
Abstract
Background: Medicolegal dilemmas faced by Sports Medicine providers differ from those of other primary care physicians in type and frequency. Exotic, high-profile challenges are widely covered in the literature and offer guidance on how to navigate challenging situations. However, there is a gap in the literature on how to approach more mundane, but nevertheless common, medicolegal dilemmas.
Purpose: The purpose of this article is to provide Sports Medicine providers simple tools for determining whether a course of action is legal or ethical and offer Sports Medicine educators a model for teaching these skills.
Methods: We searched U.S. federal and state law using the LexisNexis® database for laws regulating Sports Medicine practice, and PubMed for articles related to physician approaches to Sports Medicine legal and ethical challenges. Searches started with the term sports medicine, and included winnowing terms of ethics, ethical practice, ethical guidelines, law, and legal guidelines. We used current ethical practice guidelines followed by the American Medical Association and described in detail by Beauchamp and Childress.
Results: We offer a framework for how to approach legal challenges in Sports Medicine and apply it to four common scenarios that Sports Medicine physicians often face. We further suggest that the profession formally address this literature gap with a standardized curriculum in Sports Medicine law.
Conclusion: A curriculum using this framework and clinical vignettes provides learners and practitioners with familiarity and confidence when legal and ethical challenges arise in Sports Medicine.
Introduction
There Are Few Requirements for Medical Education in Law and Ethics
Medicolegal dilemmas faced by Sports Medicine physicians differ from those of other primary care physicians in type and frequency.1 Education and training in navigating these dilemmas is not standardized in formal education at the medical student, resident, or Sports Medicine fellowship level. The Liaison Committee on Medical Education (LCME) requires “instruction for medical students in medical ethics,” but does not define specific learning objectives and does not require any legal training.2 The Accreditation Council for Graduate Medical Education (ACGME) likewise requires that residency curriculum must contain, “advancement of residents’ knowledge of ethical principles foundational to medical professionalism,” also with no specific learning objectives and no required legal training.3 The ACGME requirements for Sports Medicine requires that fellowship curriculum must contain, “advancement of fellows’ knowledge of ethical principles foundational to medical professionalism,” “an adherence to ethical principles,” and expertise and knowledge in, “ethical principles as applied to exercise and sports” and “medicolegal aspects of exercise and sports.”4 These requirements include legal training, but as with the LCME and ACGME (core) requirements there are no specific learning objectives defined to demonstrate knowledge or expertise in these areas. Similarly, the 2022 ACGME Sports Medicine milestones includes a worksheet specific to professional behavior and ethical principles, but there is an absence of milestones specific to law and its application to Sports Medicine issues.5 It is not surprising therefore that training in and understanding of legal dilemmas are significantly different across programs, and that many practicing physicians and learners are ill-equipped to navigate legally challenging clinical scenarios.6
Recent Sports Medicine Literature in Law Focuses on a Limited Number of Subjects
A PubMed review of Sports Medicine literature and jurisprudence over the past five years suggests that this training void is only partially filled. By far, most articles review the legal, ethical, and practical elements of concussion laws and their health impact.7⇓⇓⇓⇓⇓–13 There are also several articles on gender, hormone and play eligibility;14⇓–16 confidentiality;17⇓⇓–20 cardiovascular care and clearance;21,22 and the broad topic of balancing the competing interests of patient and team.7,23⇓–25
Challenges Absent from Recent Literature
Noticeably absent from the recent literature are articles on the extent to which Good Samaritan laws apply to coverage during a sporting event, limitations to the ability of a team physician to provide care when the team plays in other states and countries, resolution of disagreements between the team physician and other physicians regarding clearance to play, or resolution of conflict between personal team physician practice style and athletic (versus medical) consensus recommendations. Although less exotic topics, they are common in our Sports Medicine fellowship and practice, and, we expect, common to any Sports Medicine practice in the United States. Absent a formal curriculum on how to approach legal challenges, we are left to the apprentice model of teaching, with attendant differing levels of confidence and competence across our Fellows nationwide. As a specialty, we should adopt a formal model of how we approach these dilemmas and make that approach an element of our training. We might further develop curricula based on this approach to provide a homogenous training experience, leading in turn to improved confidence and competence in our graduates.
