
Abstract
Background: Recently, the use of electronic cigarettes increased sharply, leading to increased e-cigarette, or Vaping Product Use-Associated Lung Injury (EVALI), and other acute pulmonary conditions. There is an urgent need for clinical information about e-cigarette users to identify factors that contribute to EVALI. We developed an e-cigarette/vaping assessment tool (EVAT) that was integrated into the Electronic Health Record (EHR) of a large state-wide medical system and initiated a system-wide dissemination and education to support its use.
Methods: EVAT documented current vaping status, history, and e-cigarette content (nicotine, cannabinoids, and/or flavoring). Educational materials and presentations were developed via a comprehensive literature review. EVAT utilization in the EHR was assessed quarterly. Patients’ demographic data and clinical site name were also collected.
Results: The EVAT was built, validated, and integrated with the EHR in July 2020. Live and virtual seminars were conducted for prescribing providers and clinical staff. Asynchronous training was offered using podcasts, e-mails, and Epic tip sheets. Participants were informed about vaping harm and EVALI and instructed on the use of EVAT. As of December 31, 2022, EVAT was used 988,181 times, with 376,559 unique patients evaluated. Overall, 1,063 hospital units and affiliated ambulatory clinics used EVAT, including 64 Primary Care, 95 Pediatrics, and 874 Specialty sites.
Conclusions: EVAT was successfully implemented. Continued outreach efforts are needed to further increase its usage. Education materials should be enhanced to help providers to reach youth and vulnerable populations and connect patients to the tobacco treatment resources.
- Adolescent
- Cannabinoids
- e-Cigarette
- Electronic Health Records
- Lung Injury
- Maryland
- Nicotine
- Vaping
- Vulnerable Populations
Introduction
The use of electronic cigarettes has increased dramatically in recent years.1 E-cigarettes typically deliver nicotine, tetrahydrocannabinol (THC), cannabidiol (CBD), flavorings, and other additives via an inhaled aerosol, or vapor.2 E-cigarette design has evolved from cigarette lookalikes to sleek designs such as JUULs, making it attractive to youth.2,3 E-cigarettes were the most used non-cigarette tobacco product (4.5%) in 2019, with the highest prevalence among 18- to 24-year-old smokers (9.3%).4 E-cigarette usage is associated with smoking initiation5,6 and potentially can lead to dangerous pulmonary injuries, such as E-cigarette, or Vaping Use-Associated Lung Injury (EVALI).7⇓⇓–10 Because e-cigarette use has escalated so quickly, there is an urgent need for clinical information on users over time to understand associations between use and health consequences. Systematic screening and consistent, standardized documentation on the use of e-cigarettes in the electronic health record (EHR) can help clinicians facilitate nicotine treatment discussions, identify adverse events, leverage population surveillance, and reveal novel insights around usage behavior.11
In University of Maryland Medical System’s (UMMS) Epic EHR, general tobacco screening is conducted routinely as a part of the social history. Recently, tobacco use was incorporated into the “Vital Signs” section as a fifth vital sign with a hot link to the tobacco history section making it easier for use by clinical staff. Counseling patients on tobacco treatment and informing them about available resources was and remains discretionary based on the providers’ and patients’ priorities during the visit. One of the major tobacco treatment resources is a nationwide tobacco Quitline program that usually is administrated by the state health departments.12 In December 2017, UMMS introduced an EHR-based electronic referral system to the Maryland Quitline that utilized a clinical decision support tool and simplified patients’ access to the free evidence-based tobacco counseling and treatment.13,14 UMMS tobacco treatment options were enhanced in August 2019 when the University of Maryland Medical Center (UMMC) Tobacco Health Practice (THP) was established, and electronic referral to this clinic was built into the tobacco screening section in the EHR.15 However, information on use of e-cigarettes and vaping was not collected systematically and in sufficient depth and was limited to single tab within a “tobacco use” section. To meet an urgent need to collect information about e-cigarette users, we developed and integrated an e-cigarette and vaping assessment tool (EVAT) within the UMMS EHR. This study describes the results of the first 2 years of EVAT implementation, dissemination of knowledge and a system-wide uptake.
