
Abstract
Introduction: Psychological safety is the perception that it is safe to express oneself without fear of ridicule. Better patient outcomes are associated with health care teams that experience psychological safety. However, the psychological safety of the patient has largely been ignored, even though it may affect patient forthrightness and adherence. We developed an initial Patient Psychological Safety Scale (PPSS) to assess patients’ experience of psychological safety.
Methods: Thirteen items modified from team-focused measures of psychological safety comprised the initial version of the PPSS. To explore criterion validity, 8 items pertaining to nondisclosure of important information were used. A convenience sample of 100 patients from 4 primary care settings completed a survey comprised of the PPSS and nondisclosure questions.
Results: A confirmatory factor analysis (CFA) indicated that the 13-item PPSS did not measure 1 factor. A subsequent exploratory factor analysis (EFA) identified 2 factors. A second CFA was conducted on a modified 9-item PPSS representing the 2 factors and retaining items with a factor loading of 0.40 or higher, and the results indicated a good fit. Internal reliability and validity for factors 1 (relationship comfort) (α = 0.95) and 2 (belonging) (α = 0.88) were strong. Although few respondents endorsed nondisclosure, there was a significant association between lower relationship comfort and nondisclosure of disagreement with clinician recommendation (median difference = 5.0, P = .001).
Conclusions: Patients’ experience of psychological safety may affect clinical outcomes. The PPSS provides a starting point for further study of this potentially important variable.
- Behavioral Sciences
- Factor Analysis
- Patient Care Team
- Patient Safety
- Patient-Centered Care
- Primary Health Care
- Psychological Safety
- Scales
- Surveys and Questionnaires
Introduction
Psychological safety is the perception that it is safe to voice one’s concerns, raise questions, and express opinions without fear of judgment or ridicule. Since this concept was described more than 30 years ago with respect to the effective function of teams in organizations and the engagement of team members,1–2 studies have found that the presence of psychological safety in organizational teams is associated with many positive workplace outcomes.3 One of the arenas in which the construct has been widely applied is health care,4–5 and research results indicate that better patient outcomes occur when health care treatment teams are marked by psychological safety.6⇓–8
There have been many benefits from the attention given to psychological safety for health care teams, but the psychological safety of one of the members of the health care team has largely been ignored. In patient-centered care, the patient is considered to be a crucial, if not the most important member of the team. Patient-centered care emphasizes partnership and collaboration, effective communication, understanding of the patient’s situation and experience of their health challenges, and a relationship in which there is reciprocal trust,9⇓–11 contributing to health promotion and improved health outcomes.12⇓–14 It is surprising, therefore, if not troubling, that the construct of psychological safety tends to not be applied to the patient experience. While most clinicians would agree that it is important for patients to feel that they will not be judged in health care settings, that they can freely ask questions and express concerns, and that their thoughts and opinions will be valued, there is evidence that this is far from the ubiquitous experience of patients. Levy and colleagues reported data indicating that a majority of adults have withheld important information from their clinicians, particularly if they disagreed with recommendations.15 The most prevalent reason for nondisclosure was not wanting to be judged or lectured.
Physiologically, human amygdalae are wired to perceive social threats as well as physical threats, because human survival is enhanced by cooperation and social connection but endangered by discord and hostility.16–17 When presenting for health care, patients may bring anxiety, fear, or suspicion due to new distressful symptoms, previous experiences of judgment by health care workers, or poor health outcomes of close family members. Furthermore, if patients expect to experience condescending attitudes or lectures,15 they may have heightened awareness of threats to psychological safety. Perceived threats can have both physiologic and behavioral responses that potentially affect chronic illness management. Possible physiologic effects include cortisol surge and other inflammatory cascades which may exacerbate poor health and suppress immune function, especially among individuals already exposed to social adversity.18–19 Behaviorally, patient engagement and activation may be adversely affected. The patient’s role in the management of chronic conditions is considered to be more crucial than formal medical care.20 When collaborative treatment plans clearly incorporate the patient’s goals and priorities, there tends to be greater patient ownership of their health, which leads to better treatment adherence and outcomes.13,21,22
To the extent that clinicians rely on patients to describe symptoms, history, lifestyle behaviors, medication adherence, and potential barriers to treatment, it can be posited that patient psychological safety may be one of the most far-reaching aspects of patient safety. This involves amplifying the “belonging” cues in health care environments with patient-centered interactions and minimizing both physical and social “threat” cues.10,23 For clinicians, high-quality listening is an essential ingredient in the communication of psychological safety,24 particularly if the listening includes compassionate curiosity in which appropriate follow-up inquiry occurs for additional depth and understanding. Furthermore, the clinical setting that prioritizes psychological safety will be cognizant of the importance of minimizing overt or covert expressions of bias, whether they be aspects of the physical environment or interpersonal interaction. With respect to social determinants of health (SDOH), a patient experiencing psychological safety is more likely to share concerns about medical costs, environmental or social barriers such as transportation issues, literacy challenges, or experiences of trauma or discrimination.
