
Abstract
Over the past several years, in both clinical and academic medicine, there seems to be a growing consensus that racial/ethnic health inequities result from social, economic and political determinants of health rather than from nonexistent biological markers of race. Simply put, racism is the root cause of inequity, not race. Yet, methods of teaching and practicing medicine have not kept pace with this truth, and many learners and practitioners continue to extrapolate a biological underpinning for race. To achieve systemic change that moves us toward racially/ethnically equitable health outcomes, it is imperative that medical academia implement policies that explicitly hold us accountable to maintain a clear understanding of race as a socio-political construct so that we can conduct research, disseminate scholarly work, teach, and practice clinically with more clarity about race and racism. This short commentary proposes the use of a socioecological framework to help individuals, leadership teams, and institutions consider the implementation of various strategies for interpersonal, community-level, and broad institutional policy changes. This proposed model includes examples of how to address race and racism in academic medicine across different spheres, but also draws attention to the complex interplay across these levels. The model is not intended to be prescriptive, but rather encourages adaptation according to existing institutional differences. This model can be used as a tool to refresh how academic medicine addresses race and, more importantly, normalizes conversations about racism and equity across all framework levels.
In confronting the syndemics1 of our time, where racialized health disparities are magnified by a catastrophic pandemic and the eruption of protests in response to police violence, many academic medical groups are urgently articulating policies to ensure equity and justice in medicine.2⇓–4 Such policies reflect a growing understanding that racial/ethnic health disparities are a result of differences in social, economic and political determinants of health and inequities in power, that significantly or disproportionately impact racial/ethnic communities.5⇓⇓⇓–9 In addition, the phenomenon of “weathering,”10,11 the epigenetically-driven deterioration of health in Black individuals as a consequence of the cumulative impact of social and economic adversity and political marginalization, is clearly implicated in the morbidity and mortality experienced by Black Americans. Scientists have linked biomarkers, including cortisol levels, sympathetic nervous system activity, blood pressure reactivity, cytokine production, and glycohemoglobin levels, to racial discrimination, socioeconomic status, occupation, birth outcomes, and environmental risk.12⇓⇓–15 This reinforces or supports the concept of allostatic load, which is the cumulative wear and tear on the body’s systems resulting from repeated exposure and adaptation to stressors. Simply put, these are the physiologic manifestations of racism, making racism, not race, the fundamental root cause of racial/ethnic health inequities.
Despite the growing acknowledgment in the academic medical community of racism contributing to health disparities in marginalized communities, our current methods of teaching and practicing medicine continue to suggest to learners and patients a biological underpinning to race. For example, medical educators may focus on background epidemiologic data noting that Black women have a significantly higher rate of preterm birth than White women. Without further context, learners may then extrapolate that Black race has a biological basis for preterm birth among Black women in America.16,17 In the clinical setting, patients may see their clinicians input race into algorithms that then determine their 10-year risk for a heart attack or stroke (eg, ASCVD risk estimator18). As a result, clinicians may also inadvertently also teach patients that race is biological, and thus the outcomes, “based on race,” are not modifiable.
To achieve systemic change that moves us toward racially/ethnically equitable health outcomes, it is imperative that medical academia implement policies that explicitly hold us accountable to maintain an appreciation of race as a socio-political construct. It is vital that we are equipped with the knowledge and skills to: (1) contextualize teaching about racial inequities so learners understand that race is often a marker of racism and not a surrogate for biology; (2) critically evaluate race parameters and ‘corrections’ found in medical guidelines and algorithms to promote comprehension for our learners and shared decision making with our patients; and (3) challenge research that utilizes race indiscriminately without clear explanations in study protocols. To effectively teach and practice these recommendations, we need leaders and educators willing to interrogate the foundation of modern academic medicine that has its roots in white supremacy. This interrogation is especially crucial as we seek to increase racial/ethnic diversity among the leadership of our institutions and grapple with the minority tax experienced by the few existing Black, Indigenous, and People of Color (BIPOC—including Latino/a/x, Asian, and other marginalized racial groups) faculty.