To address this gap, the objective of this paper is to offer Sports Medicine practitioners simple guides to assess the legality and ethicality of a given action and provide Sports Medicine educators a model for teaching these skills.
Model for Teaching
Illustrate the Question with a Clinical Vignette
Case-based learning is a teaching tool used across medical fields to impart relevance, establish decision-making skills, and help learners connect theory with practice.26 Each question should start with a clinical vignette illustrating how the question arises and options available to the Sports Medicine physician. With available prompts changing key facts, a vignette can be adapted to several learning environments, and be used to briefly teach a core concept emphasizing a practical skill, or, through exploring all the prompts, provide an in-depth review of the topic, including detailed didactic knowledge.
Developing Decision Guides
Evidence of Common Legal and Ethical Standards
To generate decision guides, we searched US federal and state law using the LexisNexis® database for laws regulating Sports Medicine practice, and PubMed for articles related to physician approaches to Sports Medicine legal and ethical challenges. Searches started with the term sports medicine, and included winnowing terms of ethics, ethical practice, ethical guidelines, law, and legal guidelines. We used current ethical practice guidelines followed by the American Medical Association and described in detail by Beauchamp and Childress.
Assess Legality under US Tort Law
Legal questions posed by the vignette are assessed using common elements of US tort law. This ensures relevance across all states, whose laws may differ in technicality, but share a common root. Tort law is the primary legal mechanism underlying legal questions in medicine, including Sports Medicine.1 As with all law and regulation training, individual state chapters and fellowships will need to supplement this general training with specific legal duties unique to their jurisdictions to be complete.
Torts have vague boundaries that make precise definition vexing. In simple terms, a tort is an action which creates civil liability on the part of the actor to remediate the attendant damage caused by the action.27 The academic classification of torts as a distinct area of the law is a relatively novel one. In the words of the authoritative text Prosser and Keeton on the Law of Torts, the definition of tort law is vulnerable to being “…a sort of legal garbage-can to hold what can be put nowhere else…”27 But whereas its scholarly classification relative to other parts of law can be difficult to define, the law governing torts often has common elements that exist in all its permutations in American law.
