
Abstract
Background: Medical cannabis is commonly used for chronic pain, but little is known about differences in characteristics, cannabis use patterns, and perceived helpfulness among primary care patients who use cannabis for pain versus nonpain reasons.
Methods: Among 1688 patients who completed a 2019 cannabis survey administered in a health system in Washington state, where recreational use is legal, participants who used cannabis for pain (n = 375) were compared with those who used cannabis for other reasons (n = 558) using survey and electronic health record data. We described group differences in participant characteristics, use patterns, and perceptions and applied adjusted multinomial logistic and modified Poisson regression.
Results: Participants who used cannabis for pain were significantly more likely to report using applied (50.7% vs 10.6%) and beverage cannabis products (19.2% vs 11.6%), more frequent use (47.1% vs 33.1% for use ≥2 times per day; 81.6% vs 69.7% for use 4 to 7 days per week), and smoking tobacco cigarettes (19.2% vs 12.2%) than those who used cannabis for other reasons. They were also significantly more likely to perceive cannabis as very/extremely helpful (80.5% vs 72.7%), and significantly less likely to use cannabis for nonmedical reasons (4.8% vs 58.8%) or report cannabis use disorder symptoms (51.7% vs 61.1%).
Discussion: Primary care patients who use cannabis for pain use it more frequently, often in applied and ingested forms, and have more co-use of tobacco, which may differentially impact safety and effectiveness. These findings suggest the need for different approaches to counseling in clinical care.
Introduction
Chronic noncancer pain (CNCP) is a common reason for medical cannabis use in the United States.1⇓⇓⇓⇓⇓–7 While little is known about the perceived helpfulness of cannabis for patients who use it for pain, cannabis’ widespread use suggests it is viewed as a helpful primary or adjunctive treatment for some individuals. Although additional research is needed on the benefits of cannabis for pain, studies show a small but significant benefit of cannabis relative to placebo for CNCP.8⇓–10
Cannabis use is also associated with potential harms, which could be more marked in states with legal or medical cannabis, where various commercial cannabis products are available and marketed with minimal standardization of preparations.11 The harms of cannabis likely vary by product characteristics (eg, the ratio of THC [tetrahydrocannabinol] to CBD [cannabidiol]), mode of use (eg, ingestion vs application), and frequency of use. Depending on how patients use cannabis for pain, they may be more or less susceptible to adverse effects compared with patients who use cannabis for other reasons. For example, smoking cannabis may lead to respiratory complications, even in individuals who do not smoke tobacco,12⇓⇓⇓–16 and vaping cannabis can result in lung injury.17,18 Little is known about the safety of applied and ingested forms of cannabis, which are commonly used for pain.19 A dose-response relationship has been observed between cannabis consumption and the risk of psychosis and declines in psychosocial function,15,20⇓⇓–23 and more frequent cannabis use may increase the risk of cannabis use disorder (CUD).15,24 However, little research has explored cannabis use patterns and indicators of potentially problematic use in patients who use cannabis primarily for pain.
Roughly 8% to 24% of adults use cannabis at least once a month in states with medical and/or legal cannabis.25 With widespread cannabis availability in legal contexts, it is critical to evaluate the safety and effectiveness of real-world cannabis use for pain. Patients with pain may be older, have more comorbidities and more complex medication regimens than patients who use cannabis for other reasons; these characteristics likely impact the absorption and metabolism, and, therefore, the safety and effectiveness of cannabis.
This primary-care based study was designed to identify and quantify differences in characteristics, cannabis use patterns (mode and frequency), CUD symptoms, and perceived helpfulness of cannabis for patients who use cannabis primarily for pain compared with patients who use cannabis for other reasons.
Methods
Study Setting
This study was conducted in Kaiser Permanente Washington (KPWA), a large health plan and care delivery system. Medical cannabis has been legal in Washington state since 1998 and nonmedical use since 2012.26 This study was funded by the National Drug Abuse Treatment Clinical Trials Network.