Methods
Ethics
The exempt status of the study was confirmed by the University of Maryland Baltimore Institutional Review Board (reference number HP-00093456).
UMMS Description
UMMS is a 13-hospital network, forming one of the largest health care systems in Maryland with ambulatory multidisciplinary clinics in more than 150 locations across the state, including UMMC’s main campus, UMMC Midtown Campus, and St. Joseph Medical Center located in Baltimore city and vicinity as well as regional Centers in Upper Chesapeake, Eastern Shore, Baltimore-Washington, Prince George’s, and Charles counties areas.16 UMMS is providing access to medical care for residents in urban, suburban, and rural settings, with a high proportion of minority, lower socioeconomic status patients, and high rates of tobacco use.
EVAT Development
The content, layout, and location of the EVAT was built with advice from the Epic manufacturer using Epic shared resources and examples from other health system, and followed the evidence based guidelines in this domain.17,18 A mock-up was developed, tested, and validated by the Epic IT team before releasing EVAT for general use.
A screenshot of the EVAT is shown in Appendix Figure 1. Discrete choices were provided to document current vaping status (current every day, current someday, former, never user, etc.). Start and quit dates and passive exposure were recorded if applicable. For those who ever vaped, information about substances such as nicotine, THC, CBD, flavoring, or other compounds was collected. Additional comment options allowed users to document device modifications or whether the patient was “dabbing” or “dripping.” A “Yes/No” check box was available if the provider performed counseling for the patient about e-cigarette use, and an open text box to write additional information provided by patients. The section was designed to be completed by a clinical provider and was available for hospital units and affiliated ambulatory sites. However, it was not a required component of the EHR.

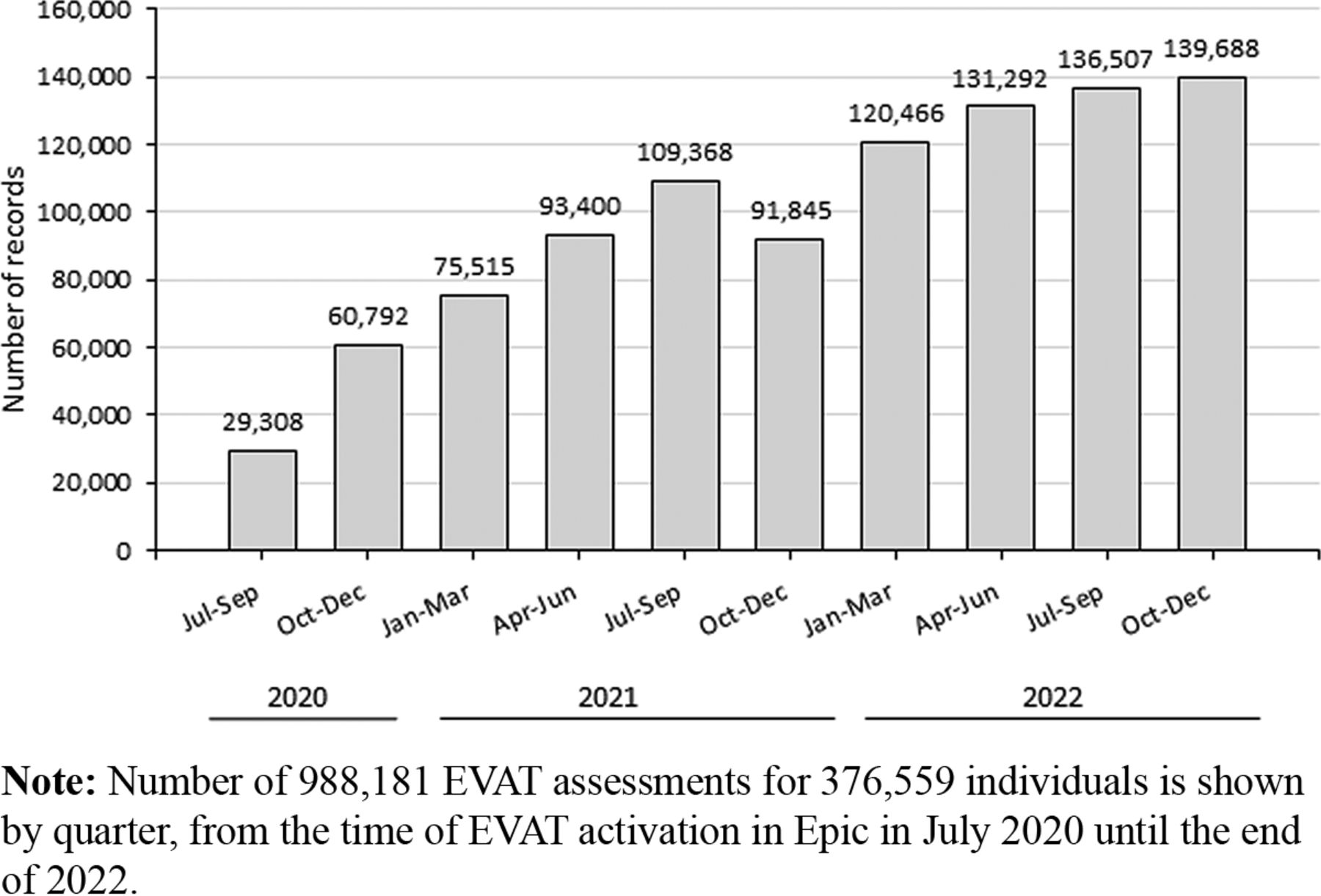
Vaping assessment tool utilization in UMMS practices (July 2020 – December 2022).
Dissemination and Education Efforts
