
Abstract
Introduction: The 1985 Hames Consortium convened family medicine researchers to identify outstanding questions in their practice.
Method: In this descriptive review, we collected, codified, and analyzed available literature to describe the availability of evidence to answer these questions.
Results: Of 136 total questions, researchers rated 33 questions as not at all answered (24.2%), 49 questions as somewhat answered (36.0%), 37 as mostly answered (27.2%), and 17 as fully answered – will implement in practice (12.5%). Notably, 2 of the categories with the highest number of total questions, community oriented primary care and the value of comprehensive care, had the highest percentage of unanswered questions.
Discussion: The Hames 100 questions and categories themselves demonstrate the values and purpose of family medicine research and can serve as a powerful tool to discuss the future of family medicine research. The varied questions illustrate the broad scope of interest of family physicians in 1985, which remains just as relevant today. Our findings indicate that relatively few questions were fully answered, with even fewer questions answered in family medicine journals.
- ADFM/NAPCRG Research Summit 2023
- Evidence-Based Medicine
- Family Medicine
- Hames Consortium
- Practice-Based Research
- Research
Introduction
In 1963, the World Health Organization recognized the “particular contribution” family medicine can make to medical research.1 The legacy of family medicine research began even before family medicine was a specialty. From Curtis G. Hames2 to John Fry3,4 to James Mackenzie, Will Pickles, and F. J. A. Huygen, family physicians advance the care of their patients through research.5 Family medicine has made valuable contributions to the practice of evidence-based medicine.6
Family medicine researchers have regularly convened to set a vision for the discipline,5,7 including the Ambulatory Sentinel Practice Network (ASPN) in the 1980s.8 The Curtis G. Hames Lectureship and Professorship Endowment, established in 1981, sponsored the Hames Consortium, an annual meeting to generate innovative ideas for family medicine research.9 These convenings included members