, learning culture and trust. Scores from (0 to 1). Collected by survey distributed to clinical practice members by Cooperatives.
Collected at baseline and at end of the interventionChange Process Capacity Questionnaire (CPCQ) 14-items of CPCQ; we selected the measures focused on the extent to which practices used different types of quality improvement strategies for cardiovascular disease prevention. Scores from (−28 to 28). Collected by survey that was completed by lead clinician or office manager.
Collected at baseline and at end of the intervention.Clinical Quality Aspirin Therapy (CMS164v4) Percentage of patients 18 years of age and older with ischemic vascular disease with documented use of aspirin or another antithrombotic. Scored from (0 to 100%). Collected by Cooperatives through EHR-generated reports, EHR chart review, and health information exchange reports.
Quarterly rolling 12-month performance on each measure at the practice levelBlood Pressure Management (CMS165v4) Percentage of patients 18 to 85 years of age with a diagnosis of hypertension whose BP was adequately controlled (<140/90 mm Hg). Scored from (0 to 100%). Cholesterol Management (CMS347v1) Percentage of adult patients at high risk for a cardiovascular event who were using or prescribed statin therapy. Scored from (0 to 100%). Smoking Cessation (CMS138v4) Percentage of patients aged 18 years and older who were screened for tobacco use one or more times within 24 months AND who received cessation counseling, if identified as a tobacco user. Scored from (0 to 100%). For the ABCS data, we reviewed data, including trajectories of change over time, computing descriptive statistics related to variability and removing practices that exhibited extreme, implausible jumps or otherwise implausible trajectories that could not be addressed by Cooperatives. Practices were also removed that had submissions with non-standard measurement periods. For all other variables and outcomes, data quality checks were performed in an iterative manner, with our team identifying anomalies or irregularities (e.g., excessive missingness, implausible or non-sensical inputs) and Cooperatives addressing those on their end and resubmitting corrected data.
Abbreviations: ABCS, Aspirin, Blood Pressure, Cholesterol, and Smoking; EHR, electronic health record.
Qualitative Data Collected What Was Collected How Were Data Obtained When Were Data Collected Artifacts Documents related to Cooperatives’ work (e.g., grant application, training materials) Obtained from Cooperatives Throughout initiative Online Diaries Platform to share real-time implementation experiences Online text entries from Cooperative teams prompted by ESCALATES Throughout initiative Field Observation Visits to learn about each Cooperative team, and understand the work they were doing (e.g., startup, recruitment, implementation activities, including observing facilitators work with practices) Fieldnotes, including
observation of 41 facilitators
with 54 unique practicesAugust 2015 – March 2016;
July 2016 – April 2017Semi-structured Interviews Interviewed Cooperative leadership, members of partner organizations, and facilitators to explore start-up and implementation experiences 39 interviews with Cooperative leadership and partners; 89 unique facilitator interviews; 66 interviews with practice members Throughout the initiative Context Assessments Cooperatives completed assessments to provide information about their local contexts, including team’s experience, regional attributes, experiences with recruitment and implementation of external support Two written assessments;
Cooperative teams answered
5 to 6 broad questionsRecruitment and implementation phases Abbreviations: ESCALATES, Evaluating System Change to Advance Learning and Take Evidence to Scale.
Experience Level Low Medium High Cooperative 2 5 4 6 3 7 1 Number of Practices 226 251 209 211 315 263 245 Practice Characteristics, n (col %)