If patient psychological safety is to gain attention, there needs to be a way to assess it. At present, no measure of patient psychological safety has been found in the extant literature. Therefore, we sought to modify team-focused measured scales for psychological safety to create a brief patient psychological safety scale, maintaining consistency with the types of items found on team-focused scales to the extent possible. Here we describe the initial data collection with the scale items we developed, the results of the factor analysis of the new scale, and an initial exploration of criterion validity.
Methods
Participants
Third-year medical students completing rotations in 4 midwestern Family Medicine practices invited patients at the time of checkout to complete the Patient Psychological Safety Survey (PPSS), producing a nonrandomized sample of convenience. The 4 sites were an academic Family Medicine practice with approximately 11% African American (AA) patients, a suburban practice in a community with approximately 65% AA residents, a suburban practice in a community with approximately 5% AA residents, and a small-town practice with approximately 10% AA residents. Data were collected between August and December 2022. The research protocol was approved by the university Institutional Review Board, finding that the protocol protected the rights and welfare of human subjects and met federal regulations for the protection of human subjects in research. Patients invited to participate in the study were provided with an informed consent document to read. The initial item on the survey asked participants to indicate agreement with a statement that they had read the informed consent form and agreed to give their consent.
Measures
A 13-item PPSS was developed by the authors by modifying items from team-focused measures of psychological safety, aiming to maintain consistency with the types of items found on these other measures. We sought to keep our scale brief and have the respondents’ experience with their clinician be the focal point of consideration. For this initial scale development, we did not endeavor to consider all the possible contributors to patient experience with their clinician, such as cultural factors that affect patient expectations. A 5-point Likert scale was used, with 1 being “strongly disagree” and 5 being “strongly agree.” Respondents were instructed to consider the “clinician” to be their primary provider. Items included in the original scale are included in Table 1.
Items Included in the Initial Scale and Factor Loadings for the Resulting 9-Item Patient Psychological Safety Scale
The 7 questions used by Levy and colleagues to investigate patient nondisclosure of important information were included in the overall survey.9 One additional question was added: “Have you ever avoided telling your clinician that you did not intend to follow through with their recommendations?” These 8 questions (included in Table 2) requested a “yes” or “no” response.
Psychological Safety Scales by Avoidance Questions (n = 94)
Data Analyses
Descriptive statistics were produced for the demographics of the participating patients and study variables – percentages for categorical variables and medians and interquartile ranges (IQR) for continuous variables. A confirmatory factor analysis (CFA) was conducted to examine psychological safety as 1 single construct/scale. The following fit indices were used to determine the fit of the model: Root Mean Square Error of Approximation (RMSEA), Comparative Fit Index (CFI), and the Standardized Root Mean Square Residual (SRMR). A model is considered to have acceptable fit if the RMSEA, CFI, and SRMR are <0.08, >0.90, and <0.08, respectively. Since the original hypothesized model did not fit well, we conducted an exploratory factor analysis (EFA) to determine the number of factors. Based on the results of the EFA, a CFA was then conducted with the new factor(s). Cronbach alphas were then estimated to examine the internal validity and reliability of the new scale(s). Descriptive statistics with means and standard deviations were estimated to describe the scales. For the questions regarding withholding of information, Wilcoxon rank sum tests were used to examine differences in median factor scores between those who endorsed avoidance and those who did not. All analyses were conducted using R version 4.1. For the CFA, the Lavaan package was used.
