
Abstract
Background: Primary care level close monitoring of mild COVID-19 patients has shown to provide a risk reduction in hospitalization and death. We aimed to compare the risk of all-cause death among COVID-19 ambulatory patients who received and did not receive telephonic follow-up in primary health care settings.
Methods: A secondary database analysis, 2-group comparative study, was conducted with data from the medical information systems of the Mexican Institute of Social Security. A total of 1,498,808 ambulatory patients aged 20 years old and over and with laboratory confirmed SARS-CoV-2 by PCR or rapid antigen test were analyzed. Of them, 535,898 (35.8%) where followed by telephonic calls. The cases were attended from October 14, 2020, to April 10, 2022. Death incidence was evaluated. To assess the association between death and telephonic follow-up we calculated risk ratio using a multivariate logistic model.
Results: Case fatality rate was 1.29% in the patients who received telephonic follow-up and 2.95% in the cases who did not receive phone calls. Medical history of chronic kidney disease, COPD, cardiovascular disease, tobacco consumption and diabetes were associated with increased risk of death. In the multivariate model, telephonic follow-up was associated with lower risk of all-cause death, with an adjusted risk ratio of 0.61 (95% confidence interval from 0.59, 0.64).
Conclusion: Our data suggest that telephonic follow-up is associated with a risk of death reduction in adult outpatients with mild COVID-19, in the context of a multimodal strategy in the primary health care settings.
Introduction
The Coronavirus Disease 2019 (COVID-19) pandemic has placed numerous challenges for health care systems.1 Primary care programs have been implemented to treat COVID-19 cases, to reduce severe cases through different interventions, such as smartphone applications, telemedicine, telephonic follow-up and remote oximeter monitoring as well 2⇓⇓–5.
The Mexican Institute of Social Security (IMSS) is the main health institution in Mexico and the largest Latin-American social security system. Nowadays, IMSS provides health care, economic assistance, and social services to about 68 million affiliates, that is 54% of mexican population6. As of October 2020, the IMSS implemented a telephonic follow-up strategy to favor patient’s home isolation and timely hospitalization of the COVID-19 cases. The patients with mild COVID-19 at the initial medical consultation (without pneumonia signs and with oxygen saturation greater than 90%), were sent to home isolation for recovery and follow up. For each patient with COVID-19, a family doctor made daily telephone calls, with the aim of evaluating their health status and identifying data of clinical worsening. If so, the patient was quickly referred to the hospital. If by the tenth day patients did not get worse, follow-up was concluded.
A previous report from our group found that a multimodal strategy in the primary care setting reduced the risk of hospitalization and death combined in 28,048 adult outpatients with mild COVID-19. This strategy consisted of providing, whether patients agreed, telephonic follow-up and medical kits containing, besides an information brochure and a pulse oximeter, medications for symptomatic relief and face masks. However, the sample size was not enough to clarify if the risk was also associated with the death alone7. So, in this study, we aimed to compare the risk of all-cause death in COVID-19 ambulatory patients who received and did not receive telephonic follow-up, in the context of the above-mentioned multimodal strategy.
Materials and Methods
Study Design and Population
A secondary data analysis, 2-group comparative study, was conducted with data from the medical information systems of the IMSS. The analyzed database integrated information from Family Medicine Information System (SIMF) and the Online Epidemiologic Surveillance System (SINOLAVE). The SIMF collects information regarding clinical data of every patient, as well as their diagnosis and follow-up. The SINOLAVE contains COVID-19 suspected cases data as underlying medical conditions and laboratory test results. Both systems are implemented across the 1530 IMSS primary health care units encompassed across the Mexican territory.
A total of 1,498,808 ambulatory patients aged 20 years and over with laboratory confirmed SARS-CoV-2 by PCR or rapid antigen test identified between October 14, 2020, to April 10, 2022, were included. This period encompasses from the second to fourth epidemic waves in Mexico.
