
Article Figures & Data
Figures
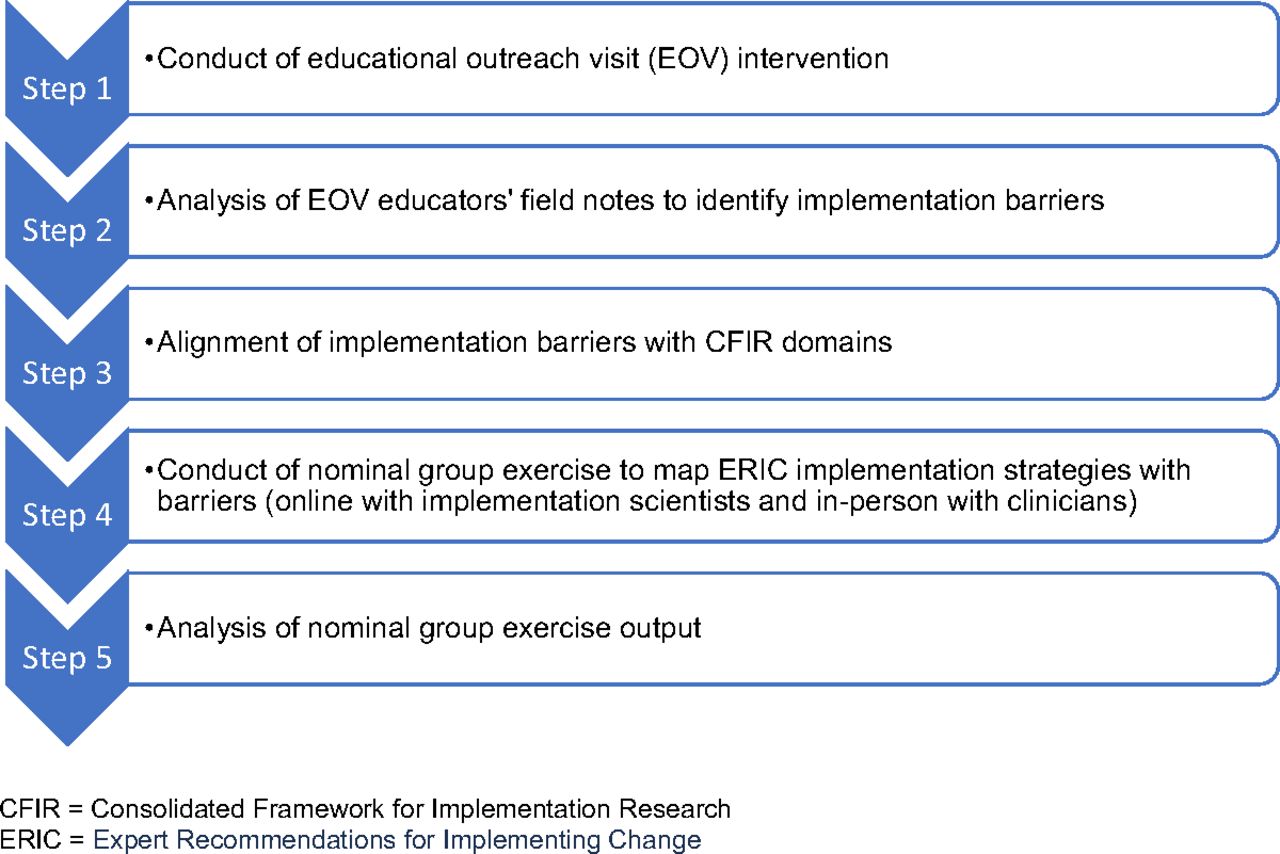
- Figure 1.
Overview of methods supporting this study.