from the Study Group on Family Medicine Research, an autonomous group organized and supported by the Society of Teachers of Family Medicine Task Force on Research Status and Needs; North American Primary Care Research Group; American Academy of Family Physicians; College of Family Physicians of Canada; and Family Health Foundation of America.7 The 1985 Hames Consortium convened family medicine researchers to identify outstanding questions in their practice.3 The resulting “100 most important family medicine research questions” (Hames 100) set an ambitious agenda for family medicine researchers.
The purpose of this study was to describe the progress researchers have made toward answering these research questions nearly 40 years later.
Method
In this descriptive review,10 we collected, codified, and analyzed data to describe the availability of evidence to answer the Hames 100. Although these are research questions, we did not isolate them from the context of the practice of family and community medicine. We approached this study through a constructivist lens,11 to recognize that all practicing family physicians practice within unique contexts that are informed by their communities, patients, and hospital systems.
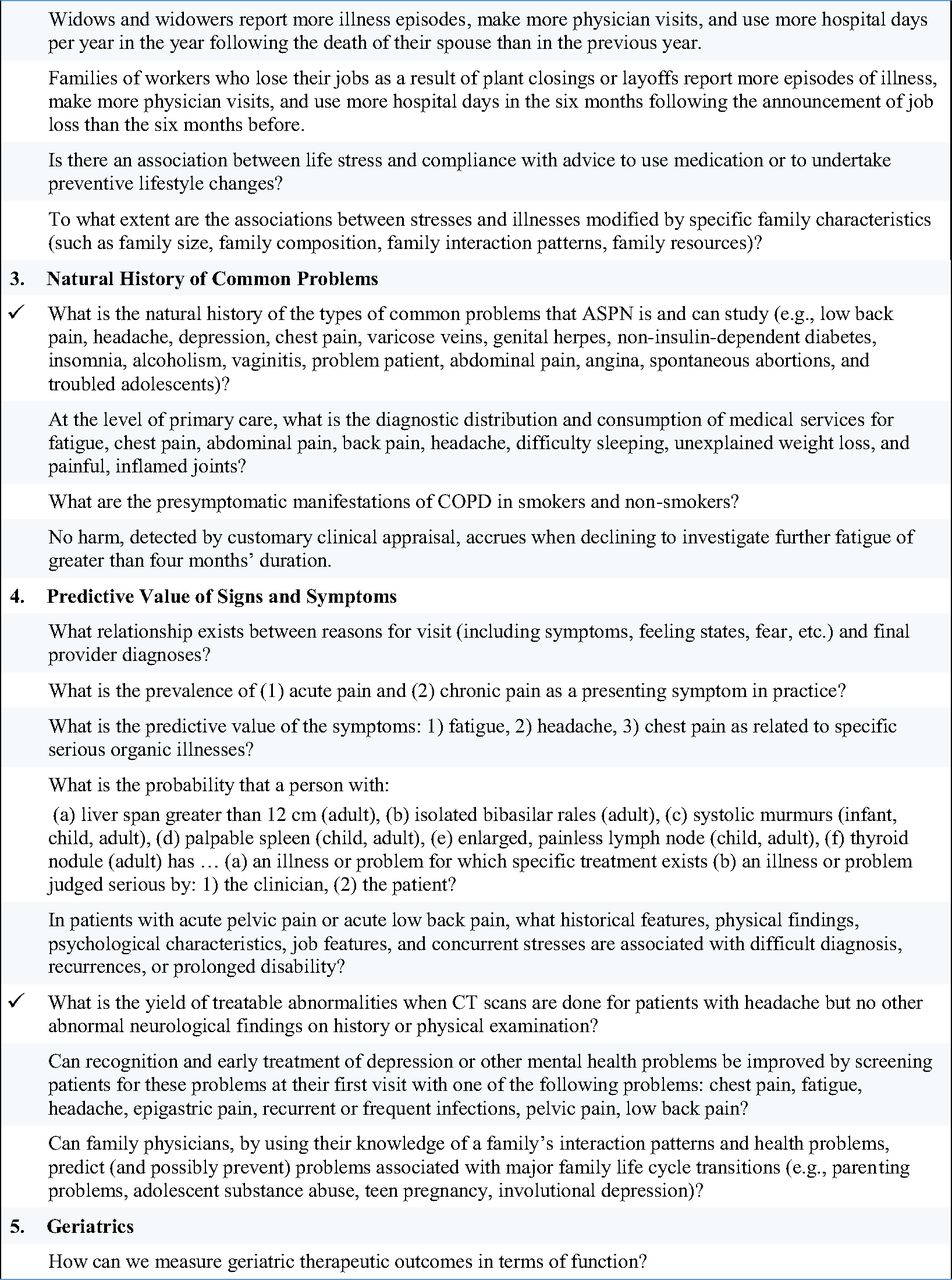
First, we reviewed all questions to clearly define the sample. See Appendix A for a full list of the questions organized by original categories. For multistep questions (eg, What percent of young men have had a physician encourage/teach testicular self-examination? What percent of these young men do it?), we divided the question into 2 or more questions. Then, we reviewed all questions for clarity and structure. We excluded questions that were: not written as a clear question or hypothesis (eg, Use of computers to manage potential drug interactions within the active patients of a practice); overall too nebulous (eg, what constitutes a community?); had ambiguous concepts that we could not fairly operationalize without knowing the writer’s intent (eg, … with heavy business-leader input …); or too specific to answer outside of the time when it was written (eg, … total cost of readily available mammography of $40.00 is sufficient to …).