For each patient we obtained information regarding age, sex, occupation, previous medical conditions (such as hypertension, obesity, diabetes among others), geographical region (north, center and south) and telephonic follow-up. For emergency department attention, intubation, hospitalization and all-cause death outcomes, data from hospital and death registers, were also obtained and verified. For this last supplementation, data from the Virtual Center in Emergencies and Disasters (CVOED) platform and from the Hospital Discharges System (SUI13) were used. The first system data derived from the COVID-19 IMSS hospitals while SUI13 included information from the 251 second care level and 25 tertiary health care hospitals.
Statistical Analysis
We compared patient’s characteristics according to the telephonic follow-up using the Chi-square test. Incidence of all-cause death was also calculated. To evaluate the association between variables and all-cause death, crude Relative Risk (RR) with 95% Confidence Interval (95% CI) were obtained in the bivariate analysis. Finally, to adjust the RR for telephonic follow-up and all-cause death, we constructed a multivariate logistic model, including the variables that were significant in the bivariate analysis. Statistical analysis was conducted using Stata version 14.
Ethical Statement
All procedures followed were in accordance with ethical standards of the institutional and national laws and with the 1964 Helsinki declaration and its later amendments.
In this research neither patient follow-up nor subject interviews were conducted. Given that the study was based only in the use of anonymized data from institutional medical information systems and patients were not involved, this research was determined as exempt of reviewing by the Institutional Review Board. Formal informed consent was not required. No external database linkage was performed.
Results
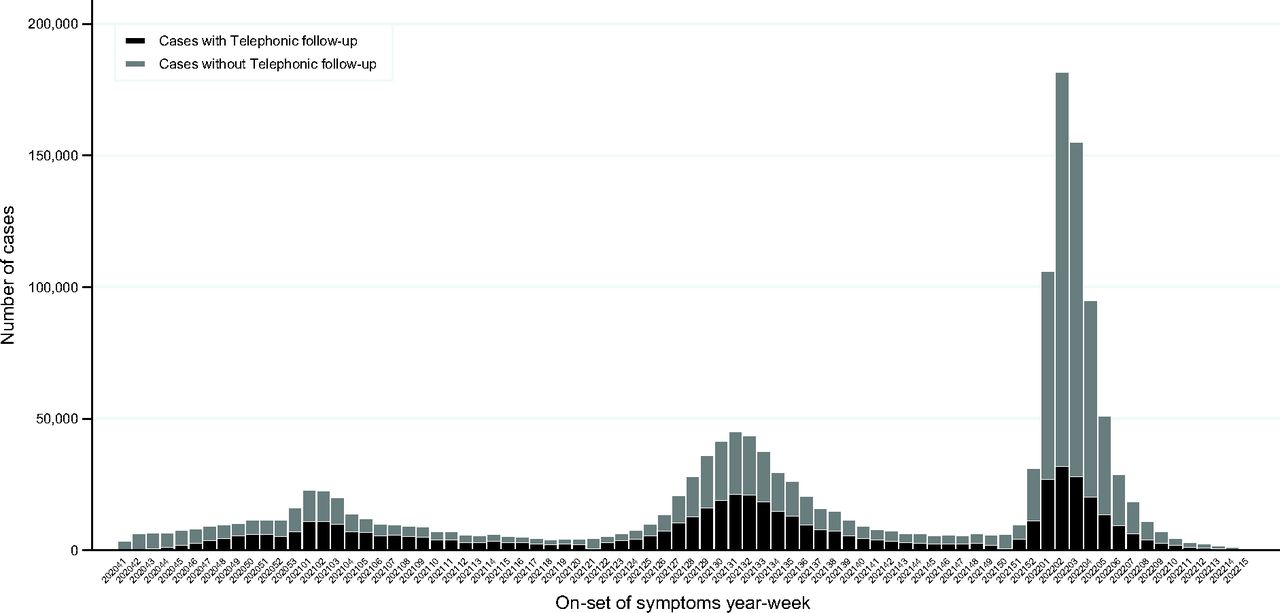
Of the total of 1,498,808 laboratory confirmed SARS-CoV-2 ambulatory patients included in this analysis, 535,898 (35.8%) were followed by telephonic calls. The majority of cases occurred during the fourth epidemic wave (January 2022), followed by the third wave (summer 2021). The second wave (winter 2020) had the lowest number of cases (Figure 1).

