
Abstract
Research is being recognized as important to the further growth of Family Medicine. It is also important to improving the health of the nation. Family Medicine must consider the barriers and facilitators to research to plan for the future. Understanding the role of all members of the research team is necessary. In February 2024, a descriptive analysis of Family Medicine Principal Investigator (PI) with active projects funded by the National Institutes of Health(NIH) was performed using the NIH Research Portfolio Online Reporting Tools Expenditures and Results (RePORTER) tool. Sixty-four percent of the 310 grants identified were awarded to Principal Investigators (PIs) with PhD degrees. Researchers with a PhD have been able to significantly contribute to the research mission of the discipline. Family medicine will need to continue to expand the research team to optimize productivity.
- ADFM/NAPCRG Research Summit 2023
- Administration
- Capacity Building
- Community-Based Participatory Research
- Faculty
- Family Medicine
- Research
In the beginning of the discipline, the priority was on creating administrative units in academic medical centers that could house the teaching of family medicine (FM). Initially, the focus was on residency teaching. It quickly became clear that to increase the number of FM residents, there was a need to work at the medical school level to prepare students for a future career in FM. In addition, there was rapid growth in the number of community-based programs for training family medicine residents. At the time, it was thought by some that these programs were potentially better for family medicine training because of the lack of competition from other specialties and the more prominent community focus. Most of these programs, however, were less likely to pursue a research focus. During this time, there were nonphysicians (ie, education specialists, clinical psychologists, social workers, etc.) who were included in the educational mission.1 Research was not a clear priority.
The discussion about research in FM was propelled by 2 major motivations; the desire or recognition that family medicine could not gain “parity” in the academic health center without a research portfolio, and more importantly, family medicine needed to define its importance in the health care system with a set of internally derived, evidence-based definitions.2 At this point, there was a paucity of family physicians with substantive research training. It was felt by many that academic departments needed to have family medicine trained research leadership as role models (as opposed to nonphysicians). Since there was a lack of research legacy in family medicine, many FM faculty did not know how to use PhD trained researchers. Furthermore, family medicine research was less conducive to the model of working with laboratory trained basic scientists that was prominent in other specialties. Another model, that some viewed as negative, was having PhD researchers in Departments of Family Medicine, in some instances, doing research that “really was not family medicine” (eg, toxicology). Likewise, most PhD researchers had little or no knowledge of primary care.