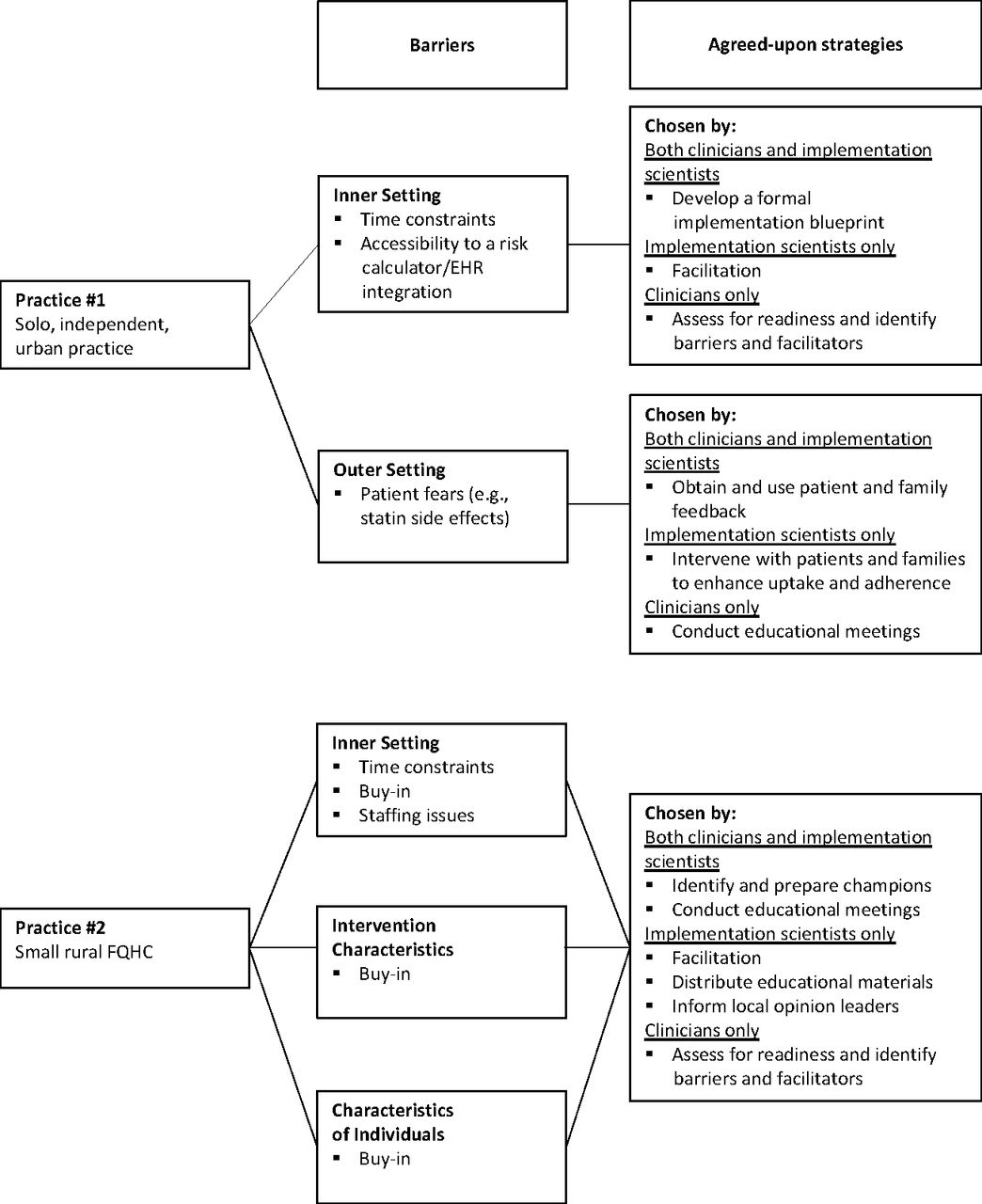
- Figure 2.
Example implementation plans tailored to clinics with different combinations of barriers. Abbreviations: EHR, Electronic Health Record; FQHC, Federally Qualified Health Center.


Tables
- Table 1.
Agreed-Upon ERIC Implementation Strategies for Individual Barriers to Implementing the Cardiovascular Disease Risk Calculator
Barriers to Implementation Subset of ERIC Implementation Strategies Access to Calculator1 Workflow2 Clinical Champion Team Communication Time3 Calculator Training Trust in guidelines4 Patient population5 Patient Fears6 Cost to Patients7 Variations in Calculator Results8 Buy-in Staffing9 Assess for readiness and identify barriers and facilitators C C Develop a formal implementation blueprint IS&C Conduct local needs assessment C C C Obtain and use patients/consumers and family feedback IS&C IS&C Facilitation IS IS IS IS IS IS IS IS IS Provide local technical assistance IS&C C Tailor strategies IS C Promote adaptability IS IS IS&C Use data experts IS IS Identify and prepare champions IS&C C C IS IS IS IS&C IS Organize clinician implementation team meetings IS&C C Recruit, designate, and train for leadership IS Inform local opinion leaders IS IS IS Build a coalition C IS Identify early adopters IS&C IS Conduct local consensus discussions IS IS C IS Capture and share local knowledge IS Model and simulate change IS C IS Visit other sites IS IS Conduct ongoing training C IS Provide ongoing consultation IS Develop educational materials IS IS&C IS Make training dynamic C Distribute educational materials IS IS Conduct educational meetings IS&C C C C IS C Conduct educational outreach visits IS Shadow other experts IS Facilitate relay of clinical data to providers IS IS Revise professional roles IS IS&C Involve patients/consumers and family members IS IS&C IS&C Intervene with patients/consumers to enhance uptake and adherence IS IS Prepare patients/consumers to be active participants C IS IS&C Fund and contract for the clinical innovation C Access new funding IS IS Place innovation on fee for service lists/formularies IS Alter incentive/allowance structures IS Alter patient/consumer fees IS&C Use other payment schemes IS Change record systems IS&C Abbreviations: ERIC, Expert Recommendations for Implementing Change; C, ERIC strategies agreed upon by C only; IS&C, ERIC strategies agreed upon by both implementation scientists (IS) and clinicians (C); IS, ERIC strategies agreed upon by IS only.