Weekly distribution of the number of COVID-19 cases, in the comparison groups.
Compared with patients without follow-up, patients followed by telephonic calls had higher frequency of previous medical conditions including obesity, hypertension, diabetes, and tobacco consumption, but lower frequency of emergency department visits. Incidence of all-cause death was 1.29% in patients who received telephonic follow-up and 2.95% in those who did not receive phone calls (Table 1).
Patients’ Characteristics According to the Study Group
In the bivariate analysis, hospitalization, emergency department attention, intubation, and age showed the highest risk of all-cause death. Medical history of chronic kidney disease, COPD, cardiovascular disease, tobacco consumption and diabetes were also associated with an increased risk of all-cause death. Patients with onset of symptoms during the 4th wave and telephonic follow-up showed lower risk of all-cause death (Table 2).
Association between All-Cause Death and the Patient’s Characteristics
Given the imbalances on comparison groups and to adjust the association between telephonic follow-up and the risk of all-cause death, a logistic model was computed. In this multivariate model, telephonic follow-up was associated with lower risk of all-cause death, with an adjusted RR of 0.61 (95% CI from 0.59 to 0.64) (Table 2).
Discussion
In the present study, we have shown that telephonic follow-up by family medicine physicians is associated with a reduction of all-cause death in outpatients with mild COVID-19.
As previously mentioned, the COVID-19 pandemic has led to changes in the methods of primary health care delivery including telemedicine, remote monitoring, and telephonic follow-up8–9.
A similar study was conducted in South-West England during the first wave pandemic in 2020. From a total of 70,431 COVID-19 adults studied, 10,891 patients received telephone consultation and 642 face-to-face consultation. Incidence of all-cause death were 5.8% and 12.5% respectively (risk ratio 0.46). Our crude relative risk was very similar (0.44), but our all-cause death incidence was lower than the other study. This last situation could be explained because the English study included cases from the first pandemic wave, the most severe, when no vaccinations were available. Like our results, the South-West England study also found differences among groups, with higher frequency of comorbidities but lower rates of hospitalization in patients with telephonic consultations compared with face to face consultations10.
Two small studies conducted in Spain, evaluated hospitalization rates in COVID-19 patients followed by telephone during 2020. The first study found an incidence of 15% from 301 patients11 and the second reported a hospitalization incidence of 17% from 453 COVID-19 outpatients12. Again, this high hospitalization rates could be explained by the most severe COVID-19 that occurred during the first wave.
Our study should be contextualized in relation to its limitations. First, our observational design has lower validity degree compared with clinical controlled trials. Second, since our study was based on the use of institutional databases, which have been not designed for research purposes, main variables were obtained from the real-life strategy, including their inherited biases. Moreover, neither level of family support data, medical kit delivery nor specific medication prescription were available. And third, the imbalances among comparison groups were also another limitation in our report, however, after adjusting in the multivariate analysis, a similar relative risk association was found. Despite these important limitations, our study analyzed almost 1.5 million subjects, which is a very considerable sample size, that supports our conclusions. To our knowledge, this is the first report with a sample of such magnitude.
Conclusions
Our data suggest that telephonic follow-up is associated with a risk of death reduction in adult outpatients with mild COVID-19, in the context of a multimodal strategy in the primary health care settings. Given that our results are based on the IMSS experience, it is important to point out that the telephonic follow-up impact may vary according to differences among health care systems.
Acknowledgments
We gratefully acknowledge to Dirección de Innovación y Desarrollo Tecnológico of the IMSS for their technical support to this project.
Notes
This article was externally peer reviewed.
Funding: None.
Conflict of interest: None.
To see this article online, please go to: http://jabfm.org/content/36/1/164.full.
- Received for publication June 16, 2022.
- Revision received September 27, 2022.
- Accepted for publication September 28, 2022.




{kind=link}