
Article Figures & Data
Figures
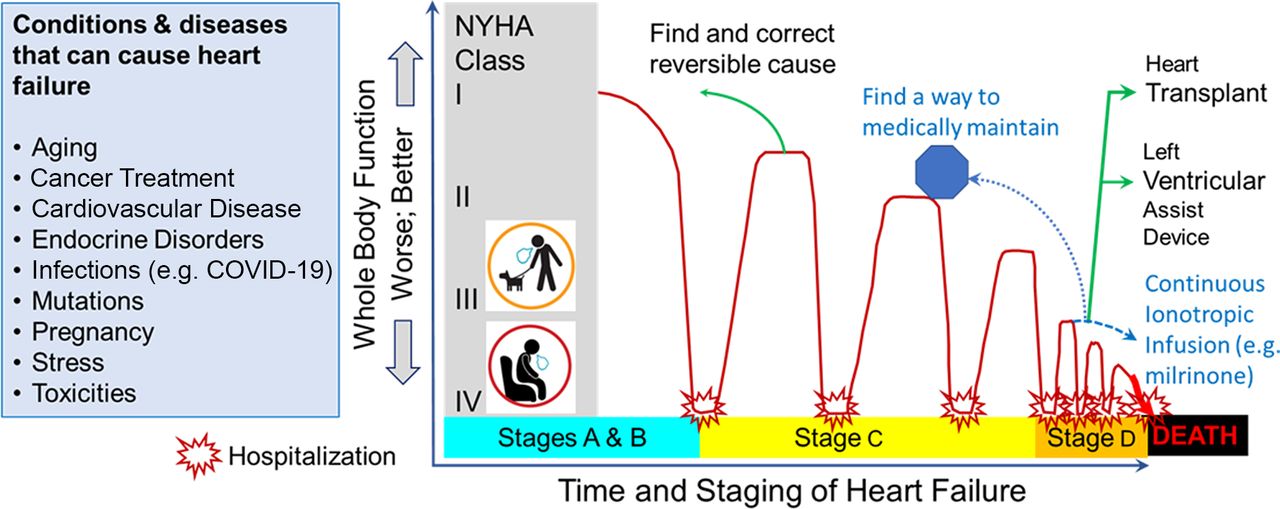
- Figure 1.
Heart Failure Progression. Many underlying disease processes cause the heart to fail. Unless a correctable underlying cause is found and successfully treated, the majority of heart failure (HF) patients will progress in an undulating downward fashion toward death. American Heart Association (AHA) Staging describes the status of HF1: A “at risk for HF,” has underlying risk but without detectable dysfunction, such as hypertension; B “pre-HF”: has underlying cause and detectable cardiac dysfunction but without over heart failure symptoms; C “symptomatic HF”: has documented cardiac dysfunction and heart failure symptoms; D “advanced HF”: patient has refractory heart failure without chance of meaningful return to an acceptable plateau. The New York Heart Association (NYHA) classification describes a patient’s overall function (I: normal; II: moderate exertion causes symptoms; III: mild exertion causes symptoms; IV: symptoms at rest or with minimal exertion). Continuous inotropic infusion can provide a bridge to intervention (heart transplant or left ventricular assist device), bridge to medical treatment to achieve a better plateau, or palliative comfort care.

Tables
Stage Description A At-risk for HF but without functional heart disease or evidence of dysfunction B Pre-heart failure, or patients with evidence of structural heart disease but not clinical symptoms or signs C Symptomatic heart failure D Advanced or refractory heart failure Abbreviation: HF, Heart failure.
Left Ventricular Ejection Fraction (LVEF) ≤ 40% 41–49% ≥ 50% Has well developed guideline-directed medical therapy. Medical therapy needs to be continued with improvement in LVEF Heart Failure with Reduced Ejection Fraction (first presentation) Heart Failure with Improved Ejection Fraction Has not been investigated as separate entity; therefore, there is no data Heart Failure with Mildly Reduced Ejection Fraction (first presentation) Some treatment is possible Heart Failure with Preserved Ejection Fraction (first presentation) Class Description I Patients with heart disease with no limitation of physical activity. II Patients with heart disease with slight limitation of physical activity. Ordinary activity produces symptoms, but no symptoms are produced at rest. III Patients with marked limitation of physical activity. Less than ordinary activity creates symptoms, but no symptoms are produced at rest. IV Patients cannot perform physical activity without symptoms. Symptoms may be produced at rest. Comorbid Condition Recommendation Evidence Rating Hypertension Uptitration of medications according to GDMT to maximum tolerated dosages SORT A1 Diabetes SGLT2i as initial therapy for hyperglycemia SORT A10 Iron deficiency Intravenous iron repletion SORT B9 Central Sleep Apnea Adaptive servo-ventilation should not be used as it increases mortality SORT A1 Atrial fibrillation Guideline directed management should be pursued, including consideration of rhythm control and left atrial appendage closure in select patients SORT A vs B depending on component of therapy1 Valvular heart disease Manage according to current guidelines See relevant guideline11 Ischemic heart disease Should be considered in cases of HF to facilitate diagnosis and management SORT B1 Abbreviations: HF, Heart failure; GDMT, guideline-directed medical therapy.