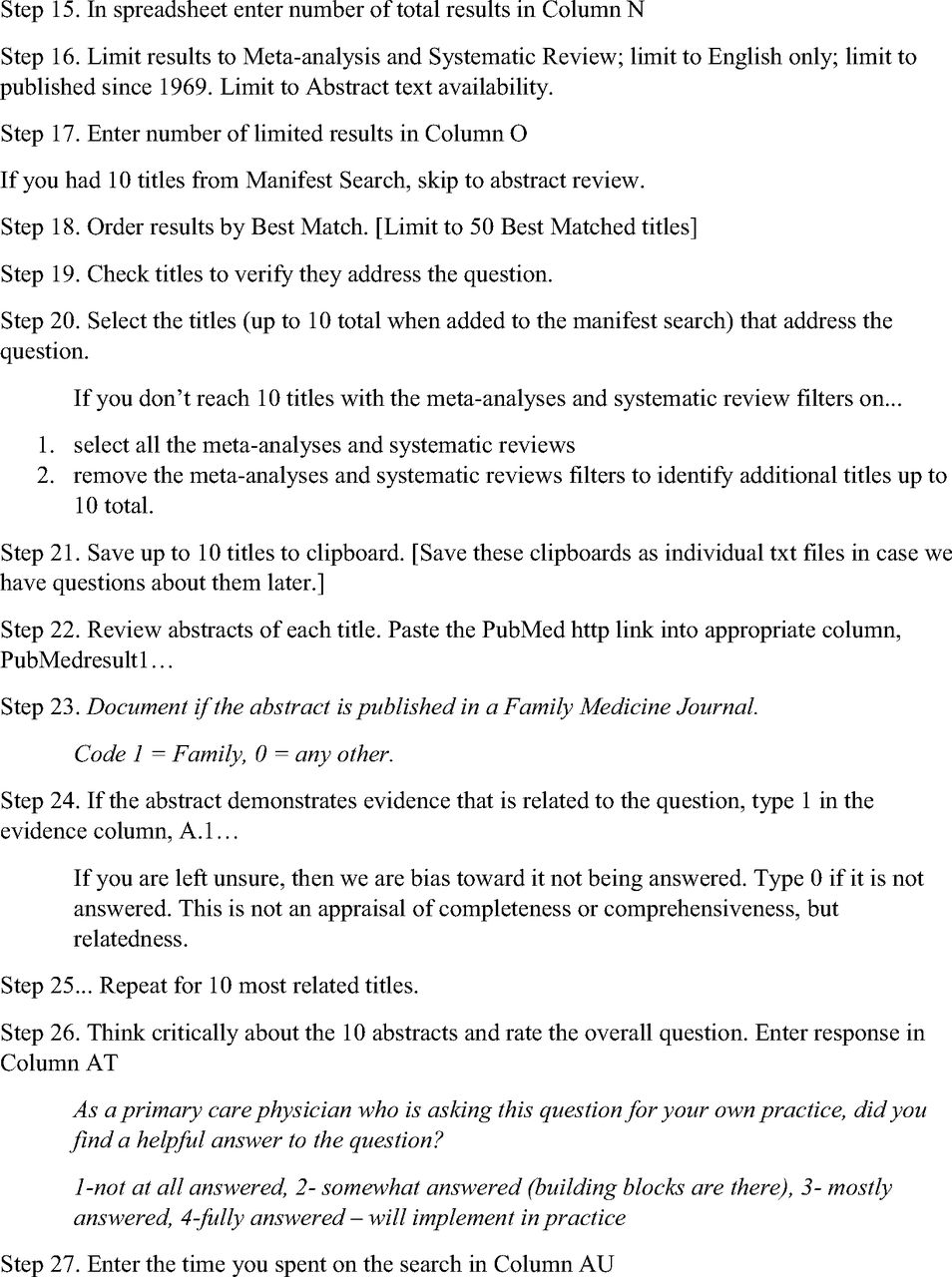
As we developed the method, we positioned ourselves as family physicians – who we imagined were the end users for whom the Hames 100 questions were written. Family physicians often seek answers to clinical questions between patient appointments or amid documentation through lunch or after hours. Our goal was to replicate what an average practicing family physician may do. Four medical students who plan to become family physicians acted as data extractors/coders. We selected students to ensure that the coders did not already know if the questions had been answered. The search strategy was limited to PubMed and prioritized meta-analyses and systematic reviews. The searches were date limited to 1969 and afterward. For each question in the dataset, researchers collected the abstracts of up to 10 peer-reviewed publications relevant to each question. See Appendix B for a full summary of search methods. Then, they coded each abstract for what journal it was published in, identifying it as a family medicine journal or not a family medicine journal. They read the abstracts associated with the question and rated the question as: not at all answered, somewhat answered, mostly answered, or fully answered – will implement in practice. The coding scheme included the following detailed descriptions. Not at all answered: search identifies no abstracts directly addressing the question. Somewhat answered: search identifies abstracts that provide a background foundation to answering the question at hand, but abstracts do not specifically answer the parameters that need to be examined. No specific conclusions or relationships within the question are studied. Mostly answered: search identifies abstracts that provide a background foundation to answering the question and examine parameters like those asked. However, abstracts do not answer/address the specific parameters that we want to examine. The question is partially answered, and some information can be extrapolated from existing data, but further research can be done to clarify some aspects or to fully answer all facets of the question. When literature presented conflicting evidence, coders rated the question as mostly answered. Fully answered: search identifies abstracts that summarized clear answers and solutions they would be able to implement in the context of their practice. Abstracts directly answer the question posed and provided ample evidence to support the answer.