Location1Rural 10 (4.4) 30 (12.0)* 40 (19.1) 46 (21.8) 0 (0.0) 72 (27.4) 37 (15.1)* Large Town 18 (8.0) 5 (2.0)* 54 (25.8) 16 (7.6) 0 (0.0) 76 (28.9) 33 (13.5)* Suburban 3 (1.3) 22 (8.8)* 21 (10.0) 13 (6.2) 0 (0.0) 20 (7.6) 28 (11.4)* Urban Core 195 (86.3) 151 (60.2)* 94 (45.0) 136 (64.5) 315 (98.4) 90 (34.2) 91 (37.1)* Practice Ownership Clinician owned 84 (37.2) 63 (25.1)* 96 (45.9) 72 (34.1) 144 (45.7)* 104 (39.5) 93 (38.0)* Hospital/Health System 59 (26.1) 118 (47.0)* 81 (38.8) 31 (14.7) 1 (0.3)* 75 (28.5) 30 (12.2)* Safety Net2 58 (25.7) 25 (10.0)* 32 (15.3) 90 (42.7) 16 (5.1)* 71 (27.0) 42 (17.1)* Other3 1 (0.4) 2 (0.8)* 0 (0.0) 15 (7.1) 1 (0.3)* 8 (3.0) 5 (2.0)* Practice Size Solo 67 (29.6) 13 (5.2)* 19 (9.1) 43 (20.4) 101 (32.1)* 78 (29.7) 36 (14.7)* 2 to 5 clinicians 103 (45.6) 123 (49.0)* 105 (50.2) 124 (58.8) 34 (10.8)* 137 (52.1) 73 (29.8)* 6 to 10 clinicians 34 (15.0) 33 (13.1)* 36 (17.2) 34 (16.1) 13 (4.1)* 29 (11.0) 26 (10.6)* 11 + clinicians 22 (9.7) 28 (11.2)* 49 (23.4) 4 (1.9) 7 (2.2)* 14 (5.3) 35 (14.3)* Patient Characteristics ≥50% patients over 40 years old 136 (60.2) 129 (51.4)* 119 (56.9)* 0 (0.0)* 113 (35.9)* 160 (60.8) 174 (71.0)* ≤50% patients classified as white 91 (40.3) 57 (22.7)* 16 (7.7)* 33 (15.6) 87 (27.6)* 54 (20.5) 43 (17.6)* >30% Medicaid patients 77 (34.1) 13 (5.2)* 45 (21.5)* 78 (37.0) 51 (16.2)* 72 (27.4) 15 (6.1)* >10% uninsured patients 59 (26.1) 41 (16.3)* 27 (12.9)* 68 (32.2) 10 (3.2)* 63 (24.0) 43 (17.6)* Notes: Percentages may not add up to 100% due to missing data. Variables with >15% missing data indicated with an.* 1Location designation determined using rural-urban commuting area codes. 2Safety net includes Federally Qualitied Health Centers, rural health clinics, Indian Health Services clinics, and other federally owned clinics. 3Other ownership includes nonfederal, private/non-clinician, and those indicating “other” without specifying an ownership type.
- Table 5.
Facilitation Outcomes, Cardiovascular Disease Preventive Services Delivery Performance, and Practice Capacity Outcomes at Baseline and Post-Intervention, Overall, and by Level of Cooperatives’ Experience
Level of Cooperatives’ Experience Overall Low Medium High Mean (SD) Mean (SD) Mean (SD) Mean (SD) Hours of Facilitation 18.1 (18.4) 6.2 (5.1) 18.9 (17.0) 26.5 (21.9) Difference Between Groups Reference +12.7 +20.3 Months of Facilitation 7.2 (3.5) 4.0 (2.1) 8.2 (3.2) 8.4 (3.3) Difference Between Groups Reference +4.2 +4.3 Aspirin (%) Baseline 63.9 (24.2) 67.5 (23.9) 69.6 (19.2) 48.7 (26.5) Follow-up 66.6 (22.8) 69.4 (24.1) 71.8 (17.2) 53.5 (25.4) Difference from baseline to follow-up +2.7 (8.5) +1.9 (6.7) +2.2 (9.3) +4.8 (8.5) Blood pressure (%) Baseline 64.7 (13.7) 64.8 (15.6) 66.1 (13.2) 62.0 (12.1) Follow-up 66.5 (13.6) 67.2 (14.6) 67.5 (13.4) 64.1 (12.4) Difference from baseline to follow-up +1.8 (6.5) +2.4 (5.6) +1.4 (6.8) +2.1 (6.9) Cholesterol (%) Baseline 61.9 (19.3) 65.7 (19.8) 66.4 (13.0) 48.3 (21.3) Follow-up 65.8 (17.7) 68.2 (19.3) 68.9 (12.5) 56.8 (19.9) Difference from baseline to follow-up +3.9 (7.4) +2.5 (6.2) +2.5 (6.2) +8.5 (8.8) Smoking (%) Baseline 60.0 (32.4) 79.4 (21.2) 61.2 (30.9) 37.9 (30.8) Follow-up 65.6 (30.8) 82.0 (20.5) 66.6 (29.2) 47.0 (32.3) Difference from baseline to follow-up +5.6 (11.3) +2.6 (6.9) +5.4 (11.8) +9.1 (12.9) Adaptive Reserve (AR) (score) Baseline 0.703 (0.118) 0.678 (0.118) 0.710 (0.117) 0.715 (0.117) Follow-up 0.721 (0.124) 0.705 (0.129) 0.734 (0.115) 0.719 (0.128) Difference from baseline to follow-up +0.018 (0.117) +0.027 (0.122) +0.024 (0.112) +0.004 (0.118) CPCQ (score) Baseline 8.8 (12.6) 10.7 (12.1) 7.9 (12.7) 8.3 (12.7) Follow-up 14.9 (9.3) 15.7 (10.2) 14.0 (8.8) 15.3 (9.1) Difference from baseline to follow-up +6.1 (13.8) +5.0 (14.5) +6.1 (13.4) +7.0 (13.7) Notes: The table shows mean baseline and post-intervention levels, and standard deviations of ABCS, AR, and CPCQ as well as levels of hours and months of facilitation during the intervention for all practices in the sample as well as stratified by Cooperative level of experience. For clinical measures, preliminary data quality assessment revealed large increases or decreases for some practices. To eliminate the influence of such outliers, we excluded practices with outcome change below the 5th percentile or above the 95th percentile from all our analysis. For overall pre-post ABCS, AR, and CPCQ changes, bold denotes statistical significance at the 5% level.