Drug Class Initial Dose Target or Maximum Dose Comments ARNi Avoid if hemodynamically unstable, history of angioedema, or potassium level ≥ 5 mmol/L
Preferred over ACE-I and ARB due to superior efficacy
Sacubutril-valsartan 24/26 mg twice daily if ACE inhibitor or ARB naïve or 49/51 mg twice daily with adequate blood pressure (SBP ≥ 120 mmHg) 97/103 mg twice daily Original study excluded patients with SBP < 100 mmHg ACE Inhibitor Similar restrictions to ARNi
Use if ARNi is not feasible
Captopril 6.25 mg 3 times daily 50 mg 3 times daily Enalaprol 2.5 mg twice daily 10–20 mg twice daily Lisinopril 5 mg daily 20–40 mg daily Ramipril 1.25–2.5 mg daily 10 mg daily ARB Class preferred with history of angioedema or intolerance to ARNi and ACEi
Use if ARNi is not feasible
Candesartan 4–8 mg daily 32 mg daily Losartan 25–50 mg daily 50–150 mg daily Valsartan 20–40 mg twice daily 160 mg twice daily Beta Blocker Class-wide risk of hypotension, worsening asthma, and contraindicated in untreated high-degree heart block
Limit to carvedilol, metoprolol succinate, and bisprolol; It is not class-wide benefit.
Carvedilol 3.125 mg twice daily 25–50 mg twice daily 6.25 mg is the minimal effective dose. Benefits increases with increasing dose to 25 mg. Metoprolol succinate extended release 12.5–25 mg daily 200 mg daily Bisoprolol 1.25 mg daily 10 mg daily SGLT2i Risk of euglycemic ketoacidosis and urinary tract infections Dapagliflozin 10 mg daily Empagliflozin 10 mg or 25 mg daily 25 mg if patient also has type-2 diabetes. MRA Dose-adjustment or contraindicated depending on renal and potassium status; do not use if potassium level ≥ 5 mmol/L or Cr ≥ 2.5 mg/dL. Avoid if eGFR < 30 mL/min. Spironolactone 12.5–25 mg daily 25–50 mg daily Risk of gynecomastia, breast pain, menstrual irregularities, decreased libido Eplerenone 25 mg daily 50 mg daily Lower risk of gynecomastia Additional Therapies Comments Hydralazine plus nitrate Comments Fixed-dose combination 20 mg isosorbide dinitrate/37.5 mg hydralazine three times a day 40 mg/75 mg 3 times a day If patient is intolerant of RAAS inhibition
African American patients on maximum GDMT needing additional benefit
Separate isosorbide dinitrate and hydralazine 20 mg isosorbide dinitrate and 25 mg hydralazine both three times a day 40/75 three times a day Cardiac glycoside Comments Digoxin 0.125–0.25 mg daily No target dose Care with decreased creatinine clearance Selective sinus node inhibitor Ivabradine 2.5–5 mg twice daily 7.5 mg twice daily Used if HR ≥ 70 in setting of maximal GDMT Soluble guanylate cyclase inhibitor Vericiguat 2.5 mg daily 10 mg daily Use for patients who cannot tolerate or is already on all 4 major categories of beta-blocker, ARNi, Anti-aldosterone, and SGLT2i.
Can cause hypotension, this is a major limitation
Implanted Devices Device Class-1 Indication per AHA/ACC/HFSA Benefit Comments Automated implanted defibrillator (AICD) LVEF≤ 30%, NYHA class-1, > 40 days post MI, expected to live > 1 year Only prevents sudden cardiac death (SCD)thereby reducing mortality Does not improve cardiac function Automated implanted defibrillator (AICD) LVEF≤ 35%, NYHA class 2–3, expected to live > 1 year Only prevents SCD thereby reducing mortality Does not improve cardiac function Cardiac resynchronization therapy (CRT) with defibrillator LVEF≤ 35%, NYHA class 2–3, or on chronic IV infusion, expected to live > 1 year, left bundle branch block on ECG with QRS duration ≥ 150 ms Improves quality of life, reduce hospital re-admission, prevents SCD, reduce mortality Can improve cardiac function in ∼ 2/3 of cases
Can provide benefit with CRT-P (i.e., without defibrillation option)
↵12. Heidenreich PA, Bozkurt B, Aguilar D, et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol May 3 2022;79(17):e263-e421. doi:10.1016/j.jacc.2021.12.012.
In this issue




{kind=link}
Jump to section
- Article
- Abstract
- Practice Recommendations
- Background
- Classification
- Pharmacologic Therapy
- Renin-Angiotensin-Aldosterone System (RAAS) Inhibitors
- β Blockers
- Mineralocorticoid Receptor Antagonists (MRAs)
- Sodium-Glucose Cotransporter 2 Inhibitors (SGLT2i)
- Additional Medications and Therapies
- Management of Associated Conditions
- Conclusion
- Notes
- References
- Figures & Data
- References
- Info & Metrics