Coders recorded how much time was spent in the search. We limited the time search to 60 minutes, which we anticipated would be more time than most primary care clinicians would have to identify if there is an answer to the clinical question. When coders were uncertain about a rating, we discussed it as a team to establish the evidence of the rating. In addition, in the coding documents themselves, coders included their rationales for each rating.
Results
As written, the original list of questions presented 144 questions divided into 21 categories. An additional 12 categories included “no questions.” 2 categories were cross listed with other categories. After subdividing questions into searchable queries, the list expanded to 167 questions. We then removed 31 questions in the review for clarity and structure.
Researchers searched for 136 total questions. Total search time was 4436 minutes, with an average of 32.62 minutes per question (S.D. 12.69). All searches occurred in December 2023–February 2024. Of 1179 abstracts reviewed, 87 (7.4%) were from family medicine journals. See Box 1.
Box 1. Family Medicine Journals* Represented in the Dataset
African Journal of Primary Health Care & Family Medicine
American Family Physician
Annals of Family Medicine
Archives of Family Medicine
Australian Family Physician
BMC Family Practice
Canadian Family Physician (Médecin de famille canadien)
Family Medicine
Family Practice Research Journal
Family Practice
Journal of Family Medicine and Primary Care
Journal of Family Practice
Journal of the American Board of Family Medicine
Journal of the American Board of Family Practice
South African Family Practice
*We include all journal names as indicated in PubMed to demonstrate the historicity of the sample. For example, the Journal of the American Board of Family Practice is now the Journal of the American Board of Family Medicine. This dataset included abstracts from when the journal published under each name.
For the outcome variable, researchers rated 33 questions as not at all answered (24.2%), 49 questions as somewhat answered (36.0%), 37 as mostly answered (27.2%), and 17 as fully answered – will implement in practice (12.5%). See Figure 1 for a distribution of the variable by category. Categories with higher percent of answered questions included the doctor/patient relationship (33.3%), value of continuity of care (25.0%), natural history of common problems (22.2%), family systems and family dynamics (20.0%), and the value of coordinated care (20.0%). Notably, 2 of the categories with the highest number of total questions, community oriented primary care (COPC) and the value of comprehensive care, had the highest percentage of unanswered questions.

Proportion of Hames 100 questions answered by category.
Discussion
The Hames 100 questions and categories themselves demonstrate the values and purpose of family medicine research and can serve as a powerful tool to discuss the future of family medicine research. The varied questions illustrate the broad scope of interest of family physicians in 1985, which remains just as relevant today. Our findings indicate that relatively few (12.5%) questions were fully answered, with even fewer questions answered in family medicine journals. Family medicine is uniquely positioned to address gaps in research that impact the health of our patients and communities. The questions that were fully answered demonstrate great strides in research to understand disease processes and the value of primary care. Research has shown the value of continuity of care and coordination of care, and the clear value of family medicine (eg, Dyer et al12 and Yang et al13). The Hames 100 also can also facilitate discussion on future research questions for the discipline.
Notably, 25% of questions posed were not answered, and 63% of questions were only partially answered. The paucity of answered questions causes us to reflect on how family physicians practice evidence-based medicine. Family physicians often make clinical decisions extrapolated from highly controlled research. Patients are unique and complex, and function within a unique socioecological and psychosocial context. The aggregate of many decisions, when combined into a single patient with unique circumstance, has little evidence base. The practice of medicine necessitates coping with a certain level of uncertainty.14,15
The questions that continue to be unanswered are indicative of the complexity of family medicine and the challenges of finding clear answers to the problems our patients and communities face. These searches revealed how little we understand about some family medicine specific questions such as underlying causes of depression, differences across the life course, or specific recommendations for clinical conversations about cancer prevention and screening.