Study Sample
The sample included primary care patients who responded to a survey on cannabis use.27 The original survey sample included 5000 patients selected from a representative cohort of KPWA patients aged ≥18 with primary care visits (January 28, 2019-September 12, 2019) and documentation of a routine cannabis screen (n = 108,950). Survey design, sampling, procedures, and sample characterization, including comparison of respondents to eligible primary care sample and nonrespondents, have been reported previously.27 The validated single-item screen asks about the frequency of past-year cannabis use (ie, none, less than monthly, monthly, weekly, and daily).28 Sample selection included patients who reported no past-year use, as well as random, stratified oversampling for Black, Indigenous, and other patients of color, and patients with weekly-to-daily cannabis use, to adequately account for the experiences of these subgroups who are often underrepresented in research.27 Of the 5000 invited to complete the cannabis use survey, 1688 (34%) responded. (See Lapham et al., 202227 for comparison of eligible sample and survey responders.) Participants consented to use of data from their electronic health records (EHRs). Informed consent assured survey results were confidential and that study data were protected by a Certificate of Confidentiality from the National Institutes of Health. The KPWA Institutional Review Board approved the study, including waivers of consent to identify the eligible sample, documentation of informed consent for survey respondents, and HIPAA (Health Insurance Portability and Accountability Act) authorization.
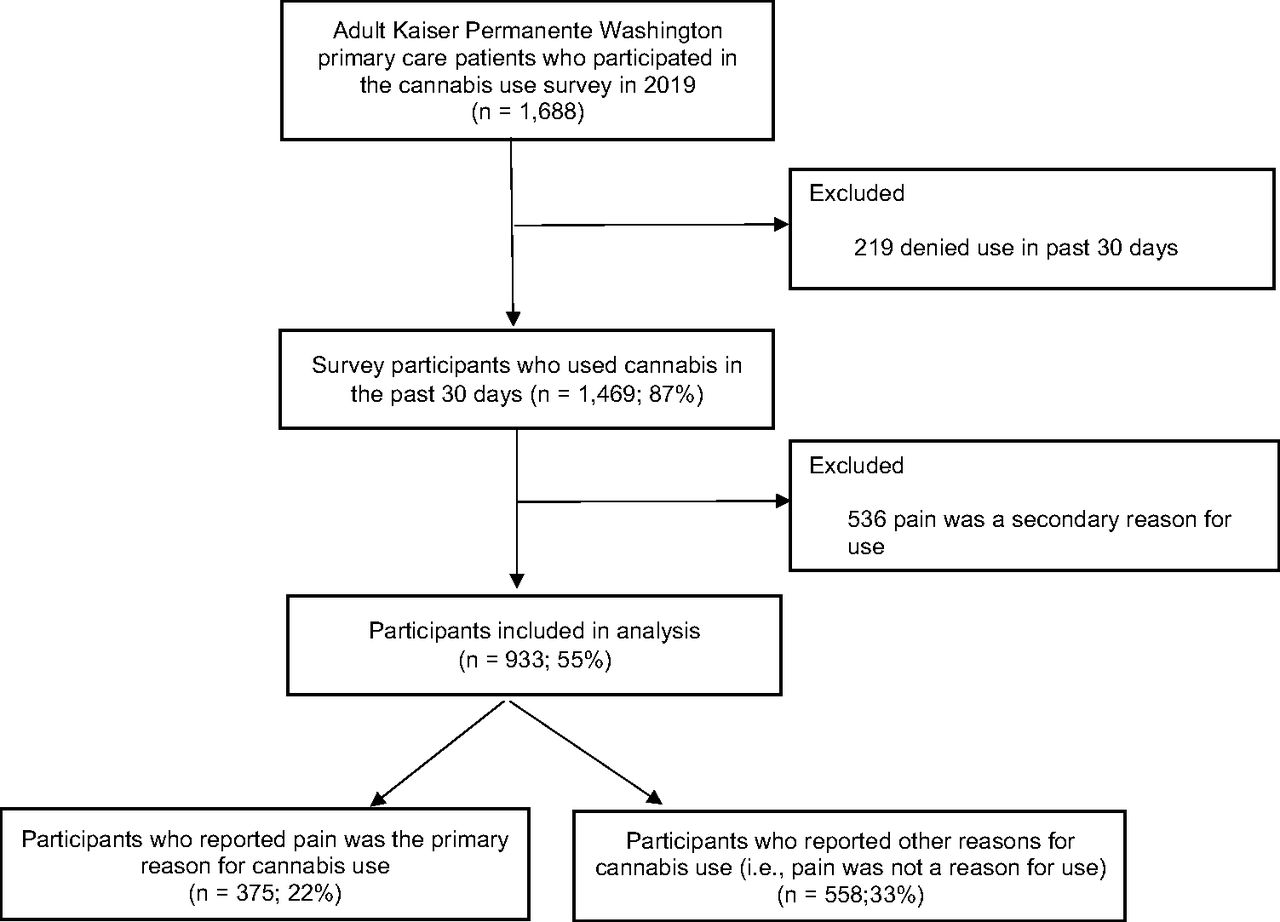
This study included respondents who reported past 30-day cannabis use (n = 1469) (Figure 1). Among these, the primary analyses were conducted comparing participants who reported pain as the primary reason for use (n = 375) to those who did not report pain as a reason for use (n = 558). In secondary analyses, we compared participants who reported pain as a reason for cannabis use, but not the primary reason (n = 536). (See Appendix Table 1 for instrument.)

