
Article Figures & Data
Figures
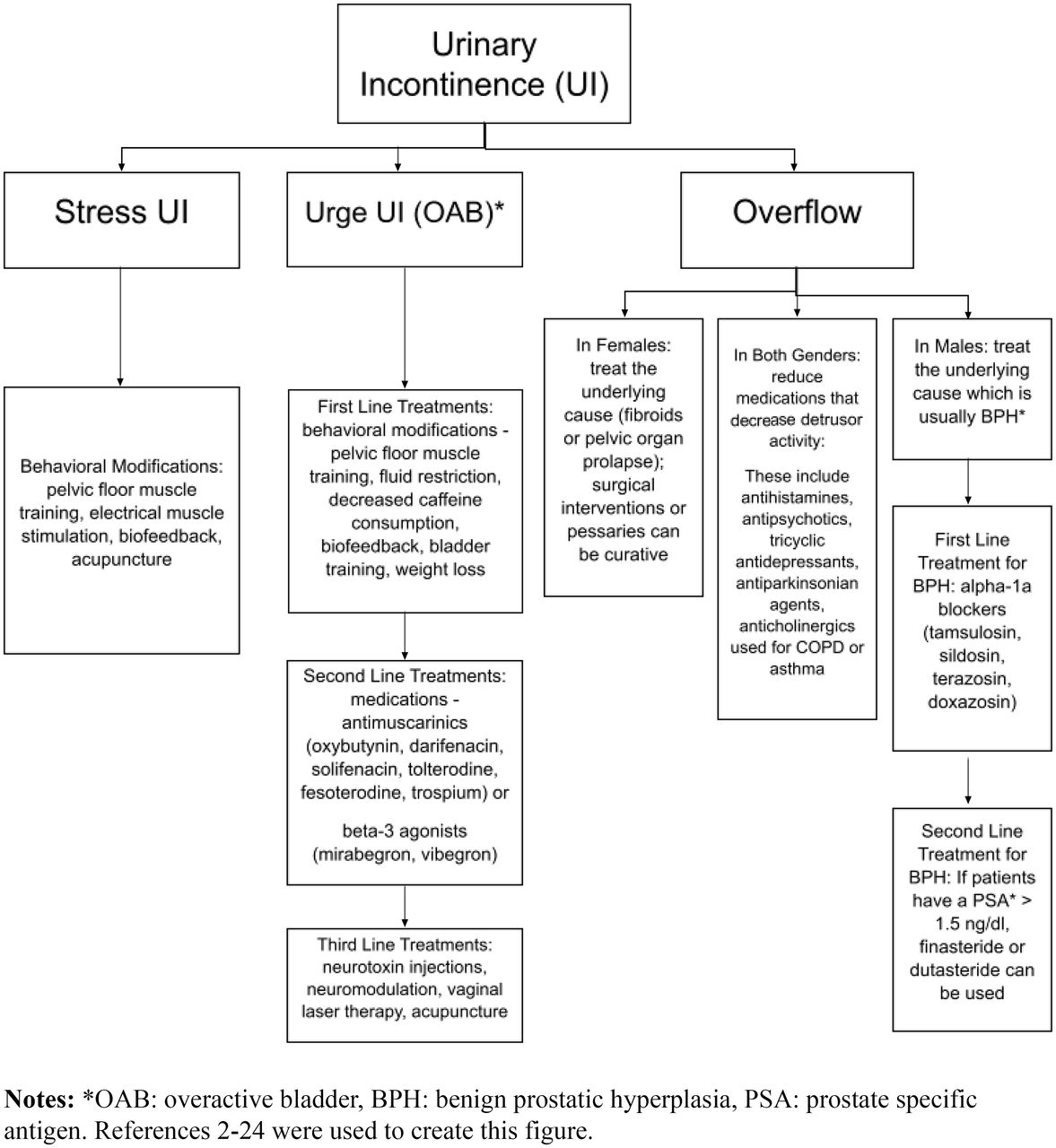
- Figure 1.
Flowchart of types of urinary incontinence and corresponding treatments.