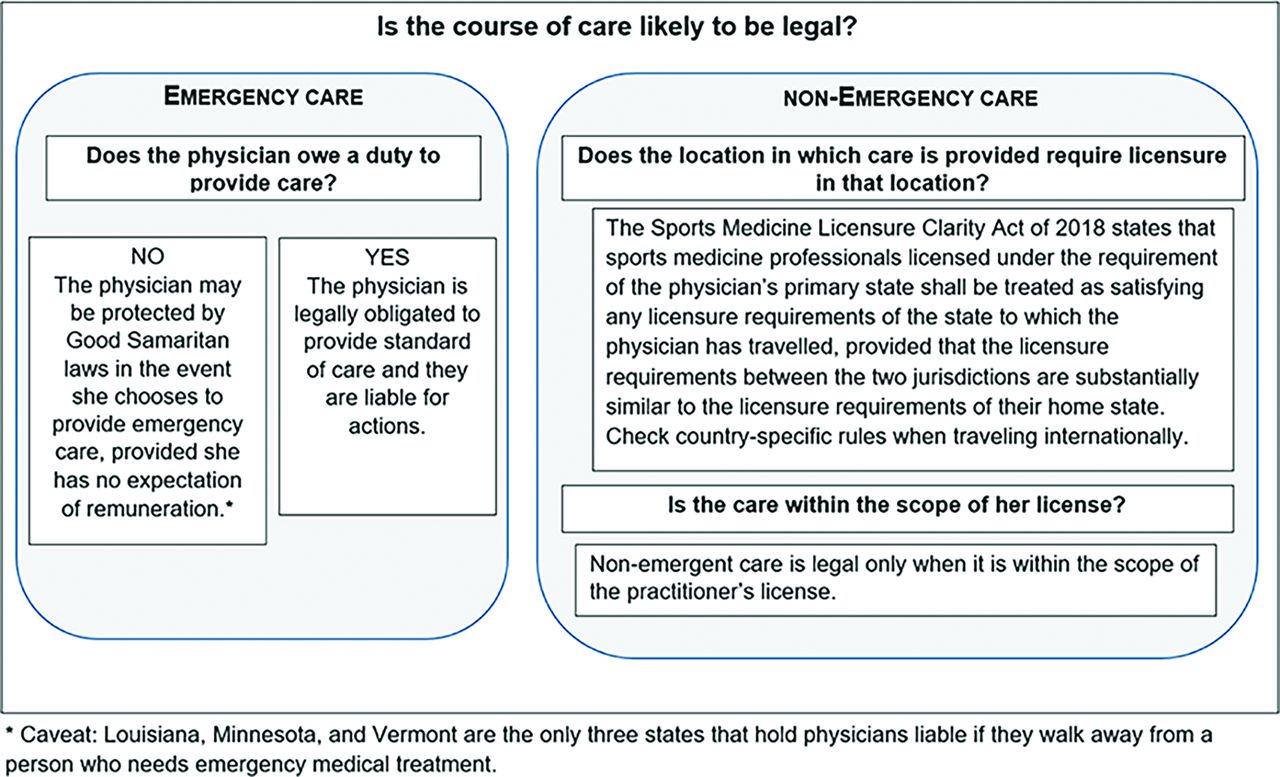
A commonly encountered example in Sports Medicine would be surrounding Good Samaritan laws. Historically, American courts have not imposed a duty to assist those in need of emergency care when a doctor-patient relationship does not exist. Currently, all 50 states have passed Good Samaritan statutes, which, generally, confer immunity from civil liability on various types of rescuers providing emergency care.28 Although these statutes do not impose an affirmative duty on a physician to render emergency aid, they generally curtail the circumstances where liability could be imposed upon physicians who provide emergency aid outside compensated employment.29 Although the precise definitions of what constitutes “emergency care,” “good faith,” and “without compensation” may vary from state to state, they are similar in core meaning. Rendering emergency care “in good faith” is generally used to assign an objective standard to the physician’s belief that an emergency has occurred. Not all jurisdictions define “in good faith,” but looking at how some jurisdictions have clarifies the purpose of this qualification. For example, Hawaii and Pennsylvania have defined “… good faith to include, but not be limited to, ‘a reasonable opinion that the immediacy of the situation is such that the rendering of care should not be postponed.’”30 Most states require that for emergency care to be covered by their Good Samaritan law it must be provided without an expectation of compensation.31 Care delivered that results in a bill for services, or is conditioned on remuneration would therefore not be protected under most Good Samaritan laws, but post-treatment tokens of appreciation (such as a seat upgrade or meal from an airline for emergency services provided on an airline flight), are not expected compensation, and care provided that results in such tokens would remain protected.32 A caveat to relying on Good Samaritan law is that it typically does not apply where the physician has a duty to provide care, such as when treating patients under their care, or providing services contracted (i.e., staffing a medical tent for an organized event indicates a duty to provide care). The jurisdiction where the emergency care is rendered will dictate whether the physician must be a volunteer to secure protections afforded by the Good Samaritan statute. For example, in Virginia, the physician’s status as a volunteer is necessary to obtain the protections afforded by the Good Samaritan statute.28
A flowchart to help assess the legality of an action based on these elements of tort law is shown in Figure 1.

Flowchart to help determine whether an action is legal.