Study population selection criteria.
Sociodemographic Characteristics of Survey Participants Who Used Cannabis for Pain and Who Used Cannabis for Other Reasons in the Past 30 Days
Data
Study data came from survey responses and EHRs. All research data were stored in limited access databases and deidentified before analysis.
Survey Measures
The cannabis survey was developed by an expert panel and pilot tested in a convenience sample of KPWA Health Research Institute colleagues. The survey included 2 to 75 items, depending on skip patterns, with de novo questions on reasons for cannabis use, mode and frequency of use, experience of CUD symptoms, and helpfulness of use. Participants could complete the survey online or by phone.
Participants reported whether cannabis use in the past 30 days was for medical, nonmedical, or both reasons for use (Question 1 in Appendix Table 1). Participants also reported whether they used cannabis to help manage any pain, which could include CNCP or other forms of pain; other symptoms or conditions (eg, seizures, nausea or vomiting); or none (Question 4 in Appendix 1). Those who reported more than 1 reason for cannabis use were asked to identify the reason they used it most often—that is, their primary reason for use (Question 5 in Appendix 1). Participants who reported pain as their only or primary reason for cannabis use were included in the pain as primary reason for use subgroup (hereafter referred to as use for “pain”), whereas those who reported reason(s) for use other than pain (including ‘none’ or ‘other’) were included in the other reason(s) for use subgroup (hereafter referred to as use for “other reasons”). Participants who reported pain as a reason, but not the primary reason, for cannabis use were designated as pain as the secondary reason for use subgroup (hereafter referred to as use for “pain – secondary”).
Participants were prompted to indicate modes of use and their most frequent mode of use in the past 30 days (‘smoke it,’ ‘vaporize it,’ ‘dab it,’ ‘eat it,’ ‘drink it,’ ‘apply it to the skin’ and ‘other.’). Participants were additionally asked for the typical times per week and typical times per day they used cannabis in the past 30 days, as well as how helpful cannabis has been for the reasons they use it (‘not at all helpful’, ‘slightly helpful,’ ‘somewhat helpful,’ ‘very helpful,’ or ‘extremely helpful’). In addition, participants were queried about symptoms of cannabis use disorder (CUD) in the past year, using questions from the Composite International Diagnostic Interview and based on Diagnostic and Statistical Manual of Mental Disorders, fifth Edition (DSM-5) CUD criteria.29 Lastly, participants were asked about their tobacco and nicotine use, employment status, and education.30
Electronic Health Record Measures
Clinical correlates of cannabis use, including CNCP diagnoses and substance use disorder diagnoses in the 2 years before the cannabis use survey completion date were identified from EHRs. CNCP diagnoses were defined as EHR documentation of 2 or more International Classification of Diseases-Tenth Revision (ICD-10) codes for similar pain types at least 30 days apart, or an ICD-10 diagnosis consistent with general CNCP.31,32 Participant age, gender, race, and ethnicity were also derived from EHR data available on the cannabis use survey completion date.