For dissemination, the research team contacted department chairs, clinic administrators, and colleagues seeking opportunities to present educational materials for physicians, nursing staff, and medical assistants at grand rounds, clinical and faculty meetings, and special tobacco-related events. Seminars for prescribers were delivered by a physician educator; those for nursing staff and medical assistants were delivered by a nurse tobacco coach. Educational materials and presentations were developed via a comprehensive literature review.7⇓⇓–10,19⇓⇓–22 The clinical team focused on tobacco use disorder (TUD) as a chronic condition requiring evidence-based care. Just as clinicians do not ask patients with diabetes to get better on their own, TUD treatment should use an “opt-out” approach.23 Seminars reviewed information on the components of e-cigarettes, physiologic effects of vaping including EVALI and obstructive lung disease, the health impacts of e-cigarette use, an overview of EVAT including the steps for completing it in the EHR, resources available for patients to help with reducing or abstaining from both cigarette and e-cigarette use, and use of the tobacco fifth vital sign in the EHR. Seminars were held virtually, hybrid (virtual and in-person), or in-person. Tip sheets and recorded PowerPoints were provided for asynchronous learning. The team also partnered with a pediatric pulmonologist who was evaluating youth patients who vaped. A warm handoff model was created to ensure that these patients could be transferred to UMMC THP on reaching adulthood.
Data Extraction and Analysis
Data on EVAT utilization were extracted from the EHR quarterly including patient’s medical record number, name, age, race, ethnicity, tobacco use status, medical problems, date of the evaluation, and names of the clinical sites. Data were analyzed using SAS 9.4 software (SAS Institute Inc., Cary, NC). Associations between patients’ demographic characteristics and use of e-cigarettes were assessed using Chi-square tests. Significance level was established at α = 0.05.
Results
The team delivered multiple seminars (in-person, hybrid, and virtual) to engage providers from departments across UMMS. These presentations were for general practitioners (Internal Medicine, Family Medicine, and Pediatrics) as well as specialists (Radiation Oncology, Otolaryngology, Thoracic Surgery, Cardiology, Psychiatry, Cancer Center, and others). In addition, sessions were held for nursing and other clinical staff. The priority was given to the departments and personnel that are likely to have high proportion of smoking and vaping patients such as family medicine, psychiatry, and youth/adolescent clinical programs. Each seminar was customized for the department and the disease presentations common in their patient population.