Research funding for Departments of Family Medicine remains limited, in particular compared with the proportion of the physician workforce providing clinical care.16 As noted in the 2021 National Academies of Sciences, Engineering, and Medicine (NASEM) report on Implementing High-Quality Primary Care, “the current research funding environment has prevented addressing meaningful questions critical to the advancement of primary care.”17 The disease-specific focus and limited time frame of grant funding mechanisms may incentivize a reductionist approach to health conditions, or research on “low-hanging fruit.” Although individual research studies may inform disease-specific management, broader questions on health systems, coordination of care, and comprehensive care cannot be easily answered. Investigating more complex health systems questions require full research programs (with qualitative, quantitative, and mixed-methods research expertise), interdisciplinary expertise and collaboration, as well as longitudinal, sustainable funding mechanisms.
Many questions addressed foundational constructs of family medicine,18 such as continuity, comprehensiveness, and community. However, the evidence for these questions did not uniformly conceptualize or operationalize these concepts, limiting how we can synthesize and apply findings. For example, although family medicine researchers have clearly defined continuity,19 the broader literature did not use these definitions or measures. One notable concept in this dataset is COPC.20 Although family medicine is founded in the context of community, little evidence was available for the value of community-oriented family medicine. However, this lack of evidence could be connected to the rare use of this term. As researchers, we must attend to how we define and describe these concepts. Otherwise, lessons we learn from COPC or, more recently, patient-centered medical homes (PCMH)21 will be lost in the literature.
Although family medicine researchers are well positioned to answer questions that include layers of family, systems, and community, our results show that evidence to these family medicine questions is more commonly found in literature outside family medicine journals. This could relate to the overlap with other specialties (eg, research on cancer may be more likely to be published in cancer specific journals). However, it also reduces our ability to understand the impact family medicine researchers have on the medical literature.
Interpretations are limited to the method and search strategy. Searches were limited to PubMed; however, some of the questions would likely be better answered by social scientists and indexed in the American Psychological Association PsycINFO or the Education Resources Information Center (ERIC). The Hames 100 predates the FINER criteria,22 with many questions difficult to truly interpret or assess. These family medicine pioneers did not review the questions for feasibility, interest, novelty, ethics, and relevance when they created the list. Many research questions were specific to their time period and context and are not relevant or applicable in the current health care landscape. Some of the research questions listed are no longer important to today’s clinical practice.
As our team discussed the available evidence for some questions, we debated whether a question was answered if the existing evidence was bound by time. Ultimately, this study demonstrated that research questions must be revisited and studies replicated. Two question contexts were particularly sensitive to time: money and relationships. When the question queried the cost of health care, we were less likely to consider a question fully answered. Cost models were bound by the larger economy at the time of study. Similarly, many questions involved relationships: between the patient and physician and within families. Since relationships are culturally situated, the evidence from older studies was less applicable to today’s practice.
Furthermore, important questions may have been missing from the Hames 100. It is important to continually review these lists to guide the future of primary care research. The NASEM report on Implementing High-Quality Primary Care identified many examples of research questions that go unasked due to the current funding and peer-review environment.17
The Hames 100 questions provide a fascinating look into the values and broad scope of care of family physicians at the time of the 1985 Hames Consortium. Many questions remain practical and important today, yet few questions from this time period are fully answered. This study highlights the importance of translational research to implement care that we know to be evidence-based, but also flags the importance of increased and sustained investment in family medicine research and support for longitudinal interdisciplinary collaborations to research more complex and broad health care questions that remain unanswered. Further, these findings indicate the important role of family physicians in research.
Acknowledgments
In the original document, each question is followed by a set of initials. We presume these to indicate the authors of the “100 Most Important Family Medicine Research Questions.” However, the Curtis G. Hames, Sr., Papers 1943-1999, located in Historic Collections and Archives in the Robert B. Greenblatt, M.D. Library at the Medical College of Georgia, have no additional information about the question writers. Thus, we acknowledge them here: LC, MW, LG, PF, KW, PN, LB, MG, CB, CS, GF. We also thank John Frey and John Saultz for reviewing early versions of this manuscript.
Appendix A








Appendix B
Search Strategy and Coding Process


Notes
This article was externally peer reviewed.
Funding: None.
Conflict of interest: CJWL and DAS are editors of the JABFM, and JB is editing Fellow.
To see this article online, please go to: http://jabfm.org/content/37/S2/S106.full.
- Received for publication March 23, 2024.
- Revision received June 30, 2024.
- Accepted for publication July 8, 2024.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.