Analytic Approach
Descriptive statistics were used to characterize participants who used cannabis for pain and those who used cannabis for other reasons across demographic and clinical characteristics, mode-specific patterns of cannabis use, CUD symptoms, and perceived helpfulness of use. Between-group differences were estimated using c2 tests of independence or Fisher’s exact tests if cell sizes were <5 with an α level of 0.05. In participants who used cannabis for pain, we examined within-group patterns by mode of use and by perceived helpfulness.
Using multinomial logistic regression, we estimated the adjusted prevalence and relative risk ratio (RRR) of combined modes of cannabis use—inhale (smoke, vape, and dab), apply, ingest (eat and drink), or other—comparing participants who used cannabis for pain and those who used cannabis for other reasons. Using modified Poisson regression models,33 we estimated the adjusted prevalence and relative risk (RR) of 2 measures of cannabis frequency—times per day and days per week—again comparing participants who used cannabis for pain and those who used cannabis for other reasons. Poisson, rather than logistic, regression models were used to estimate relative rates because outcomes were expected to be common.34 Standard errors were calculated using a robust sandwich estimator to account for misspecification of the mean-variance relationship.33 All models were adjusted for demographic characteristics (age, gender, race/ethnicity, employment status, education) and other cannabis outcomes.
In sensitivity analyses, we compared sociodemographic characteristics between participants who used cannabis for pain and participants who used cannabis for other reasons to excluded patients who used cannabis for pain – secondary. We also conducted descriptive analyses of CUD symptoms excluding participants who only used cannabis in applied forms.
Analyses were conducted using Stata, version 15.1 (StataCorp LLC, College Station, TX).
Results
Among 933 participants included in primary analyses, 375 reported using cannabis for pain and 558 reported using cannabis for other reasons in the past 30 days.
Sociodemographic and Clinical Characteristics
Compared with participants who used cannabis for other reasons, those who used cannabis for pain were more likely to be aged ≥50, female, retired or have a disability, and have less than a bachelor’s degree (Table 1). The prevalence of CNCP diagnoses among participants who used cannabis for pain was more than double that of participants who used cannabis for other reasons (54.9% [206/375] vs 21.9% [122/558]; P = .001) (Table 2). Participants who used cannabis for pain had significantly higher prevalence of tobacco use disorder (16.0% vs 10.8%, P = .019) and were twice as likely to report that they smoke cigarettes every day (14.6% vs 7.2%, P = .001).
Chronic Pain and Substance Use Disorder Diagnosis History; Current Cigarette Smoking Status and Vaping of Tobacco/Nicotine; and Mode, Frequency, and Helpfulness of Cannabis Use in Survey Participants Who Used Cannabis for Pain and Who Used Cannabis for Other Reasons in the Past 30 Days
In sensitivity analysis, participants who used cannabis for pain – secondary (n = 536) were more like participants who used cannabis for other (nonpain) reasons than those who used cannabis for pain in age, employment, and disability status (Appendix Table 2). However, they were more likely to be female and have less than a bachelor’s degree, similar to participants who used cannabis for pain.
Cannabis Use Patterns
Participants who used cannabis for pain and those who used cannabis for other reasons endorsed an average of 4.1 (S.D. 2.4) and 2.5 (S.D. 1.8) reasons for use, respectively. Smoking was the most common mode of use for both groups (Table 2). Significantly more participants who used cannabis for pain reported applying cannabis (eg, lotion, ointment, patch, salve; 50.7% vs 10.6%; P < .001) and drinking cannabis (19.2% vs 11.6%; P = .001). Participants who used cannabis for pain were more likely to use it ≥3 times per day (47.5% vs 33.1%; P < .001) and ≥4 days per week (81.6% vs 69.7%; P < .001). These participants were also less likely to report their cannabis use was for nonmedical reasons only (4.8% vs 58.8%; P < .001). Across modes of use, most participants who used cannabis for pain used it for both medical and nonmedical reasons (Table 3).
Cannabis Use Patterns Among Survey Participants Who Used Cannabis for Pain in the Past 30 Days, by Each Mode of Use*
Cannabis Use Disorder Symptoms and Diagnoses
Participants who used cannabis for pain were less likely than those who used cannabis for other reasons to report experiencing any DSM-5 CUD symptom in the past year (51.7% vs 61.1%; P = .005) (Table 4). These participants were also less likely to meet DSM-5 criteria for moderate or severe CUD (5.9% vs 21.0%; P < .001). These findings were robust in sensitivity analysis that excluded participants who apply cannabis only (Appendix Table 3).