Results
A total of 100 patients responded to the invitation to complete the survey, although analyses were performed only on the 94 with complete data. Slightly over half (51.0%) of participants were <55 years of age and 75% of participants were females. Participants were not asked to indicate their race.
The results of the first CFA considering the patient psychological safety scale as a single factor suggested that the model was not a good fit (RMSEA = 0.14; CFI = 0.86; SRMR = 0.09). An EFA was then conducted to explore the number of factors. The eigen values suggested 2 factors. We kept items that had a factor loading of 0.40 or higher for each factor (see Table 1). Two of the items (“My clinician would be unhappy if I disagreed with their recommendations” and “My clinician’s office space does not make me feel safe and welcome”) did not load onto either of the 2 factors and 2 items (“My clinician has negative feelings toward me” and “My clinician makes assumptions about me and my life”) had low factor loadings on the first factor and were removed. A second CFA was then conducted to examine the 2-factor scale.
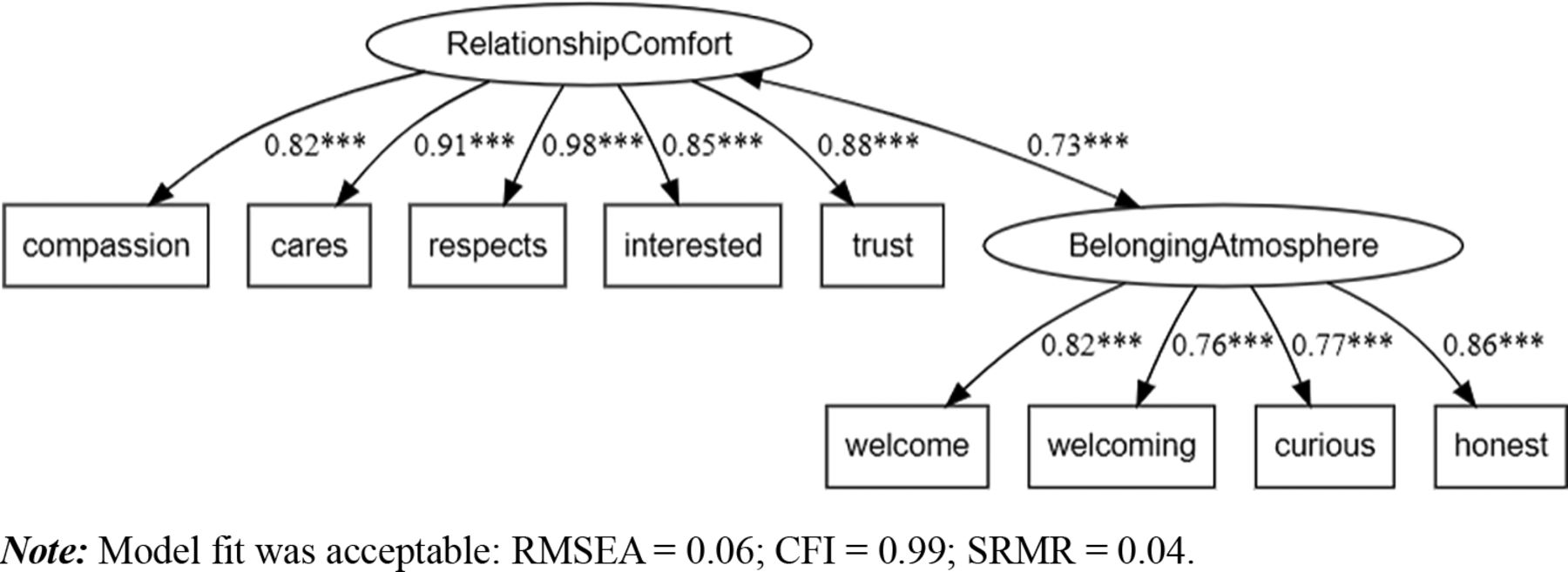
The results of this second CFA suggested that the model was a good fit (RMSEA = 0.06; CFI = 0.99; SRMR = 0.04) (see Figure 1). In addition, the model’s χ2 (33.96) and P-value (0.14) also suggested a good fit model. The Cronbach’s alphas for factor 1 (relationship comfort) (α = 0.95) and factor 2 (atmosphere of belonging) (α = 0.88) suggest good internal validity and reliability. The median (range) for factor 1 was 25.00 (17.00, 25.00) and for factor 2 was 19.00 (7.00, 20.00).