Include a Parallel Ethical Framework
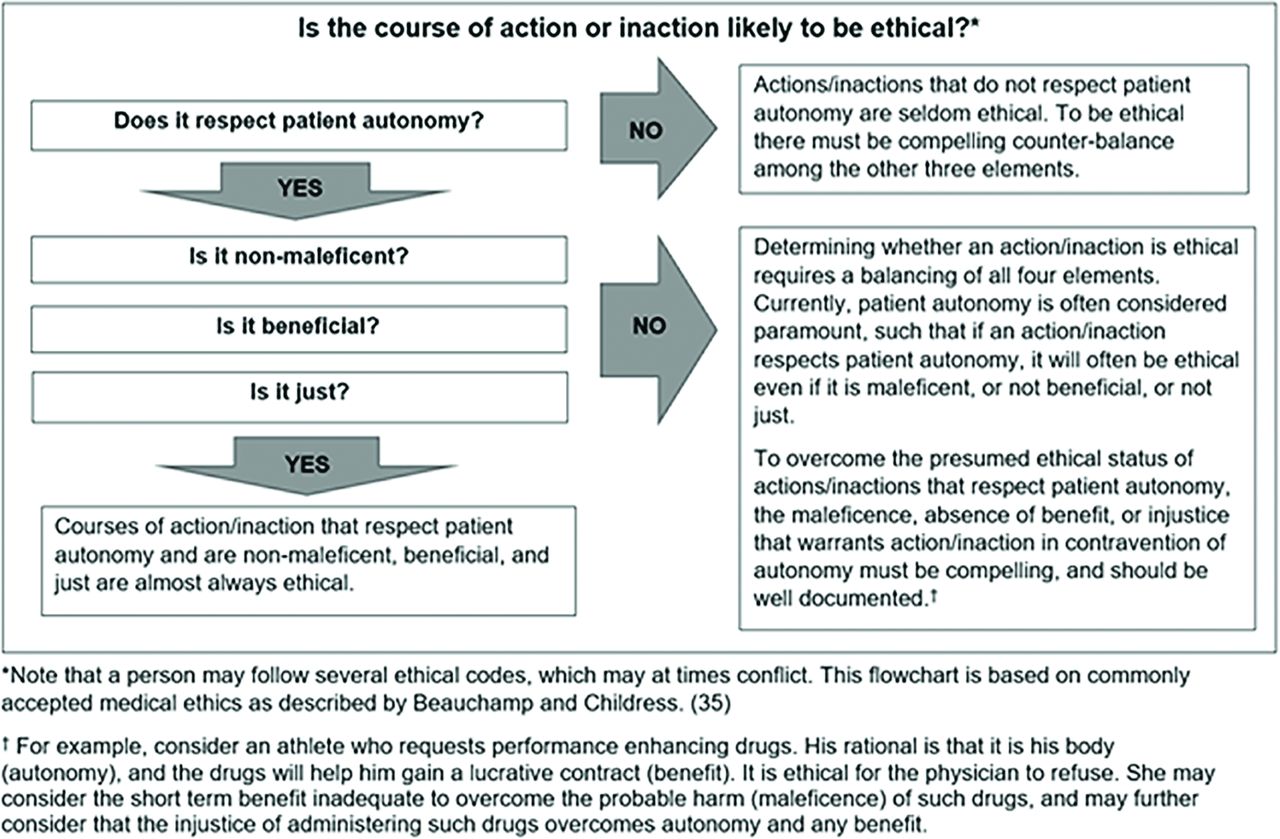
Virtually all scenarios that are legally challenging include an ethical challenge. For this reason, it is appropriate in a model legal framework to include a parallel ethical framework. The American Medical Association Code of Medical Ethics’ opinion on treating athletes clarifies how physicians are expected to balance patient versus team priorities, stating, “The professional responsibility of the physician who serves in a medical capacity at an athletic contest or sporting event is to protect the health and safety of the contestants,” and, “The physician’s judgment should be governed only by medical considerations.”33 This is consistent with Sports Medicine literature,17,23 and fits within the general approach to medical ethics in the United States outlined by Beauchamp and Childress.34 Beauchamp and Childress describe their approach as a framework of four broad moral principles: respect for autonomy, non-maleficence, beneficence, and justice.35 Their framework is drawn from several ethical theories and accommodates modifying priority among these principles depending on competing moral consideration.35 Thus, although patient autonomy is considered the primary principle to uphold, it may be seconded to other principles, for example, to justice in the case of threats to public health.35
In any given scenario, the answer to the question, “Is a given action (or inaction) ethical?” is found by answering principal questions: “does it respect patient autonomy, is it non-maleficent, is it beneficent, and is it just?” with particular attention to autonomy. A flowchart form of this line of inquiry is presented in Figure 2.