A Way Forward
Although there have been many important recommendations challenging and dismantling how currently we think about and use race,19 we propose using a socioecological framework20 (Figure 1) to provide more clarity about the strategies needed at the individual, interpersonal, community, and systemic levels to assure enduring change. This figure not only provides core concepts of how to address race in academic medicine across different spheres but also shows the complex interplay between and necessary dependence across these levels. This approach can be used as a tool to reframe how academic medicine addresses race and, more importantly, normalizes conversations about racism and equity across all framework levels.
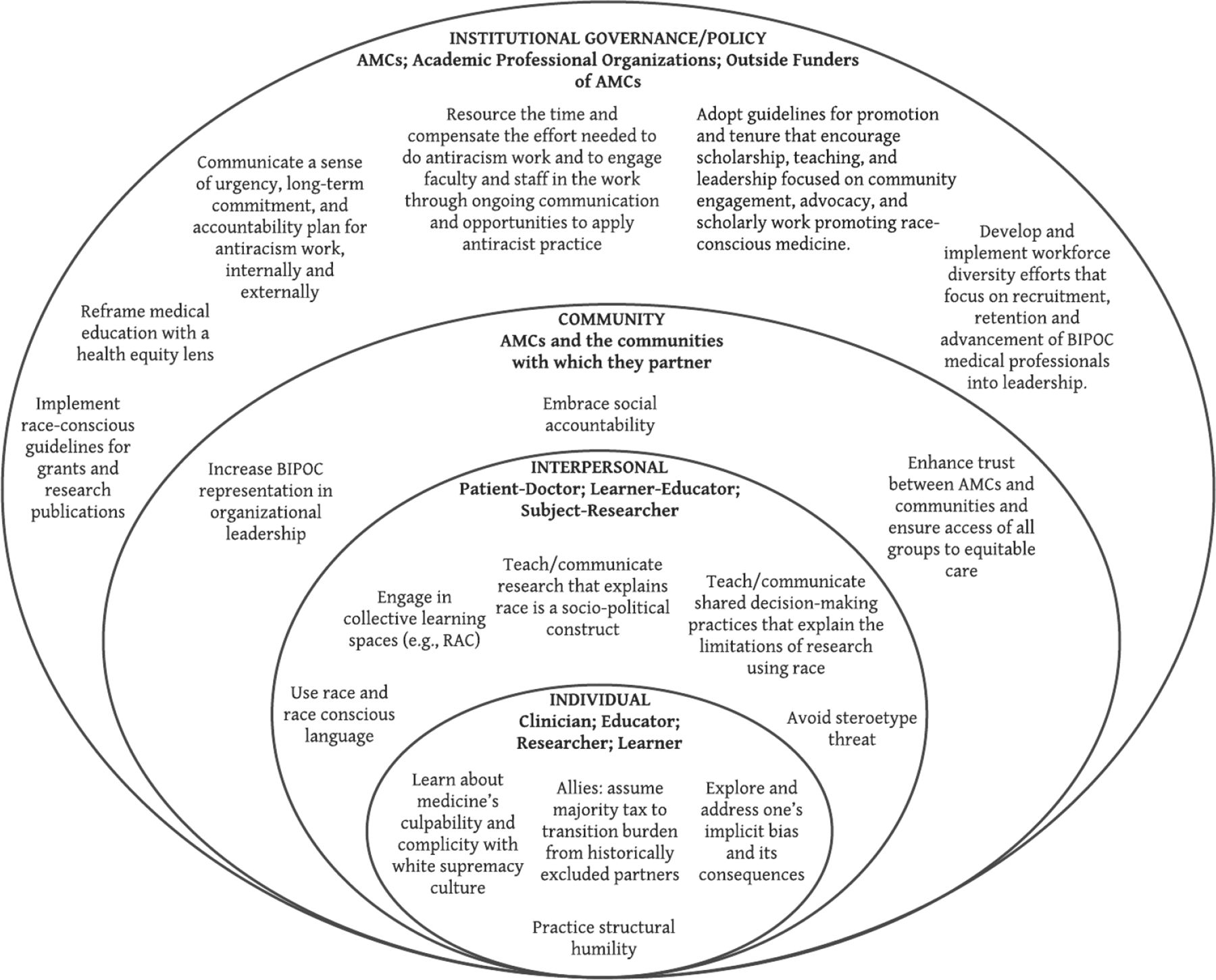
A Socioecological model for addressing race in academic medicine. Abbreviations: AMC, academic medical centers; RAC, racial-affinity caucusing.