Sources: EvidenceNOW EHR records.
Abbreviations: SD, standard deviation; CPCQ, Change Process Capacity Questionnaire; ABCS, Aspirin, Blood Pressure, Cholesterol, and Smoking; EHR, electronic health record.
- Table 6.
Changes in Outcomes from Baseline to Follow-up by Level of Cooperative Experience
Level of Cooperatives’ experience Low Medium High Coef. (p-Value) Coef. (p-Value) Coef. (p-Value) Hours of Facilitation Unadjusted: Difference Between Groups Reference +12.68 (0.180) +20.33 (0.039) Adjusted: Difference Between Groups Reference +13.96 (0.205) +24.12 (0.022) Months of Facilitation Unadjusted: Difference Between Groups Reference +4.20 (0.036) +4.33 (0.002) Adjusted: Difference Between Groups Reference +4.37 (0.029) +4.86 (<0.001) Aspirin (%) Unadjusted Reference +0.33 (0.885) +2.89 (0.081) Adjusted: Full Sample Reference −0.29 (0.897) +2.14 (0.179) Adjusted: Practices below the median at baseline Reference +2.59 (0.604) +2.05 (0.683) Adjusted: Practices above the median at baseline Reference −1.67 (0.054) −0.16 (0.848) Blood pressure (%) Unadjusted Reference −0.99 (0.270) −0.19 (0.852) Adjusted: Full Sample Reference −0.87 (0.560) +0.64 (0.582) Adjusted: Practices below the median at baseline Reference −1.02 (0.684) +0.61 (0.791) Adjusted: Practices above the median at baseline Reference −0.96 (0.155) +0.02 (0.978) Cholesterol (%) Unadjusted Reference −0.02 (0.991) +5.99 (0.014) Adjusted: Full Sample Reference +0.40 (0.842) +4.59 (0.142) Adjusted: Practices below the median at baseline Reference +1.85 (0.682) +3.33 (0.527) Adjusted: Practices above the median at baseline Reference −1.07 (0.570) +2.78 (0.069) Smoking (%) Unadjusted Reference +2.73 (0.277) +6.43 (0.003) Adjusted: Full Sample Reference +3.33 (0.245) +7.07 (0.007) Adjusted: Practices below the median at baseline Reference +5.16 (0.462) +3.97 (0.524) Adjusted: Practices above the median at baseline Reference −0.16 (0.953) +5.55 (0.019) Adaptive reserve (score) Unadjusted Reference +0.00 (0.898) −0.02 (0.267) Adjusted: Full Sample Reference +0.00 (0.907) −0.02 (0.260) Adjusted: Practices below the median at baseline Reference +0.021 (0.356) −0.016 (0.513) Adjusted: Practices above the median at baseline Reference −0.006 (0.812) −0.017 (0.286) CPCQ (score) Unadjusted Reference +1.18 (0.367) +2.04 (<0.001) Adjusted: Full Sample Reference +1.93 (0.248) +1.32 (0.346) Adjusted: Practices below the median at baseline Reference −2.23 (0.493) −2.29 (0.317) Adjusted: Practices above the median at baseline Reference +1.15 (0.589) +2.92 (0.092) Notes: The table shows unadjusted and adjusted regression estimates and p-values (in parentheses) of differences in outcome changes between Cooperative groups. Practices from Cooperatives with low experience are the reference group. Adjusted estimates are based on regressions that include practice characteristics (practice location; practice ownership; practice size; practice patient characteristics). Bold denotes statistical significance at the 5% level. All standard errors are clustered at the Cooperative level using bootstrapping.
Sources: EvidenceNOW EHR records and practice survey.
Abbreviations: EHR, electronic health record; CPCQ, Change Process Capacity Questionnaire.