Between its launch in July 2020 and December 31, 2022, the EVAT was used 988,181 times with 376,559 unique patients evaluated. EVAT usage increased from 29,467 times in June-September 2020 to 139,688 times during October-December 2022 (Figure 1). Median number of evaluations was 2 per patient, with 38.1% evaluated once, and 39.1% 3 or more (up to 10) times. EVAT utilization by the UMMS hospital and ambulatory sites is shown in Table 1. Overall, 1,063 sites from the entire UMMS performed screenings. The highest number of assessments was performed in primary care and medical specialties, with emergency department and surgical specialties contributing substantially.
EVAT Utilization by Hospital and Ambulatory Sites at UMMS (July 2020 – December 2022)
Among evaluated patients, 13.4% were teenagers and young adults (10 to 24-year-old), 60.5% were White and 28.5% were Black (Table 2). Patients 18 to 24-year-old were most likely to ever vape (18.1%). Males vaped more often than females (7.3% and 5.5% respectively). Among racial and ethnic groups, the highest proportion of those who ever vaped were multiracial, American Indian/Alaskan Native, and Native Hawaiian/Pacific Islander patients, although these groups comprised only a small proportion of the total population. White patients vaped more often than Black (7.4% and 4.3% ever vaped respectively). Among 16,243 individuals who reported using e-cigarettes at their last (or only) evaluation, 5,890 (33.5%) used other tobacco concurrently compared with 29.2% who never smoked.
Demographic Characteristics of UMMS Patients Evaluated for e-Cigarette Use/Vaping in July 2020-December 2022
When data on the EVAT utilization were cross-checked with a database of UMMS patients referred electronically to the Maryland Quitline, we found that among 17,140 patients who reported to be current e-cigarette users, 174 (1.02%) were referred to the Quitline in 2020 to 2022. In addition, 15 patients (0.09%) enrolled in UMMC THP.
Discussion
E-cigarettes are relatively new, and their management and treatment protocols are evolving. Continuous education about e-cigarettes and vaping harm, effective counseling techniques, and proper documentation are needed to address the vaping problem. We expected that a standardized data collection on use of e-cigarettes within the EHR together with education organized for providers and clinical staff would improve quality and efficiency of patient-centered communication and save providers time.18,24,25
The EVAT was successfully integrated into the EHR across all UMMS sites, including inpatient units, outpatient clinics, ambulatory sites, emergency departments, etc. The study by Patnode et al. presents a synthesis of 67 systematic reviews, which suggests that the primary care office is the optimal site for screening for tobacco and nicotine use, and for referrals to counseling.26 Review of our utilization data demonstrates that family physicians are likely to be the highest users of EVAT in the entire health system. This is because Family Medicine practices within UMMS are patient-centered medical homes and use the institutionally required tobacco metrics, which mean that all patients are screened for tobacco and vaping and referred for counseling as needed.
However, screening of youth had not yet reached a sufficient volume at UMMS. Among 21,721 10- to 17-year-old patients evaluated with EVAT, only 7,179 were screened in pediatric clinics. Screening adolescent patients represents a significant challenge, partially due to competing priorities during encounters, age limitations initially present in EVAT, and lack of knowledge of EVAT among pediatric providers. The environment in which a screening is conducted with a child, and questions about vaping history should be considered carefully to ensure accurate responses. Pediatricians should receive more specific education and training that would empower them to conduct an adequate screening and provide treatment options to adolescent patients. We conducted presentations for pediatricians and engaged a pediatric pulmonologist to amplify our message to pediatricians. However, more needs to be done to equip clinicians in adolescent clinics with knowledge and resources to address the vaping epidemic among the youth.