Addressing race requires us to address racism and white supremacy. In confronting this classic “wicked problem,”21 disruption requires us to grapple with potential interventions at multiple, interdependent levels with a variety of stakeholders. For example, although policy change is critical, effective change first requires introspective work by individual leaders to identify and prioritize areas for growth. Several tactics are needed for sustained transformational change. We have provided substantive and practical examples in Table 1 for how to begin addressing and dismantling racism in academic medicine. Of note, we recognize that there is no “one size-fits-all” roadmap because institutions are unique or have distinct structures, policies, and practices in place. Thus, each will need its own self-assessment to design a comprehensive plan that is contextualized by the attributes and attitudes of its membership and the culture and climate of its organization. In fact, a multi-pronged, nonlinear approach will likely be most effective with bottom-up grassroots innovations converging with top-down policies. For example, there has been increasing attention to encourage and even mandate implicit bias trainings across institutions, but this strategy alone will not eliminate racism in academic medicine without diverse leaders and voices at decision making tables and adequate compensation and specific promotion guidelines for those engaging in diversity, equity, inclusion, and antiracism work. These latter strategies are especially critical for recruiting and retaining BIPOC faculty who are often expected to lead antiracism efforts while also actively engaging in community-facing advocacy work. It is imperative to address and underscore the need for funding not only individuals and their teams leading and developing antiracism efforts but also for the necessary programming that equips all members of our academic communities to effectively join in advocating for and contributing to these efforts. In addition, mobilizing the skills and expertise of nonmedical stakeholders is equally important. Academic medical centers (AMCs) are often part of larger institutions with enormous capacity for transdisciplinary teaching and learning: historians can contextualize modern medicine with a deep grounding in its past; social scientists can help us better bridge cultures and address social determinants of health; lawyers and economists can also help move our social mission to one of social action; and community organizers can assure advocacy is grounded in the needs and assets of communities. But, although we seek many diverse and interprofessional partners, it will be critical that white allies assume some of the tax currently assumed by many BIPOC clinicians, academicians, and leaders to assure sustainable and actualizable change. White allyship rarely means leading antiracism efforts or health equity research, but rather doing the hard work of learning about white privilege and how to be an effective ally; partnering, supporting, and elevating BIPOC colleagues; and even stepping aside from leadership positions in nondiversity-inclusion-and-equity-focused spaces to enable BIPOC voices and ideas to be heard throughout the health care and academic systems.
Explaining the Socioecological Model for Addressing Race in Academic Medicine
In offering this model, we especially encourage accountability from leaders and power brokers to commit to interventions that can address and eventually eliminate racist clinical, teaching and research practices. The examples we offer are not meant to be prescriptive, but meant to demonstrate the depth of work and investment needed as we strive to confront and eradicate the fallacies that academic medicine has historically held as self-evident. In this way, we can forge a brighter, more just future for learners, clinicians, scholars and, fundamentally, our patients and communities.
Acknowledgments
Our sincere thanks to Sarah Hohl for her deft creation of our figure and to Mindy Smith for her expert review and support. We also thank the countless people of color in academic medicine who struggle to do this work every day and inspire and inform our own thinking and growing in this space.
Notes
This article was externally peer reviewed.
Funding: none.
Conflict of interest: none.
To see this article online, please go to: http://jabfm.org/content/35/6/1239.full.
- Received for publication February 8, 2022.
- Revision received May 23, 2022.
- Revision received June 27, 2022.
- Accepted for publication June 30, 2022.




{kind=link}