Measure Description Practice location We used information given on zip code to classify practice locations as either Rural, Large Town, Suburban, or Urban Core, based on Rural-Urban Commuting Areas (RUCA) using 2010 Census data. Practice ownership The survey question was “Which of the following best describes your practice’s ownership? (Check all that apply)” The following categories were possible responses: clinician-owned solo or group practice; hospital/health system owned; Health Maintenance Organization (e.g., Kaiser Permanente); Federally Qualified Health Center or look-alike; non-federal government clinic (e.g., state, county, city, public health clinic, etc.); academic health center / faculty practice; federal (military, Veterans Administration, Department of Defense); Rural Health Clinic; Indian Health Service; other (please specify). Based on a hierarchical logic using these responses, including the other-specify response, and in some cases soliciting additional information from cooperatives, we recoded each practice into one of the following: Clinician-owned, Hospital/Health System, Safety Net (including FQHCs, academic health centers, federal, RHS, and IHS) or Other. Practice size The survey asked respondents to choose which of the following best describes their practice’s size: solo practice, 2 to 5 clinicians, 6 to 10 clinicians, 11 to 15 clinicians, or 16 or more clinicians. We recoded the 11 to 15 clinicians and 16 or more clinicians’ categories into one, 11 + clinicians. ≥50% patients over 40 years old The survey asked for the percent of patients at the practice who fell into the following age categories: 0 to 17, 18 to 39, 40 to 59, 60 to 75, and 76 and over. We grouped percentages for the latter three groups into one 40 + percentage, then recoded this summed value into an indicator variable for whether this percentage was at least 50%. ≤50% white patients The survey asked for the percent of patients at the practice who were white, and we recoded this percent into an indicator variable for whether this percentage was at least 50%. >30% Medicaid patients The survey asked for the percent of patients at the practice receiving Medicaid, including those eligible for both Medicaid and Medicare, and we recoded this percent into an indicator variable for whether this percentage was above 30%, representing a high proportion of Medicaid beneficiaries. >10% uninsured patients The survey asked for the percent of patients at the practice who had no insurance, and we recoded this percent into an indicator variable for whether this percentage was above 10%, representing a high proportion of uninsured patients. Number of hours Total number of facilitation hours Number of encounters Total number of facilitation encounters Months with encounter Number of months with a facilitation encounter Abbreviations: FQHCs, Federally qualified health centers; RHS, Rural health services; IHS, Rural health services.
Please rate your level of agreement with the following statements about your practice
Strongly disagree. . . . . . . . 1
Disagree. . . . . . . . . . . . . . . 2
Neutral. . . . . . . . . . . . . . . . 3
Agree. . . . . . . . . . . . . . . . . .4
Strongly agree. . . . . . . . . . .5AR1 Mistakes have led to positive changes here AR2 I have many opportunities to grow in my work AR3 People in our practice actively seek new ways to improve how we do things AR4 People at all levels in this office openly talk about what is and isn’t working AR5 Leadership strongly supports practice change efforts AR6 After trying something new, we take time to think about how it worked AR7 Most of the people who work in our practice seem to enjoy their work AR8 It is hard to get things to change in our practice AR9 This practice is a place of joy and hope AR10 This practice learns from its mistakes AR11 Practice leadership promotes an environment that is an enjoyable place to work AR12 People in this practice operate as a real team AR13 When we experience a problem in the practice, we make a serious effort to figure out what’s really going on AR14 Leadership in this practice creates an environment where things can be accomplished Question 8 was reverse-coded, then responses were rescaled to range from 0 to 1 and averaged to produce the practice-level AR score, ranging from 0 to 1.
Indicate the extent to which you agree or disagree that your practice has used the following strategies to improve cardiovascular preventive care
Strongly disagree. . . . . . . . 1
Disagree. . . . . . . . . . . . . . . 2
Neutral. . . . . . . . . . . . . . . . 3
Agree. . . . . . . . . . . . . . . . . .4
Strongly agree. . . . . . . . . . .5CPCQ1 Providing information and skills-training CPCQ2 Using opinion leaders, role modeling, or other vehicles to encourage support for changes CPCQ3 Changing or creating systems in the practice that make it easier to provide high quality care CPCQ4 Removal or reduction of barriers to better quality of care CPCQ5 Using teams focused on accomplishing the change process for improved care CPCQ6 Delegating to non-clinician staff the responsibility to carry out aspects of care that are normally the responsibility of physicians CPCQ7 Providing to those who are charged with implementing improved care the power to authorize and make the desired changes CPCQ8 Period measurement of care quality for assessing compliance with any new approach to care CPCQ9 Reporting measurements of practice performance on cardiovascular disease prevention measures (such as aspirin for patients at risk for ischemic vascular disease) for comparison with their peers CPCQ10 Setting goals and benchmarking rates of performance quality on cardiovascular disease prevention measures at least yearly CPCQ11 Customizing the implementation of cardiovascular disease prevention care changes to the practice CPCQ12 Using rapid cycling, piloting, pre-testing, or other vehicles for reducing the risk of negative results for introducing organization-wide change in care CPCQ13 Deliberately designing care improvements so as to make clinician participation less work than before CPCQ14 Deliberately designing care improvements to make the care process more beneficial to the patient Reponses were rescaled to range from −2 to 2 and summed to produce the practice-level CPCQ score, ranging from −28 to 28.

In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.