When this article was first proposed, there was an assumption that more had to be done to integrate PhDs into departmental research planning, even though it was known that there were many examples of PhDs working collaboratively in departments, and even serving as research directors and Vice Chairs of Research.3 However, a review of an admittedly incomplete research director list of the Association of Departments of Family Medicine (ADFM) shows that 50% of research directors have a PhD as their terminal degree while 75% of Vice Chairs of Research have a PhD, including 1 Doctor of Pharmacy (PharmD) and 1 MD/PhD. So, there is significant integration of PhD researchers in FM already.
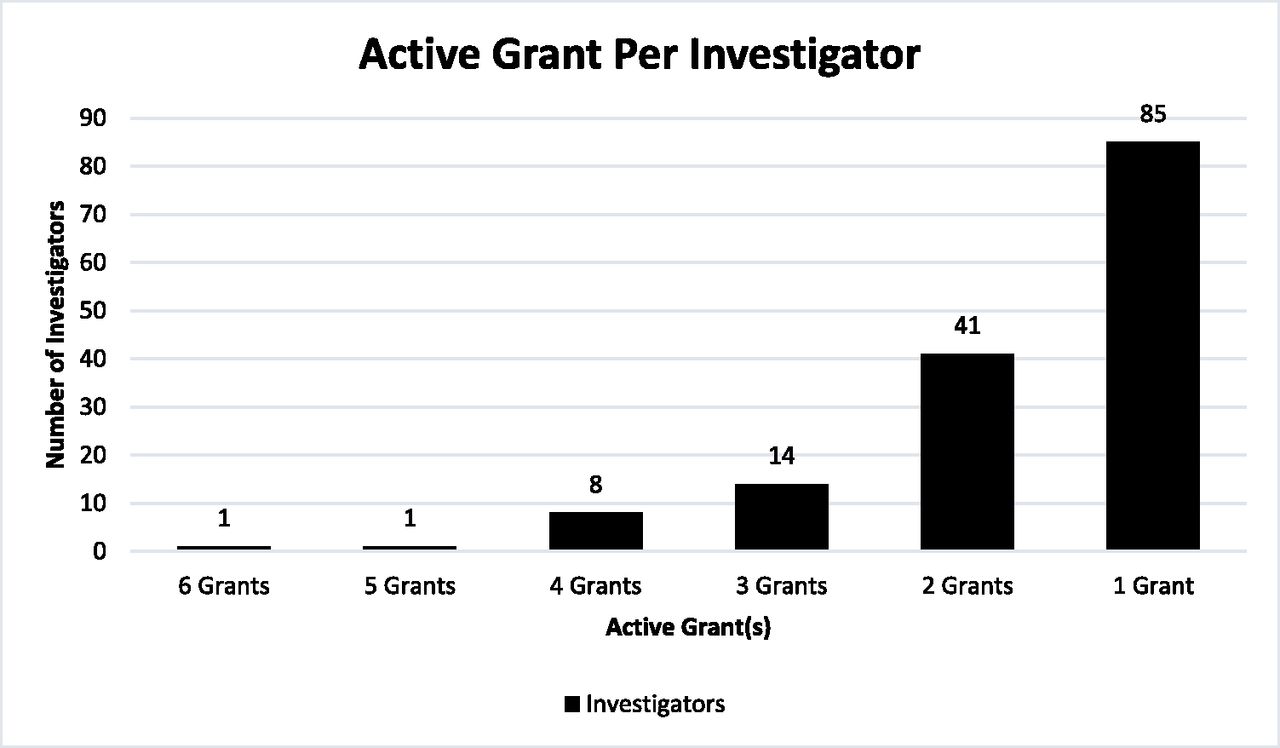
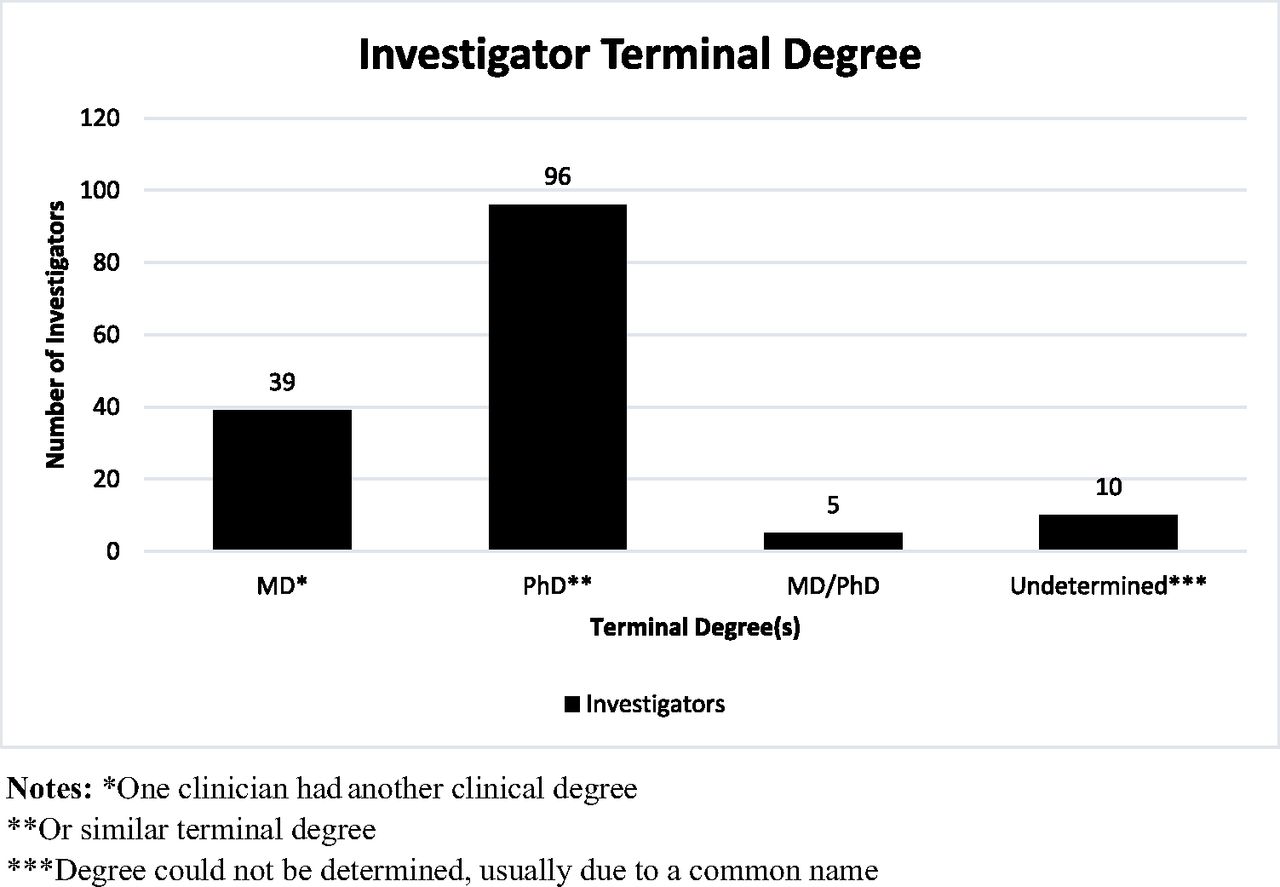
In another attempt to quantify the role of PhDs in family medicine research, a review of the receipt of federal funds for research was undertaking using the National Institutes of Health (NIH) Research Portfolio Online Reporting Tools Expenditures and Results (RePORTER), which is “an electronic tool that allows users to search a repository of both intramural and extramural NIH-funded research projects.”4 On February 15, 2024, a search for grants awarded to Principal Investigators (PIs) in Departments of Family Medicine identified 310 active projects. Importantly, this is an undercount because only investigators from departments in which Family Medicine is listed first in the name are included. (Departments of Community and Family Medicine are listed under public health and preventive medicine.) This classification is subject to error but amenable to correction on notification of the NIH of the investigators preferred department classification. Figure 1 shows the number of grants per person. Figure 2 shows the number of grants by degree type. Sixty-four percent of FM grants were awarded to PhDs. If you compare this with grants awarded by NIH between 2014 and 2023 68.5% of awards were given to principal investors with a single nonclinical degree.5

Number of investigators by volume of federally funded grant projects.

Number of federally funded investigators by terminal degree(s).
This data suggests that PhD PIs in FM are similar in percentage to other NIH grantees.