Flowchart to help determine whether an action is ethical.
Applying the Models for Case-Based Education
To demonstrate how this approach might look in a curriculum, we will apply it to some unmet challenges described in the Introduction.
First Case
Title: The Good Samaritan in Sports Medicine
Case: A Sports Medicine physician is the team doctor for a Pennsylvania (PA) high school hockey team. She is licensed to practice medicine in PA, and also the adjacent states of Maryland and New Jersey where her team often travels to play. This year, the team was invited to play in Virginia; during the course of that game, a fan behind her bench collapses. Is it legal for her to provide medical assistance to the fan? Is it ethical? Do either of those answers depend on whether she is a volunteer or paid? If the team is professional or amateur? If the person who collapsed was a team member instead of a fan? An opposing team member?
• Is it legal? Was the care emergent? Yes. Was the care administered in good faith? Yes. Did the physician provide the care without compensation? Maybe. The hypothetical case does not specify if the physician is paid or a volunteer. However, regardless of whether she was paid by the PA team for care of those players, she did not receive compensation for providing care to the fan, or other persons not covered by her contract. For these reasons, yes, it is legal for the physician to provide medical assistance to the fan.
• Is it ethical? Does it respect patient autonomy? Yes. Is it non-maleficent? Yes. Is it beneficent? Yes. Is it just? Yes. Providing emergent medical care is ethical; in fact, although physicians are generally free to choose whom they serve, in emergencies, physicians have a positive ethical duty to provide care. This does not mean that they have a legal duty to respond, but most states have Good Samaritan laws in place that protect physicians who render emergency care from civil damages via lawsuits.32 Indeed, physicians only have a legal duty to provide care to current patients, so this case further highlights the important, though sometimes overlapping regions of legal and ethical obligations.
Second Case
Title: The Good Samaritan Overseas
Case: The same Sports Medicine physician is asked to go with the team to play in several other states in which she is not licensed to practice, and then accompany them to exhibition games in Canada and Germany. Is it legal for her to agree to travel to states in which she is not licensed to provide medical care to the team? To other countries? Is it ethical?
• Is it legal? The Sports Medicine Licensure Clarity Act of 2018 states that sports medicine professionals licensed under the requirement of the physician’s primary state shall be treated as satisfying any licensure requirements of the state to which the physician has travelled, provided that the licensure requirements between the two jurisdictions are substantially similar to the licensure requirements of their home state.36 There are some limitations associated with this act. First, the physician must remain within the scope of her licensure in her home state. Second, the physician may not exceed the scope of substantially similar sports medicine professionals licensed in the state to which she has travelled. Reciprocity agreements between states remain unimpacted by this legislation.36 The team physician should consider licensure issues before agreeing to treat the team in international competition. In Canada, the practice of medicine is regulated by provincial and territorial medical regulatory authorities and a temporary license to practice medicine is required.37 In Germany, a travelling team physician must apply for a temporary license to practice medicine, or otherwise must possess a license to practice medicine recognized under the law of the European Union.38
• Is it ethical? Does it respect patient autonomy? Yes. Is it non-maleficent? Yes. Is it beneficent? Yes. Is it just? Yes. It is ethical to provide medical care in states and countries in which she is not licensed. (Note that in the case of other states, there is not a conflict between the ethics of care and the ethics of following the law, as the 2018 Sports Medicine Licensure Clarity Act makes such care lawful.) International medicine, and the ethics involved, is a relatively new field of study and education within medicine. However, given that the team members will have already consented to care from the sports medicine physician, and the governing law asserts that the physician, for all purposes, is practicing in their licensing state, there is no additional ethical consideration to be made for international travel. If the physician was called on to treat a fan, such as in Case 1, or members of the opposite team, then considerations of culture, confidentiality, and consent would need to be further examined, and should be determined before travel to ensure no conflict arises.