1 Accessibility to risk calculator/electronic health record integration.
2 Documented workflow.
3 Time constraints.
4 Trust in guidelines (by clinicians).
5 Patient population (i.e., perceived limited population at risk for cardiovascular disease).
6 Patient fears (e.g., statin side effects).
7 Patient issues with costs of medications.
8 Results vary by calculator.
9 Staffing issues.
- Table 2.
Agreed-Upon ERIC Implementation Strategies for Barriers to Implementation by 5 CFIR Domains
Barriers categorized into CFIR Domains ERIC Strategies Inner Setting1 Outer Setting2 Intervention Characteristic3 Characteristics of Individuals4 Process5 Assess for readiness and identify barriers and facilitators C C C Develop a formal implementation blueprint IS&C IS&C Conduct local needs assessment C C C Obtain and use patients/consumers and family feedback IS&C Facilitation IS IS IS IS IS Provide local technical assistance IS&C C Tailor strategies IS&C Promote adaptability IS&C Use data experts IS IS Identify and prepare champions IS&C IS&C IS&C IS&C Organize clinician implementation team meetings IS&C C Recruit, designate, and train for leadership IS IS Inform local opinion leaders IS IS IS IS Build a coalition IS&C IS IS C Identify early adopters IS&C IS IS&C Conduct local consensus discussions IS IS&C IS Capture and share local knowledge IS Model and simulate change IS&C IS Visit other sites IS Conduct ongoing training IS&C IS Provide ongoing consultation IS IS Develop educational materials IS IS&C IS Make training dynamic C C Distribute educational materials IS IS IS Conduct educational meetings IS&C C IS&C IS&C Conduct educational outreach visits IS IS Shadow other experts IS Facilitate relay of clinical data to providers IS IS Revise professional roles IS&C Involve patients/consumers and family members IS&C IS Intervene with patients/consumers to enhance uptake and adherence IS IS IS IS Prepare patients/consumers to be active participants C IS&C IS Fund and contract for the clinical innovation C Access new funding IS IS Place innovation on fee for service lists/formularies IS Alter incentive/allowance structures IS Alter patient/consumer fees IS&C Use other payment schemes IS Change record systems IS&C Abbreviations: CFIR, Consolidated Framework for Implementation Research; ERIC, Expert Recommendations for Implementing Change; C, ERIC strategies agreed upon by C only; IS&C, ERIC strategies agreed upon by both implementation scientists (IS) and clinicians (C); IS, ERIC strategies agreed upon by IS only.
1 Inner Setting barriers: time constraints, accessibility to risk calculator/electronic health record integration, buy-in, documented workflow, calculator training, staffing issues, clinical champion, team communication.
2 Outer Setting barriers: patient fears (e.g., statin side effects), patient issues with costs of medications.
3 Intervention Characteristics barriers: buy-in, trust in guidelines (by clinicians), patient population (i.e., perceived limited population at risk for cardiovascular disease), results vary by calculator.
4 Characteristics of Individuals barriers: buy-in, calculator training.
5 Process barriers: documented workflow, clinical champion.
- Table 3.
Number of Clinics Reporting Different Types of Barriers Categorized into 5 CFIR Domains
Number of Clinics Barrier Types Categorized into CFIR Domains Inner Setting Outer Setting Intervention Individual Process 7 • • • 5 • • • • 4 • • • • • 4 • • • • 4 • 4 • • 3 • • 2 • • • 2 • • 2 • • • 1 • • • 1 • 1 • 1 • • • 1 • • • • Total: 42 40 18 27 21 17 Abbreviation: CFIR, Consolidated Framework for Implementation Research.
Note: Two clinics reported no barriers.




{kind=link}
{kind=link}