Perhaps our future is already here. This future calls for further work to define and refine the roles of PhDs and other doctoral trained faculty in the pursuit of family medicine research. To this end, some have advocated that the physician-scientist model should be employed to train a cadre of family physicians who get the type of training that is offered in rigorous PhD programs. This model is currently being piloted in family medicine. However, most MD/PhD programs are in the basic sciences and do not relate to the usual family medicine topics. There are a few MD/PhDs who have their other degree in social sciences.6 There are 2 PhD programs in family medicine in Canada. There are others in Europe. In the United States, there are doctoral programs in population health and similar topic areas, but there are not any that are explicitly focused on family medicine research. In another respect, there are too many people, especially students and residents, who believe that the path to family medicine research lies through getting a Master's degree in Public Health (MPH). While this training is useful in understanding evidence-based medicine and understanding the dynamics of community outreach, most MPH programs are insufficient in and of themselves to the launching of a research career. Pre- and postdoctoral training awards, such as the T-32 and K-series career development awards, provide an opportunity to do substantive training of PhDs and MDs, but those usually require, appropriately so, that the administrative unit already have a substantive research record and infrastructure. These programs also provide an opportunity to train PhDs in a family medicine model; this is requisite to optimize research synergy.
The future of FM research depends in part on FMs ability to work collaboratively with other disciplines to solve problems that need to be solved. This thought is consistent with the gauntlet laid down by the then head of NIH, Elias Zerhouni M.D., when he said that many of the major problems that we face in the 21st century cannot be solved by a single discipline.7 This concept takes on an even greater importance when we consider how important social circumstances are in influencing medical outcomes. The built environment, climate change, nutrition, communication, socioeconomics, structural racism, and social stress all play a part in determining the medical outcomes that patients and thus society face. PhD researchers play multiple roles in fulfilling the needs of family medicine research. PhD research faculty can serve as content experts, mentors, research strategic planners and multiple other roles. Family medicine can prepare itself for expansion of the breadth and depth of research by continuing to build multidisciplinary teams.
Acknowledgments
Many thanks to Sue Rovi, PhD, Ping-Hsin Chen PhD, and Jesse Crosson, PhD for your presence on the journey.
Notes
This article was externally peer reviewed.
Funding: None.
Conflict of interest: None.
To see this article online, please go to: http://jabfm.org/content/37/S2/S53.full.
- Received for publication April 15, 2024.
- Revision received October 3, 2024.
- Revision received October 7, 2024.
- Accepted for publication October 14, 2024.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.