Third Case
Title: Conflicts of Interest in Return to Play
Case: The same physician is serving as the medical director for a local soccer tournament. She is also serving as her team’s physician during the tournament. The star player from a different team sustains concussion-like symptoms and is removed from the game early in the day. As the tournament physician, she evaluates the player, deems that the player likely has a concussion, and advises that she should not return to play that day. Later that day the physician’s team is warming up to play the team whose player had been concussed. The physician notices that the concussed athlete is warming up to play. The physician approaches the opposing coach to inquire and is told that they visited a local urgent care clinic and were cleared for participation as the provider at the clinic didn’t think the athlete was concussed. The physician refuses to allow the player to play, as her opinion is that the athlete is concussed. The family argues that the athlete should play, and that they have signed a waiver to free the tournament from liability. Given that the physician’s medical decision impacts the performance of an opposing team, is it ethical that she makes such a recommendation? Does the medical opinion of the tournament physician negate other providers’ opinions for return to play decisions? Could a parent physician clear their child to play? Would a waiver protect the tournament or the physician from liability? How do the wishes of the player (or guardian) change impact these decisions?
• Is it legal? The tournament physician’s duty is to the player.39 If her opinion is that the player is not safe to play, she is not obligated to authorize play. In the event the tournament rules required only “physician clearance,” and not “clearance by the tournament physician,” then as an administrative decision a tournament official could accept the clearance of the urgent care physician; in that case, liability for the medical clearance rests on the physician signing the clearance form. Similarly, if the administrative system allows for a parent to sign a clearance through a waiver, they may allow the player to participate, but this is directly against medical advice, hence the physician would not be liable. Courts have generally invalidated waivers signed by patients that might protect physicians who have provided negligent medical care,39 so the physician should only sign clearances based on her medical judgment, in light of her duty to the patient, and not for administrative convenience or parental desire. No uniform rule dictates whether or under what circumstances parents may be liable to their children for tortious conduct in the United States, so it may be that liability to the physician supersedes a common prohibition against lawsuits against parents by children.30 However, as a general rule, physicians should not treat themselves or members of their immediate families, so although it may be legal for a physician to clear her child, it is not ethical.40
• Is it ethical? Does it respect patient autonomy? Yes. Is it non-maleficent? Yes. Is it beneficent? Yes. Is it just? Yes. Ethically, this is no different than any other return to play condition because it assumes that the physician is acting according to her primary ethical obligation to medical practice. This highlights the importance of physicians maintaining impeccable ethical practice and avoiding even the appearance of conflict. The higher the stakes, the greater the risk of apparent or real ethical conflict in discharging duty to patient versus duty to team.24
Fourth Case
Title: Disagreement over Relative Risk of Play
Case: The same physician approaches player participation conservatively, following more restrictive guidance when evidence is conflicting. A ten-year-old player on her team is found to be heterozygous for causative mutation in the MYBPC3 gene which can cause hypertrophic cardiomyopathy (HCM). This was discovered after the player’s father was diagnosed with HCM and his children were tested. The player himself is phenotypically normal, without HCM or left ventricular outflow obstruction. Based on the most conservative guidelines, developed in the European Union,41 the physician refuses to sign a clearance form allowing the player to engage in team sports. The player’s parents are adamant that the clearance be signed, noting that the American guidelines do not recommend restriction for his condition.42 Is it legal for the physician to refuse to sign a clearance for play? Is it ethical? (When considering the ethicality of this case, pay particular attention to: 1) the relationship between the physician and the patient, and 2) the physician’s medical reasoning.)