Confirmatory factor analysis (CFA) results for a 2 factor construct of patient psychological safety. Abbreviations: RMSEA, Root Mean Square Error of Approximation; CFI, Comparative Fit Index; SRMR, Standardized Root Mean Square Residual.
A secondary analysis was conducted to assess the relationship between relationship comfort, atmosphere of belonging, and the nondisclosure questions. A small proportion of the sample population endorsed nondisclosure with their clinician; endorsed responses ranged from 2.1% to 7.5% (Table 2). There was a significant association between lower relationship comfort and avoidance in telling your clinician that you disagreed with their recommendation (median difference = 5.0, P = .001). The majority of avoidance questions were not associated with the factors, however, participants who endorsed avoidance had lower median scores compared with those who did not endorse avoidance.
Discussion
Based on the factor analysis of our original 13-item PPSS, we have produced a shorter 9-item scale that can measure 2 important contributors to psychological safety. Acknowledging some overlap in these 2 factors, they seem to be assessing relationship comfort (factor 1) and an atmosphere of belonging (factor 2). Relationship comfort refers to perceptions of the clinician’s sincere interest in and respect for the person of the patient. An atmosphere of belonging pertains more broadly to the welcoming nature of the office setting and staff.
With respect to the exploration of criterion validity of the PPSS, unlike the prevalence of nondisclosure of information found in the Levy and colleagues' study of online survey sample of adults,9 established patients in our primary care settings reported very little nondisclosure. Given this low variability and small sample size, a larger study will be necessary for the assessment of criterion validity.
This was the initial study of the development of the PPSS and has some important limitations. The aim for the initial 13 items was that they be as similar as possible to the types of questions on team-focused measures of psychological safety, rather than considering the wide domain of variables that can affect patient experience with their clinician. Therefore, it is possible that relevant factors are not represented in the resulting PPSS. Data were collected in primary care settings in which patients were generally well-established with their primary clinician. Some degree of selection bias was likely present in this nonrandom sample of convenience, in that those patients agreeing to participate in the study may have been most positively inclined toward their clinician. Relatively few patients reported nondisclosure of important information to their clinician, a finding that limited our assessment of criterion validity. The PPSS will need to be studied with a random sample of patients, preferably in different types of clinical settings. Examining the association of the PPSS with important clinical variables such as adherence and outcomes will be important next steps. Also of interest will be identifying what specific interpersonal and environmental characteristics affect patient psychological safety, such as concordance or disconcordance between the clinician and patient on race or gender.
While the physical safety of patients has deservedly been prioritized in the provision of health care and the accreditation of health care organizations, and patient satisfaction has been used as a performance metric, the psychological safety of patients may prove to be an under-the-radar but modifiable factor that affects patient outcomes and satisfaction. Feeling safe can be appropriately understood as an aspect of being safe.25 Given the central role of the patient on the health care team, serious attention to patient psychological safety is needed. The development of the PPSS represents an initial attempt to address an important gap in the study of psychological safety in the health care setting, that is the experience of the patient. The PPSS may serve to stimulate additional research to better understand clinician behaviors that are associated with higher degrees of psychological safety, and how patient psychological safety affects important aspects of patient care and resulting clinical outcomes.
Notes
This article was externally peer reviewed.
Funding: There is no financial or other support for this work to report.
Conflict of interest: None of the authors have conflicts of interest to report.
This research protocol was approved by the Wright State University Institutional Review Board, finding that the protocol protects the rights and welfare of human subjects and meets the requirements of Wright State’s Federal Wide Assurance (FWA 00002427) and the federal regulations for the protection of human subjects in research (e.g. 2018 45 CFR 46.104).
To see this article online, please go to: http://jabfm.org/content/37/5/809.full.
- Received for publication December 12, 2023.
- Revision received February 29, 2024.
- Accepted for publication April 8, 2024.




{kind=link}