Past-Year Experience of Cannabis Use Disorder (CUD) Symptoms and Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5) CUD Category Among Survey Participants Who Used Cannabis for Pain and Who Used Cannabis for Other Reasons in the Past 30 Days
Helpfulness of Cannabis Use
Perceived helpfulness of cannabis was high in both groups, with participants who used cannabis for pain being significantly more likely to report cannabis as very/extremely helpful compared with those who used it for other reasons (80.5% vs 72.7%; P = .010) (Table 2). Among participants who used cannabis for pain, those who found cannabis very/extremely helpful were significantly more likely than those who found it slightly/somewhat helpful to endorse smoking as a mode of cannabis use and use it 4 to 7 days per week (Table 5).
Past 30-Day Helpfulness of Cannabis among Survey Participants Who Used Cannabis for Pain, by Mode and Frequency of Use and Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5) Cannabis Use Disorder (CUD) Category
Adjusted Analysis
In adjusted analyses comparing participants who use cannabis for pain to participants who use cannabis for other reasons, applying cannabis and ingesting (eating, drinking) cannabis were significantly more likely than inhaling (smoking, vaping, dabbing) cannabis (Appendix Table 4). RRRs were 109.5 (95% CI, 21.3 to 562.9; P < .001) for cannabis application and 2.0 (95% CI, 1.3–3.1; P = .003) for ingestion. After adjustment, participants who used cannabis for pain had a higher risk of using cannabis more than twice per day and 4 to 7 days per week than those who use cannabis for other reasons. RRs were 1.4 (95% CI, 1.2-1.6; P < .001) for more than twice daily use and 1.1 (95% CI, 1.0 to 1.2; P = .025) for use 4 to 7 days per week.
Discussion
In this study of primary care patients who responded to a cannabis use survey and reported past 30-day cannabis use, participants who used cannabis for pain were older and more likely to be female, retired/have a disability, have a CNCP diagnosis, smoke tobacco cigarettes, and have a tobacco use disorder than participants who used cannabis for other reasons. Further, participants who used cannabis for pain were more likely to apply and ingest cannabis and use it frequently, and less likely to describe their cannabis use as ‘nonmedical’ and meet CUD criteria. Most participants in both groups perceived cannabis use as helpful, with a slightly greater proportion of those who used it for pain reporting it as very or extremely helpful.
To balance the harms and benefits of cannabis use for pain and guide patients, clinicians may find it helpful to assess patients’ reasons for cannabis use; modes, frequency, and perceived helpfulness of use; and CUD symptoms. This approach is consistent with shared patient-clinician decision making guidance for other substances lacking clear evidence of benefits and risks. For example, although evidence on the effectiveness of opioid therapy for CNCP management continues to develop, the Centers for Disease Control and Prevention’s “Clinical Practice Guideline for Prescribing Opioids for Pain” suggests clinicians evaluate the risks and benefits of opioid use with patients before initiating and throughout opioid therapy.35 A similar framework could be applied to cannabis use for pain. Clinicians should also carefully assess nicotine and tobacco use among patients who use cannabis for pain and provide nicotine and tobacco cessation counseling and medications as indicated.
Several of our findings are congruous with prior research. Prevalence studies show that CNCP is more common in females, older individuals, and those with chronic conditions,36,37 consistent with the characteristics of participants who used cannabis primarily for pain in this study. Tobacco use disorder and nicotine use rates are high among people with CNCP,37⇓⇓–40 concordant with our findings that a higher proportion of participants who used cannabis for pain had a diagnosis of tobacco use disorder. Finally, prior research involving adult primary care patients41 is consistent with our observations that most participants who used cannabis for pain or other reasons found it helpful. With regard to our finding that participants who used cannabis for pain used it more frequently and were more likely to report tobacco use, yet were less likely to report CUD symptoms, it is conceivable that pain requires more frequent dosing of cannabis, that people with pain may use other substances in addition to cannabis for pain, and that they are less likely to report or develop CUD symptoms due to use for pain.