• Is it legal? Can the physician refuse to sign a clearance for play without legal liability? Generally, the legal theories upon which an athlete might argue that she was unlawfully deprived of the right to play are based upon the Fourteenth Amendment of the United States Constitution, the Rehabilitation Act of 1973, or the Americans with Disabilities Act of 1990. 46 States may provide additional state-specific remedies available to the athlete.43 Fortunately, Courts are reluctant to second-guess a physician’s determination that a player should not play.44 Further, the deprivation to play stems from the athletic rules, not the physician, so provided the physician is rendering an unbiased medical opinion, she should be protected from liability. The player and parents may choose to find another physician willing to sign the waiver, and then approach the administrative authority requiring physician clearance for permission to play. In this way, the physician following conservative practice is not compromised, and the player also is not penalized.
• Is it ethical? Does it respect patient autonomy? No. Although the physician may not agree with the parents’ decision, the principle of autonomy requires honoring what a patient wants (within bounds), not what a physician believes a patient should want.34 However, it is important to recognize that in this case the physician is not being asked to help the patient make a decision about their healthcare, but rather is being consulted to render an opinion on the safety of return to play. That opinion is independent of the patient’s wishes; in this case, therefore, autonomy would not be a consideration. Is it non-maleficent? The “harm” is not being allowed to play; this perhaps has an emotional harm, and perhaps impedes good health by limiting exercise. Is it beneficent? Maybe, as it may prevent harm from HCM. Is it just? Maybe. Where there is not clear evidence pertaining to practice, clinicians may differ in how they interpret and act on existing literature and guidelines. The physician’s actions may therefore be considered just; she recognizes that there is not great evidence to guide practice, and adopts a conservative approach based on a recognized standard. This does not mean that a physician who signs the form is acting in an unjust manner. The conservative guidelines from the European Union restrict participation for those with “definite diagnosis” of HCM, which the player does not have. Although adolescence has been historically associated with higher mortality for patients with HCM, this player has none of the conventional markers used to identify high-risk patients.45 Furthermore, recent advances in diagnostic, therapeutic, and management options are available for all adverse HCM complications resulting in <1% mortality rate annually for those with the condition,45,46 and the penetrance of disease in genotype positive/phenotype negative patients is low (∼6% in one study).47 For these reasons, a physician might reasonably conclude that signing the form was appropriate. Given these facts, it is likely that an ethics board would deem either action appropriate. A physician choosing to sign the form might mandate proper surveillance of the player and work with the parents to construct an amenable, yet rigorous protocol for future play, stopping conditions, and potentially sharing information with the child’s primary care physician.
Conclusion
Although “medicolegal aspects of exercise and sports” are required in Sports Medicine curricula, there is no specific guidance on how to accomplish this, and no specific learning outcomes of required competence. Recent literature does not provide guidance on several common scenarios that prompt legal questions by Sports Medicine physicians. Our approach is to provide Fellows with a legal framework based on US tort law and a parallel ethical framework to guide their actions. We help them connect theory to practice and gain facility using these frameworks by using clinical vignettes. To help ensure broader competence and confidence in navigating legal questions that arise in the practice of Sports Medicine, future research should include a formal assessment of the most common legal questions presented by Fellows and an online curriculum following our model to systematically address this education and literature gap.
Notes
This article was externally peer reviewed.
Funding: This project received no funding.
Conflict of interest: The authors report no conflicts.
To see this article online, please go to: http://jabfm.org/content/35/6/1230.full.
- Received for publication June 9, 2022.
- Revision received July 21, 2022.
- Accepted for publication July 26, 2022.




{kind=link}
{kind=link}