Demographic characteristics of the patients who were screened using EVAT provided a good representation of the diverse Maryland population with 60.5% White and 28.5% Black, whereas Asian and Hispanic populations were slightly underrepresented compared with 2020 Census data.27 This discrepancy could reflect racial composition of the population served by UMMS in its locations. An unadjusted estimated current vaping rate of 4.3% in our study population was comparable with state-wide data (4.2% adults in 2018).28 The highest proportion of current and former e-cigarette users in our population was observed in 18- to 24-year-old individuals. This finding is in line with research showing that past 30-day use has more than doubled among 18- to 24-year-olds from 2013 to 2014.3 The trends for racial distribution of current users were also comparable with nationwide data, although proportions of White (5.2%) and multiracial (8.3%) users were higher in our population than nationwide estimates (2.8% and 4.5% respectively).29
Although EVAT was successfully implemented at UMMS, more work is needed to act on the results of the screening, including connecting patients to available tobacco treatment resources. Numbers of electronic referrals to the Quitline was low. Currently, EVAT is a standalone tool, and does not directly connect with the e-referrals to the Quitline or other treatment options. Although screening for tobacco use is mandatory, counseling and referral to the tobacco use treatment is currently optional at UMMS and remains at the discretion of the individual providers. In addition, UMMC THP’s in-person visits are only available at one site (UMMC Midtown). Although prior care at Midtown is not a prerequisite for clinic enrollment, those without transportation to the clinic are limited to virtual visits. This is an opportunity to improve EVAT with a direct link to e-referrals to the Quitline and UMMC THP, as well as an opportunity for more focused clinicians’ education and intervention.
There are several study limitations. The data are derived from real-life clinical encounters rather than a formally designed study, therefore there was no consistency in the frequency of evaluations, time between evaluations and overall follow-up time. This precluded formal longitudinal study to estimate rates of quitting or switching to conventional tobacco products. In addition, we could not determine denominator to estimate probability of the patient to be screened for the use of e-cigarettes.
Our experience and observations are from one health system and may not be applicable to all health systems. Moreover, only individuals seeking medical care were assessed, thus not representing the general population.
In conclusion, physicians and other practitioners must understand emerging trends in e-cigarette use and vaping and learn about the best practices to counsel their patients about potential harms and options for treatment. Consistently recording this information in the EHR can support a more nuanced understanding of the long-term implications of e-cigarette use and vaping, especially in youth and underserved racial and ethnic minority patients. Continued outreach efforts encouraging prescribers and nonprescribing staff to use EVAT will increase the number of patients who receive counseling and referrals to treatment.
Acknowledgments
The authors thank Neil M. Siegel, MD, and Vigfus Viffusson, BFA, for informatics and information technology support.
Appendix.Appendix Figure 1: A screenshot of the e-cigarette/vaping assessment tool in Epic EHR.

Discrete choices were provided to document current vaping status (current every day, current someday, former, or never user, etc). Start and quit dates and passive exposure were recorded if applicable. For those who ever vaped, information about substances such as nicotine, THC, CBD, flavoring, or other compounds was collected. Yes/No check box was available if the provider performed counseling for the patient about e-cigarette use, and an open text box to write additional information provided by patients.
Notes
This article was externally peer reviewed.
Funding: This project is supported by the National Institutes of Health, Grant number 3P30CA134274-13S5 to study the long-term impacts of EVALI and related diseases.
Conflict of interest: The authors have no conflicting or competing interests.
To see this article online, please go to: http://jabfm.org/content/36/3/405.full.
- Received for publication December 6, 2022.
- Revision received February 8, 2023.
- Accepted for publication February 13, 2023.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Re: Integrating a Systematic, Comprehensive E-Cigarette and Vaping Assessment Tool into the Electronic Health Record
- Response: Re: Integrating a Systematic, Comprehensive E-Cigarette and Vaping Assessment Tool into the Electronic Health Record
- Research Addressing the Ongoing Changes in the Practice of Family Medicine