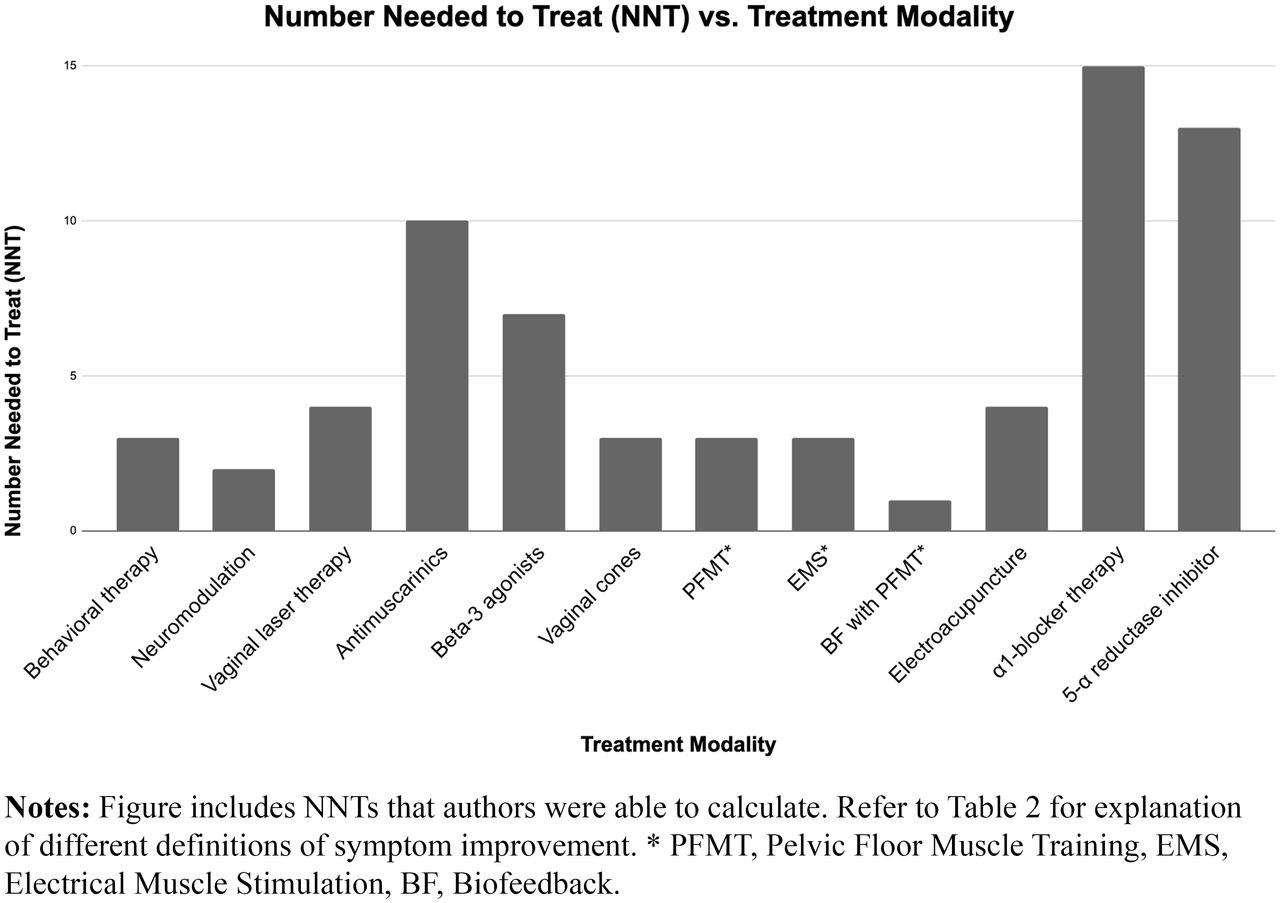
- Figure 2.
Treatment modalities and numbers needed to treat.


Tables
Type of Incontinence Definition Stress Incontinence Weakness in the urethral sphincter and/or pelvic floor causes involuntary leakage of urine when there are increases in intra-abdominal pressure (e.g., with exertion, coughing, sneezing).1 Urge Incontinence Detrusor overactivity causes urinary urgency.1 Mixed Incontinence Combination of stress and urge incontinence.1 Overflow Incontinence Overdistended bladder due to impaired detrusor contractility and/or bladder outlet obstruction causes involuntary leakage of urine.1 Neurogenic Incontinence Impaired function of either the bladder, bladder neck, and/or its sphincters related to brain, spinal cord, or nerve problem.24 Treatment Modality Type of Incontinence for Directed Therapy 1st, 2nd, or 3rd Line Therapy Adverse Effects NNT SOR Behavioral therapy (fluid restriction, bladder-sphincter biofeedback, bladder training and pelvic floor muscle exercises) Urge, Stress, and Mixed 1st line No major side effects were reported.2 NNT = 3, for >75% reduction in frequency of incontinence after 8 weeks of treatment.32 B Neurotoxin injections Urge 3rd line Urinary retention requiring clean intermittent self-catheterization (6.5% rate) and urinary tract infection (25.5% compared to 9.6% with placebo).5 Limited published randomized controlled trials did not report adequate data to calculate NNT. B Neuromodulation (PSNM, PTNS) Urge 3rd line Adverse events of PSNM include pain at the stimulator and lead sites (8.5 to 42%)6, lead migration (3.4 to 19%)6, infection (3.5-5%)6, and surgical revision with high reintervention rates at a median of 33.2%.33
Adverse effects of PTNS include discomfort and pain at stimulation site (2 to 17%)6, tingling, and swelling of the leg.33NNT = 2 for PTNS to achieve >50% reduction of incontinence episodes.34 B Vaginal laser therapy Urge 3rd line Vaginal discharge (10%) or spotting (6.7%) lasting a few days.35 NNT = 4 for objective cure at 12 months after CO2 vaginal laser.36 B Acupuncture (for urge incontinence) Urge 3rd line Rare side effects reported.10 Limited published randomized controlled trials did not report adequate data to calculate NNT. B Antimuscarinics (oxybutynin, darifanecin, solifenacin, tolterodine, fesoterodine, and trospium) Urge 2nd line Anticholinergic side effects such as dry mouth (7 to 34%)37, constipation (2 to 19%)37, blurred vision (2 to 5%)37, dyspepsia (1 to 8%)37, urinary retention (6%)13, and impaired cognitive function.15
Tolerability is one of the most common reasons for discontinuation, and persistence rates at one year range from 15 to 25%.12
Longer-acting once-daily formulations are less likely to cause severe adverse effects.13
Topical oxybutynin patch or gel have a lower incidence of dry mouth and constipation.13NNT = 10 with tolterodine to achieve 75% reduction of urge incontinence episodes at 12 weeks.15 B Beta-3 agonists (Mirabegron and Vibegron) Urge 2nd line Mirabegron may cause dose-dependent blood pressure changes and tachycardia.38