Our findings highlight the need for effectiveness and safety studies of the risks, benefits, and helpfulness of ingested cannabis, given the prevalence of this mode of use for pain and lack of evidence on its safety. This is particularly important given the higher age, comorbidity prevalence, and frequency of use among patients who use cannabis for pain in our study. Further etiologic, epidemiologic, and intervention research on cannabis and tobacco and nicotine product use is also needed. Studies have noted a potential causative role of tobacco in the etiology of painful conditions39 and possible analgesic effects of nicotine.40 Improved understanding of the interactive effects of tobacco and cannabis use on health could advance the field. Although patients generally perceive cannabis as helpful,41,42 research into perceived helpfulness by pain type and mode and frequency of use could generate hypotheses for formal effectiveness studies, and identify areas for safety research.
This study has several limitations, including the inability to infer causation due to the cross-sectional design. For some comparisons, stratification by mode of use within the 933 participants compared in the primary analysis resulted in limited statistical power. Although cannabis potency may influence patterns and health effects of use, we could not reliably assess potency or the THC and CBD content of cannabis used with this survey design. Although patients were assured of confidentiality, some nonresponse could be attributed to patients not wanting to disclose aspects of their cannabis use on a survey. Depending on participant responses, the number of survey questions ranged from 2 to 75, with more questions potentially influencing completion rate. However, we observed limited item nonresponse. Although survey questions were developed through expert consensus and pretested, it is possible that interpretations of cannabis use for pain varied across participants with different behavioral and lifestyle characteristics. Although a 34% response rate is consistent with health survey research,43,44 nonresponse may limit the external validity of our findings. Oversampling patients from minoritized racial and ethnic groups and with more frequent cannabis use allowed us to obtain perspectives from important subgroups, but may limit generalizability to primary care populations. Furthermore, this study was conducted in an integrated health system in a state with legal cannabis use; findings may not extrapolate to other health systems and settings.
In conclusion, in a state with legal cannabis use, primary care patients who used cannabis for pain used cannabis through different modes and more frequently than patients who used cannabis for other reasons. These use patterns and patient perceptions should inform clinician and patient discussions and future effectiveness and safety studies about cannabis use for pain.
Cannabis Use Survey Items
Sociodemographic Characteristics of Survey Participants Who Used Cannabis for Pain, for Pain – Secondary, and for Other Reasons in the Past 30 Days
Sensitivity Analysis of Past-Year Experience of Cannabis Use Disorder (CUD) Symptoms and Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5) CUD Category Among Survey Participants Who Used Cannabis for Pain and Who Used Cannabis for Other Reasons in the Past 30 Days, Excluding Participants Who Apply Cannabis Only (n = 21)
Adjusted Analysis*
Acknowledgments
We thank Udi Ghitza, PhD, with the National Institute on Drug Abuse for support of this study. We also thank the members of the multidisciplinary expert panel who contributed to the development of the cannabis use survey, including Steffani Bailey, PhD (Oregon Health and Science University), Kim Hoffman, PhD (Oregon Health and Science University), Michael Horberg, MD, MAS (Mid-Atlantic Permanente Research Institute), Mark Ilgen, PhD (University of Michigan; VA Ann Arbor Healthcare System), Erin McClure, PhD (Medical University of South Carolina), and Rosalie Liccardo Pacula, PhD (University of Southern California).
Appendix.
Notes
This article was externally peer reviewed.
Funding: This research was supported by the National Institute on Drug Abuse under award number UG1DA040314 (NIDA Clinical Trials Network Protocol #0077). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Conflict of interest: Ms. Ford, Dr. Lapham, Dr. Matson, Ms. Luce, and Ms. Oliver have no conflicts of interest to declare. Dr. Binswanger received royalties from UptoDate (Wolters Kluwer) and is employed by the Colorado Permanente Medical Group, which provides primary care and specialty care. She has no other conflicts of interest to declare.
To see this article online, please go to: http://jabfm.org/content/36/6/996.full.
- Received for publication April 27, 2023.
- Revision received July 17, 2023.
- Accepted for publication July 24, 2023.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.