Vibegron does not produce the same blood pressure elevation, but direct comparisons of the two drugs are unavailable.39Mirabegron should be used with caution in patients with severe or uncontrolled hypertension.38
Both drugs can cause xerostomia, constipation, and UTI in less than 6% patients.38,39NNT = 7 with vibegron to achieve 75% reduction of urge incontinence episodes at 12 weeks.15 B Vaginal cones, pessaries, and urethral plugs Stress (from POP) 1st line The common complications were extrusion of the pessary, bleeding, pain, or vaginal discharge, but these conditions could be easily solved after topical antibiotics, vaginal estrogencream, or discontinuation of pessary for a few days.19 NNT = 3 for vaginal cones to achieve a negative pad test after 6 months of therapy.40
Limited published randomized controlled trials on pessaries did not report whether symptoms were resolved so NNT could not be calculated.B Pelvic Floor Muscle Training (PFMT) Stress or Mixed 1st line No major side effects reported. NNT = 3 for PFMT to achieve a negative pad test after 6 months of therapy.40 A Electrical Muscle Stimulation (EMS) Stress Adjunct No major side effects reported. NNT = 3 for EMS to achieve a negative pad test after 6 months of therapy.40 A Biofeedback (BF) with PFMT Stress Adjunct No major side effects reported. NNT = 1 for PFMT with BF to achieve a pad test of 1 g or less 8 weeks after treatment.41 A Electroacupuncture Stress 1st line No major side effects reported. NNT = 4 reporting 50% or greater recovery at 6 weeks.42 A Alpha-1-blocker therapy (tamsulosin, silodosin, terazosin, doxazosin, alfuzosin) Overflow 1st line Orthostatic hypotension (6%), ejaculatory dysfunction (4%).43Alfuzosin has a lower incidence of ejaculatory dysfunction.25 NNT = 15 to lower urinary tract symptoms over 4 years.44 A 5-alpha reductase inhibitor (finasteride, dutasteride) Overflow 2nd line Reduction of PSA by 50% after three months of use.25 NNT = 13 to prevent one case of urinary retention and/or surgical treatment of BPH with alpha blocker plus 5-alpha reductase inhibitor combo therapy.45 B Clean Intermittent Catheterization Neurogenic bladder 1st line CAUTI. Hydrophilic pre-lubricated single-use catheters are less likely to cause CAUTI compared to standard polyvinyl chloride multi-use catheters.30 Limited published randomized controlled trials did not report adequate data to calculate NNT. C Strength of Recommendation and Level of Evidence is based on Strength of Recommendation Taxonomy (SORT).
NNTs reported were calculated by the authors based on data provided in the articles referenced.
Abbreviations: NNT, Number Needed to Treat; PSNM, Percutaneous Sacral Nerve Modulation; PTNS, Percutaneous Tibial Nerve Stimulation; CO2, Carbon Dioxide; UTI, Urinary Tract Infection; POP, Pelvic Organ Prolapse; PFMT, Pelvic Floor Muscle Training; EMS, Electrical Muscle Stimulation; BF, Biofeedback; PSA, Prostate-Specific Antigen; BPH, Benign Prostatic Hyperplasia; CAUTI, Catheter Associated Urinary Tract Infection.




{kind=link}
{kind=link}